
Executive Summary
In August 2017, Myanmar security forces and Rakhine Buddhist civilians attacked hundreds of villages in northern Rakhine state, massacring thousands of Rohingya Muslim residents and burning their homes to the ground.[1] As of January 2019, that targeted violence and ongoing abuses had prompted approximately 740,000 Rohingya to flee to Bangladesh, where they remain.[2] Physicians for Human Rights (PHR) has collected extensive medical evidence of the human rights violations committed against the Rohingya in those attacks. A PHR report published in July 2018 presented clear medical evidence to corroborate survivors’ accounts of how shootings, beatings, stabbings, and other forms of violence inflicted upon the Rohingya in the village of Chut Pyin made it an emblematic example of the targeted, systematic violence that unfolded in hundreds of other villages across northern Rakhine state.[3]
This supplemental report focuses on a separate, underreported outcome of the August 2017 attacks on the Rohingya: survivors who suffered physical impairments from their wounds that will potentially become long-term disabilities.[4] These disabilities will hinder these survivors’ ease and freedom of movement, limit their ability to seek gainful employment, and otherwise obstruct their ability to live productive, pain-free lives. The plight of these disabled Rohingya survivors highlights how the ruthless violence that the Myanmar security forces and others inflicted on the Rohingya in August 2017 will have a decades-long, painful, life-altering legacy for potentially thousands of survivors and their families.
PHR approached 120 survivors living in refugee camps in Bangladesh to request interviews and interviewed a total of 114 survivors who gave their consent to be interviewed. 90 survivors out of that pool of 114 reported physical injuries resulting from the violence and consented to and subsequently underwent clinical evaluations by PHR medical partners. In total, 43 of these injured survivors were left with long-term disabilities as a result of violence they experienced in or around August 2017.
The vast majority of Rohingya who were disabled as a result of that targeted violence were gunned down as they fled attackers. Many of the bullet wounds have resulted in permanent neurological impairment that limits limb function and causes severe and persistent pain: both can make simple tasks like walking, grasping a pot, or lifting a bag of rice extremely painful or impossible. Other survivors suffered shrapnel wounds from grenades or were injured by landmines laid in fields surrounding Rohingya villages in an apparently deliberate strategy to inflict maximum harm on Rohingya fleeing attack. Some Rohingya survivors who were unable to flee were reportedly seized by Myanmar security forces and brutally beaten, kicked, stabbed, raped, and killed.
The Rohingya profiled in this report are the survivors: unlike the estimated 10,000 killed in the attacks,[5] these people escaped death by being rescued by relatives or by taking refuge in surrounding forests or nearby villages before making the long overland journey to Bangladesh. In many cases documented by PHR, survivors said they had heard that it was unsafe to seek medical treatment inside Myanmar because doctors would allegedly report injured Rohingya to Myanmar authorities. This fear, combined with a longstanding de facto policy of denying health care services to Rohingya meant that survivors often resorted to traditional natural remedies for wound treatment and pain relief during the days- or weeks-long trek to refuge in Bangladesh. PHR clinicians have concluded that this lack of adequate medical attention often exacerbated already severe wounds: these injuries were often worsened by delayed surgery, while infections led to amputations that earlier treatment might have prevented.
The vast majority of Rohingya who were disabled … were gunned down as they fled attackers. Many of the bullet wounds have resulted in permanent neurological impairment that limits limb function and causes severe and persistent pain: both can make simple tasks like walking, grasping a pot, or lifting a bag of rice extremely painful or impossible.
PHR asserts that the attacks by Myanmar security forces should be investigated as crimes against humanity and supports recommendations by a United Nations (UN) fact-finding mission to refer Myanmar to the International Criminal Court or an ad hoc criminal tribunal for accountability for those abuses. PHR is convinced that, by inflicting indiscriminate injury and thus long-term disability on many Rohingya, Myanmar security forces also violated the right to health and the right to work of their Rohingya victims. Myanmar now has forward-looking redress obligations toward Rohingya who were disabled by the 2017 attacks, including guarantees of financial compensation for those who can no longer work; free and comprehensive access to medical services and education; and long-term rehabilitation services for disabled Rohingya if and when the Myanmar government and the international community can guarantee their safe and voluntary return to Myanmar.[6][7]
Muriam’s Story
Five-year-old Muriam Khathu (Profile 5) was at home with her parents and grandparents when soldiers began approaching their village, firing rifles and throwing and firing grenades at some of the Rohingya houses. The family ran out of the house. Soldiers shot and killed Muriam’s father, while several members of Myanmar’s security forces grabbed the 40-pound Muriam and threw her against a wall. They began stomping on her and kicking her with their combat boots, ignoring the pleas of Muriam’s mother and grandparents that they stop.
When Muriam’s assailants moved on, Muriam’s family took shelter in the forest near their village before setting out on the long journey to Bangladesh. They carried Muriam on a makeshift stretcher, but she still cried out in pain every time she was moved. Once in Bangladesh, Muriam was sent to a hospital, but the damage could not be undone: she had suffered a pelvic fracture and serious neurological injury as a result of the attack. She could move her legs only slightly and was unable to walk or bear any weight on them. Months after the attack, she said she still felt pain whenever she moved. According to a clinical examination carried out by PHR medical partners on the ground, the presence of ongoing pain and Muriam’s inability to walk more than two months after the injury indicated a low likelihood that Muriam would ever be able to walk or move without pain.
Members of Myanmar’s security forces grabbed the 40-pound Muriam and threw her against a wall. They began stomping on her and kicking her with their combat boots, ignoring the pleas of Muriam’s mother and grandparents that they stop.… [Today,] Muriam is unable to walk, play, or even sit up.
If Muriam and her family return to northern Rakhine state, many difficulties await. The rural region faces severe food insecurity and its residents are highly dependent on subsistence farming. Muriam will most likely be limited in her ability to work or do the physically demanding chores intrinsic to life in rural Rakhine State. Muriam is unable to play, walk, or even sit up. Her mother is responsible for basic personal hygiene tasks such as helping her use the toilet. Muriam will most likely have extremely limited medical support if she returns to Myanmar: the Rohingya have faced state-sponsored discrimination in accessing health services for years.[8] Even if Myanmar were to end such discriminatory practices, there are fewer than 1,400 hospital beds in Rakhine state to service a population of more than three million people,[9] imposing extremely limited access to services. The lack of adequate support services for people with disabilities in Rakhine state will likely place severe burdens on their caregiver family members. Longtime caregivers of people with disabilities are at high risk of poor health outcomes themselves, including depression and shortened life-expectancy due to the stresses imposed by caregiving.[10]
For those like Muriam whose interviews are documented in this report, the violence directed at them over a period of days in 2017 has resulted in the high likelihood of a lifetime of chronic pain and disability.

Photo: Salahuddin Ahmed for Physicians for Human Rights
Introduction
For centuries, Muslim Rohingya people have lived in Rakhine state on the western coast of Myanmar, a predominantly Buddhist country. Since the Myanmar military junta stripped the Rohingya of citizenship in 1982, the Rohingya have been stateless and subjected to decades of human rights violations, including denial of the right to health and education, limited political participation, restrictions on freedom of movement, forced displacement, arbitrary detentions and killings, forced labor, and trafficking, among other abuses.[11]
Following attacks on Myanmar security forces by the insurgent Arakan Rohingya Salvation Army in October 2016 and again in August 2017, the Myanmar military unleashed a wave of violence on Rohingya communities.[12] PHR’s July 2018 report, “The Chut Pyin Massacre: Forensic Evidence of Violence Against the Rohingya in Myanmar,”[13] detailed the brutal attacks that took place in one village. As the violence was widespread and systematic throughout Rakhine state, Physicians for Human Rights (PHR) conducted a sub-analysis: in a survey of some 604 Rohingya hamlet leaders, 534 (88 percent) reported violence against their hamlets, with more than half of the 534 reporting beatings and shootings, and almost a third reporting rapes or sexual assault.[14] The Myanmar military’s ruthless attacks on Rohingya civilians from August 2017 onward has driven some 740,000 people into neighboring Bangladesh.[15] Evidence gathered by PHR supports the conclusions of a United Nations fact-finding mission, which found that actions by Myanmar security forces indicated “genocidal intent.”[16][17]
To gather the data used in this report, PHR conducted four visits to Bangladesh after October 2017 to interview and carry out clinical examinations of Rohingya survivors of these attacks. PHR interviewed a total of 114 survivors. Of those, 24 people were witnesses who had sustained no injuries and were therefore not given a forensic exam. In total, 90 survivors who had suffered injuries underwent a PHR clinical evaluation consisting of both an interview and a physical exam. Of these survivors, 43 were left with long-term disabilities – defined as physical impairment, activity limitations, and restrictions in participating in activities of daily life – as a result of the attacks.[18] These survivors were from 19 different villages throughout northern Rakhine state.
In September 2018, the UN Fact-Finding Mission (FFM) published a 444-page report about human rights abuses against the Rohingya.[19] The mission’s report concluded that there was evidence warranting criminal prosecution for crimes against humanity, war crimes, and genocide.[20] The report names top military officials as targets for investigation and prosecution and also blames civilian authorities for “spreading false narratives, denying the wrongdoing of the (security forces), blocking independent investigations … and overseeing the destruction of evidence.”[21] The Myanmar government rejected the report’s findings as “false allegations.”[22]
The FFM’s findings were echoed in the results of the first-ever quantitative survey, carried out by PHR, of Rohingya leaders displaced to refugee camps in Bangladesh. The analysis of the survey’s results was published in a March 2019 peer-reviewed Lancet Planetary Health article, which concluded that “in 2017, the Rohingya ethnic minority population of Northern Rakhine State were the targets of a campaign of widespread and systematic violence, including violence by state forces.”[23]
To date, Myanmar authorities have failed to conduct impartial and independent investigations into these events and have not fully cooperated with the UN and other bodies seeking to do so. A four-member commission formed by the Myanmar government to investigate the alleged crimes announced in December 2018 that it had found no evidence to corroborate the UN’s accusations,[24] an assertion roundly rejected by human rights groups.[25] The UN Security Council is currently negotiating a draft resolution to address the Rohingya refugee crisis which would include the option of imposing sanctions on the Myanmar government, though news reports suggest that Russia and China have boycotted that initiative.[26]
PHR is publishing this report based on testimonies and clinical evaluations of individual cases to contribute to documentation and investigation efforts, so that those who perpetrated these crimes can be held accountable and that survivors may be given redress. While this report focuses on the rights of Rohingya survivors disabled in the violence of August 2017 to redress, and, specifically, to access health care and rehabilitative services, this does not discount the need for all people with disabilities in Myanmar to access those same services, especially those who face discriminatory obstacles in accessing health care. Likewise, this report does not discount the rights to reparations of Rohingya who were not injured in the attacks as well as the many survivors who lost loved ones (or entire families), property, and, thus, their economic viability.
Methodology
Field Investigations
Physicians for Human Rights (PHR) conducted four visits to Rohingya refugee camps (Balukhali, Jamtoli, Kutupalong, and Thangkali) near Cox’s Bazar, Bangladesh between October 2017 and July 2018. During an initial visit in October 2017, the PHR clinical team established contact with local health providers working in camps in the area and assessed the need to collect scientific and medical evidence in the form of clinical evaluations. In December 2017, the PHR medical team returned to conduct interviews and clinical examinations of survivors from dozens of villages across Rakhine state, from where most Rohingya have fled since the August 2017 attacks. PHR carried out a second field investigation in Bangladesh in March 2018, and a third in July 2018. PHR then did secondary data extraction to identify evaluations of survivors with disabilities and then conducted an analysis of those particular cases. This report follows the publication of a larger project whose methods and main findings have been previously described in the March 2019 peer-reviewed Lancet Planetary Health article, “Violence and mortality in the Northern Rakhine State of Myanmar, 2017: results of a quantitative survey of surviving community leaders in Bangladesh.”[27]
Interviews and Clinical Examinations
The findings of this report are based on two-part assessments – interviews and clinical examinations – conducted in private locations through a Rohingya language interpreter. The PHR research team collaborated with local organizations, health facilities, and community informants utilizing purposive and snowball sampling to identify survivors with physical injuries from the violence. The PHR research team also interviewed other key informants, including community leaders, medical professionals, activists, lawyers, journalists, and others. All survivors interviewed were adults or accompanied minors who self-identified as Rohingya and who were in surrounding hospitals or lived in refugee camps in the Ukhiya and Teknaf areas south of Cox’s Bazar. PHR excluded anyone who arrived before August 27, 2017 and/or was unable to provide consent.
The PHR team interviewed and evaluated 114 survivors. Twenty-four people were witnesses who had sustained no injuries and who therefore did not undergo a clinical examination. Ninety survivors who had suffered injuries underwent a PHR clinical evaluation consisting of both an interview and a physical exam. Each of these assessments began with a semi-structured interview to collect information on the survivor’s demographics and their personal experiences, as well as when they first noted any disturbances in daily life in late August 2017 and how they arrived in their current location. Questions focused on the survivor’s own experiences and on instances in which they witnessed abuse.
PHR then conducted physical examinations to identify injuries, scars, wounds, and disabilities based on the principles and guidelines of the “Manual on Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment,” commonly known as the Istanbul Protocol. The Protocol is the international standard to assess, investigate, and report alleged instances of torture and other cruel, inhuman, and degrading treatment.[28] This study focused on physical forensic examinations of the area of reported injuries; available diagnostic images, laboratory tests, and other medical records were also reviewed.
Data Extraction and Analysis
PHR investigators attempted to assess disability according to the severity of the impairment and the likelihood that it would constitute a long-lasting impediment to a survivor’s ability to work, do domestic chores, and otherwise live a fully-functional life.
To identify persons with disabilities, a PHR consultant reviewed the 90 evaluations of survivors with injuries. We defined disability as “a restriction or lack (resulting from an impairment) of ability to perform an activity in the manner or within the range considered normal for a human being as defined by the World Health Organization.[29] In this definition, a person qualifies as having a disability if their functional issues fulfill at least one of the following criteria:
- Impairments – The injury causes problems in body function or structure that affect daily life.
- Limitations in Activity – The person has difficulty executing a task or action at least once a day because of the injury.
- Restrictions in Participation – The person is restricted by the injury from involvement in a life situation that would otherwise be available, such as transportation or employment.
Based on WHO criteria, the PHR consultant then classified those people with long-term disabilities. We considered people to have long-term disabilities if they had the disabilities defined above at the time of the assessment and the clinical evaluator mentioned that the disability would likely persist as a long-term disability that would affect the person throughout their lifetime. We excluded psychological and psychosocial disabilities from this analysis. Given that this was a secondary analysis of previously collected data that was not specifically focused on collecting data on long-term disabilities, the consultant reviewed the evaluation documents and any available medical records or diagnostic data; they also consulted relevant clinicians who conducted the clinical evaluations for their assessment of whether survivor injuries and their effects qualified as long-term disabilities, the level of disability, and the impact of the disability on routine activities.
Of the 90 injured Rohingya evaluated by PHR, 43 were left with long-term disabilities as a result of the attacks. These disabled survivors were from 19 different villages throughout northern Rakhine state. The survivors with disabilities included 32 adults (five women and 27 men) and 11 children under the age of 18 (four girls and seven boys).
Consent and Ethics Approval
The PHR researchers obtained consent from each interviewee through an interpreter, following a detailed explanation of PHR’s work, the purpose of the investigation, and its voluntary nature. For reasons of safety and confidentiality, PHR has replaced the names of survivors with pseudonyms and blurred their faces in the images used in this report.
PHR’s Ethics Review Board provided guidance and approved this study based on regulations outlined in Title 45 CFR Part 46, which are used by academic Institutional Review Boards in the United States. All of PHR’s research and investigations involving human subjects are conducted in accordance with the Declaration of Helsinki 2000, a statement of ethical principles for medical research involving human subjects, including research on identifiable human material and data.[30]
PHR Clinical Team
The clinical team involved in field investigations included in this report was composed of six PHR medical experts: Rohini Haar, MD, MPH; Parveen Parmar, MD, MPH; Rupa Patel, MD, MPH; Satu Salonen, MD; Homer Venters, MD, MS; and Karen Wang, MD, MHS.
Limitations
This report sheds light on how multiple attacks on Rohingya living in northern Rakhine state unfolded and provides key forensic evidence on how these attacks had a long-term physical impact on 43 people from 19 separate villages. However, this report does not provide a full analysis of the human rights violations faced by all people from these villages or by the broader Rohingya population. The survivors were interviewed between three and 11 months after the attacks and demonstrated symptoms of trauma, which may have exacerbated recall bias. In addition, given the range of months post-injury at which an individual was interviewed (e.g., some at three months), it would not be possible to determine a definitive diagnosis of permanent disability in all the survivors. We utilize the term “long-term disability” to encompass these disabilities, while acknowledging that rehabilitation services, time, and healing may improve some physical outcomes for some of these survivors.
Definitions of a disability differ, although the WHO describes disability as an “umbrella term, covering impairments, activity limitations, and participation restrictions.”[31] While most definitions of disability include psychosocial impairments, limitations in the field made it impossible for PHR to conduct widespread and in-depth examinations to determine whether survivors suffered psychosocial disabilities as a result of the attacks. However, it is likely that many survivors suffered from post-traumatic stress disorder and other potentially disabling mental health conditions, a phenomenon that has been documented by other humanitarian organizations working with Rohingya survivors in Bangladesh.[32]
Terminology
In this report, the term “Rakhine Buddhist” refers to Buddhist people of Rakhine ethnicity, and “Rohingya” refers to civilian Muslim people of Rohingya ethnicity. “Myanmar security forces” encompasses the military and Border Guard Police officers; the term “Rakhine Buddhist civilians” in this context refers to Rakhine civilians who were armed or appear to have acted in concert with, or at least with acquiescence from, Myanmar authorities during attacks on the Rohingya.[33]
The Rohingya in Myanmar: A Short History[34]
The Rohingya were considered citizens of Myanmar (then “Burma”) under the Constitution of 1948, when the country declared independence after British rule. In 1962, the military junta took over Myanmar, and Myanmar’s Citizenship Act of 1982 fully stripped the Rohingya of their citizenship rights. Myanmar continues to deny citizenship to the Rohingya and to implement discriminatory laws and policies that have led to widespread human rights violations against the Rohingya.[35]
In 2012 and 2013, attacks on Muslim villages uprooted 140,000 Rohingya and made them internally displaced people within Myanmar.[36] In 2014, Myanmar’s first country census in 30 years did not include the Rohingya as a recognized ethnic group and the government initiated a citizenship verification program,[37] whereby the Rohingya were instructed to register as “Bengali.”[38] Many Rohingya resisted doing so for fear of being categorized as “illegal” foreigners. In 2015, a new law was passed requiring that political leaders be citizens of Myanmar, thereby excluding Rohingya from being candidates and from voting.[39] In 2015, the Myanmar government announced that people would be given National Verification Cards (NVCs), but because the process was not transparent and lacked an option to self-identify as Rohingya, many refused the NVC for fear of being registered as “illegal” and expelled from Myanmar. The government increased pressure on the Rohingya to register for the NVC.[40]
In October 2016, the insurgent Arakan Rohingya Solidarity Army (ARSA) attacked three Border Guard Police outposts, killing nine officers. The following day, the Myanmar government declared ARSA “terrorists” and responded with military force, implementing a counterinsurgency campaign. According to the International Organization for Migration, these operations drove an estimated 87,000 Rohingya into Bangladesh between October 2016 and July 2017.[41]
In August 2017, ARSA – armed primarily with knives and homemade bombs – raided 30 police outposts, killing 12 members of Myanmar’s security forces.[42] This was followed by a brutal security crackdown involving arrests, disappearances, beatings, stabbings, mass shootings, rape and sexual violence, looting, and the burning of Rohingya villages.[43] The military has denied responsibility for attacking Rohingya civilians, stating that its offensive was a counterinsurgency campaign focused on ARSA.[44] A UN fact-finding mission used satellite imagery and firsthand accounts to confirm that some 392 villages (40 percent of all settlements in northern Rakhine state) – or nearly 38,000 individual buildings – had been partially or totally destroyed.[45] A separate report by the Public International Law & Policy Group said that the “scale and severity of the attacks and abuses … suggest that the goal was not just to expel, but also to exterminate the Rohingya.”[46] Some 740,000 Rohingya have fled to Bangladesh since the start of the violence in August 2017.
Findings: Disabled by Targeted Violence
The attacks on the Rohingya described by those interviewed for this report followed a similar pattern. Usually in the early morning, when families were at home, Myanmar security forces – sometimes accompanied by groups of Buddhist Rakhine civilians who, in some instances, were armed – entered a Rohingya village. Some Rohingya woke up to the sound of gunfire or shouts. Others saw houses being lit on fire or looted. They saw fellow villagers being rounded up, arrested, beaten, or shot at. Realizing their best chance for survival was to flee to the nearby hills, many attempted to dash out of their homes, often carrying babies, elderly relatives, or the disabled.
Many people were gunned down as they ran. Others stepped on landmines that appeared purposely placed to target fleeing civilians or were hit by shrapnel from rocket launchers or grenades. Some were unable to flee and were brutally beaten after having surrendered to their attackers. Although the systematic gang rape, mutilation, and torture of Rohingya women by Myanmar security forces have been extensively documented elsewhere,[47] only one of the survivors that PHR interviewed for this report elected to recount such incidents herself.
Those who survived were eventually rescued by relatives or managed to take refuge in the surrounding forests, farmlands, or villages. In many cases, local health workers denied survivors necessary medical treatment. Many survivors had heard, directly or indirectly, that Myanmar authorities required doctors to report injured Rohingya to the authorities, thus putting the lives of those injured Rohingya at grave risk. As a result, most survivors interviewed for this report used only herbal remedies for their wounds, or were given bandages, disinfectant, and over-the-counter painkillers from local shops or clinics prior to their arrival in Bangladesh.
Many people were gunned down as they ran. Others stepped on landmines that appeared purposely placed to target fleeing civilians or were hit by shrapnel from rocket launchers or grenades. Some were unable to flee and were brutally beaten after having surrendered to their attackers.
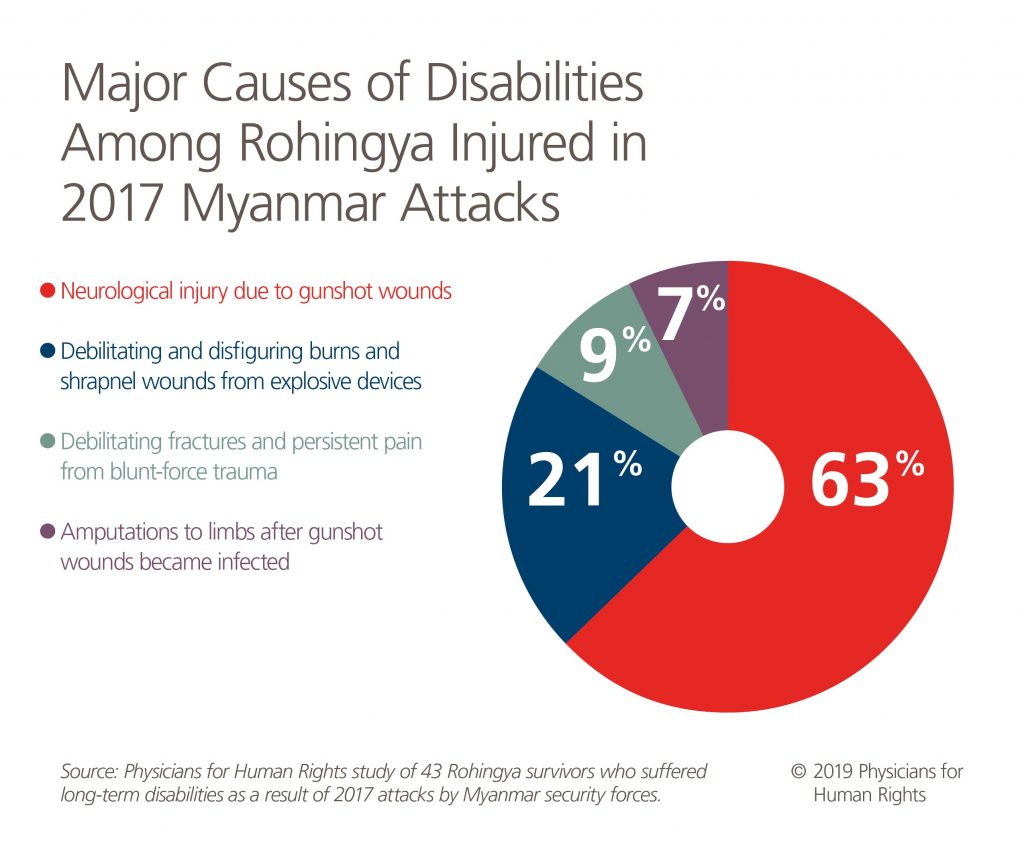
Many survivors now live with physical impairments that will potentially become long-term disabilities. Major causes of disabilities include: neurology injury due to gunshot wounds in 27 out of 43 disabled individuals (63 percent); amputations to limbs after gunshot wounds became infected (three people, or seven percent); debilitating fractures and persistent pain from blunt-force trauma (four people, or nine percent); and debilitating and disfiguring burns and shrapnel wounds from explosive devices (nine people, or 21 percent).
PHR documented significant variance in the type and severity of physical impairments that Rohingya survivors reported. Some survivors could not walk more than a few steps, while others could walk but had pain or a limp and could not remain on their feet for extended periods. Some had lost all use of an arm, while others had lost muscle control in their hands and could not firmly grasp objects. Most of these injuries were likely exacerbated by the lack of immediate medical treatment post-injury, and some examinations indicated a lack of appropriate physical therapy or other rehabilitative services for the affected limb. At the time of writing this report, several organizations in the refugee camps of Bang-ladesh were providing these services, but it was unclear how many Rohingya survivors in need of such services were aware of or had access to them.
Disabilities from Gunshot Wounds
The majority of disabled Rohingya survivors (27/43) examined by PHR medical experts were shot, often while fleeing from the scene of an attack by Myanmar security forces or Buddhist Rakhine civilians. Seven Rohingya examined by PHR medical experts had wounds that were consistent with their testimonies of having been shot from behind while fleeing. Other survivors sustained gunshot wounds when they left an area of relative safety to go back and get an infant or an elderly family member left behind in the epicenter of the attack. Still others were shot while seeking refuge from their attackers – sometimes by Myanmar security forces shooting indiscriminately into areas around Rohingya villages. Those gunshot wounds inflicted permanent neurological damage to the limbs of survivors.
Gunshot wound survivors evaluated by PHR included survivors who had a range of physical disabilities. Three people had lost a majority of function in at least one leg, meaning that they could not walk without crutches or assistance. Six more people had persistent pain and partial loss of nerve functioning, so they could walk only with difficulty and for only a few minutes at a time. Three people had suffered from nerve injury in an arm or a hand – with resulting muscle atrophy, or a wasting away of muscle mass, that results from disuse – while seven others experienced a loss of feeling or sensation in their arms and hands and could no longer do things like hold a pot or a pan or carry their child. Finally, two people had limited motion and chronic pain in their shoulders or neck secondary to gunshot wounds. These disabilities will be a significant impediment in a society in which physical labor is essential to livelihood. “I could work and run normally before. Now I cannot…. People say: ‘He got an injury.’ I feel bad about that – I used to be a normal person,”[48] Uddin said.
Eighteen-year-old Salim Uddin (Profile 18) worked as a farm laborer and lived with his parents, brothers, wife, and son in the village of Chita Para. At about 4 p.m. on a day in late August 2017, Uddin’s family was at home when they saw military personnel shooting at and burning houses. The entire family ran from their home and into the surrounding hills. But Uddin was shot in both legs: “I felt a sharp pain and a hard shake in my body, and I lost consciousness.” Eventually, his father and brothers rescued him and helped carry him to Bangladesh, where he received surgery. He still had difficulty walking and thus working, which made him feel that he no longer belonged. “How can I [farm again]?” he said. “I have to try to do as much as I can, but I can’t hold anything firmly and so I won’t be able to work.”[49]
“I could work and run normally before. Now I cannot…. People say: He got an injury. I feel bad about that – I used to be a normal person.”
Salim Uddin, 18, gunshot injuries to both legs
Faizal Islam (Profile 27) was a 28-year-old farmer who lived with his wife and two children in the village of Pa Da Kah Yua Thit. On August 25, 2017, he saw Myanmar security forces entering the area. Villagers were shot at as they ran. Islam ran with the others and was shot in his left hand, but he was able to hold onto the wound and keep running until he reached the forest, where he stayed for six days before setting out for Bangladesh. Despite receiving immediate medical attention in Bangladesh, he has lost basic motor function in his left hand, rendering him unable to grasp and hold onto objects of any size or weight.

Photo: Salahuddin Ahmed for Physicians for Human Rights
For some survivors, intense, chronic pain from gunshot wounds effectively disabled an injured limb. During an attack around August 25, 2017, Myanmar security forces shot 14-year-old Anowar Hussein (Profile 26) in his right shoulder as he ran to a nearby nut garden to hide. He pretended to be dead, and when the military retreated, he fled to the forest and eventually crossed the border into Bangladesh. When PHR medical experts interviewed him almost a year after the attack, Hussein still suffered from intense, chronic pain that caused him to have a limited range of motion in his shoulders and his right arm, which he could not raise more than 90 degrees. He had previously worked jobs that required physical labor, such as herding cattle.
“I feel bad. It is itchy here at my wound. Sometimes I can’t stand it, the itching and the pain. I can move (my arm) a bit at normal times. But when it becomes very painful, I can’t move at all,”[50] Hussein said.
“I feel bad. It is itchy here at my wound. Sometimes I can’t stand it, the itching and the pain. I can move (my arm) a bit at normal times. But when it becomes very painful, I can’t move at all.”
Anowar Hussein
Amputations Because of Gunshot Wounds
Three of the survivors (3/43 or seven percent) sustained gunshot wounds in limbs that then became infected and had to be amputated. This was likely a result of spending days or weeks hiding from Myanmar security forces without access to adequate medical care.
Mohammed Erfan (Profile 1), a 15-year-old, was at home with nine family members in late August 2017 when security forces and civilians began attacking and arresting Rohingya villagers, looting their homes and then burning them down. Erfan suffered a gunshot wound to his upper left arm as he fled toward the forest. He kept running until he lost consciousness. When he regained consciousness, he was alone and saw that his village had been destroyed. He made his way into the forest and eventually met up with an uncle. They spent two months in the forest, too terrified to leave. Eventually they trekked to Bangladesh, where medical personnel immediately referred Erfan to a hospital to have his arm amputated. Since then, his uncle has been reunited with his wife and children, leaving Erfan alone in the camp. Erfan did not know how he would find work or engage in any other productive activity without his left arm, and he appeared to be suffering extreme trauma and abandonment in addition to his physical disability.

Photo: Salahuddin Ahmed for Physicians for Human Rights
Another patient, 26-year-old Halek Husson (Profile 12) from Mirullah village, had to have an above-the-knee amputation of his left leg after a gunshot wound he suffered became infected. He now walks on crutches and can stand on his right leg for only a few minutes at a time without support. He still felt pain in his left leg after the amputation, mostly at night.
Blunt-Force Trauma
Four survivors (4/43 or nine percent) suffered blunt-force trauma such as beatings or kicking.
This was the only category in which a majority of the victims with disabilities interviewed by PHR (three out of four) were female. As in Muriam’s case, described above, these other two women were unable to escape and were detained by the Myanmar security forces, who subjected them to beatings or other forms of brutality.

Photo: Salahuddin Ahmed for Physicians for Human Rights
Myanmar security forces attacked Bi Bi Zuhra’s (Profile 15) village in the morning of August 30, 2017. Upon seeing soldiers and helicopters, Rohingya civilians fled to the river, but the security forces caught up with them. They rounded up the men and children and killed them with guns and machetes: Zuhra’s husband and five of her six children were killed in front of her. Afterward, she and six other women were taken into a home by force. The men beat her and the other women and broke her wrist. She was then raped by a man who afterwards used a knife to cut her throat in two places and left her for dead. In addition to the severe psychological trauma she endured, Zuhra developed a bony deformity on the end of her forearm that resulted in limited wrist function in that arm.
Burns and Other Injuries from Blast Explosions or Projectile Devices
Nine of the survivors (9/43 or 21 percent) had wounds from explosive devices. Some of them distinctly remembered being shot at by military forces with a rocket launcher or having stepped onto something that exploded under their feet, suggesting that they had stumbled onto landmines that appeared to have been planted as part of an intentional strategy of the Myanmar security forces to kill or injure escaping Rohingya. Others could not specify the type of weapons that had been used to attack them and were only aware that something had exploded close to them.
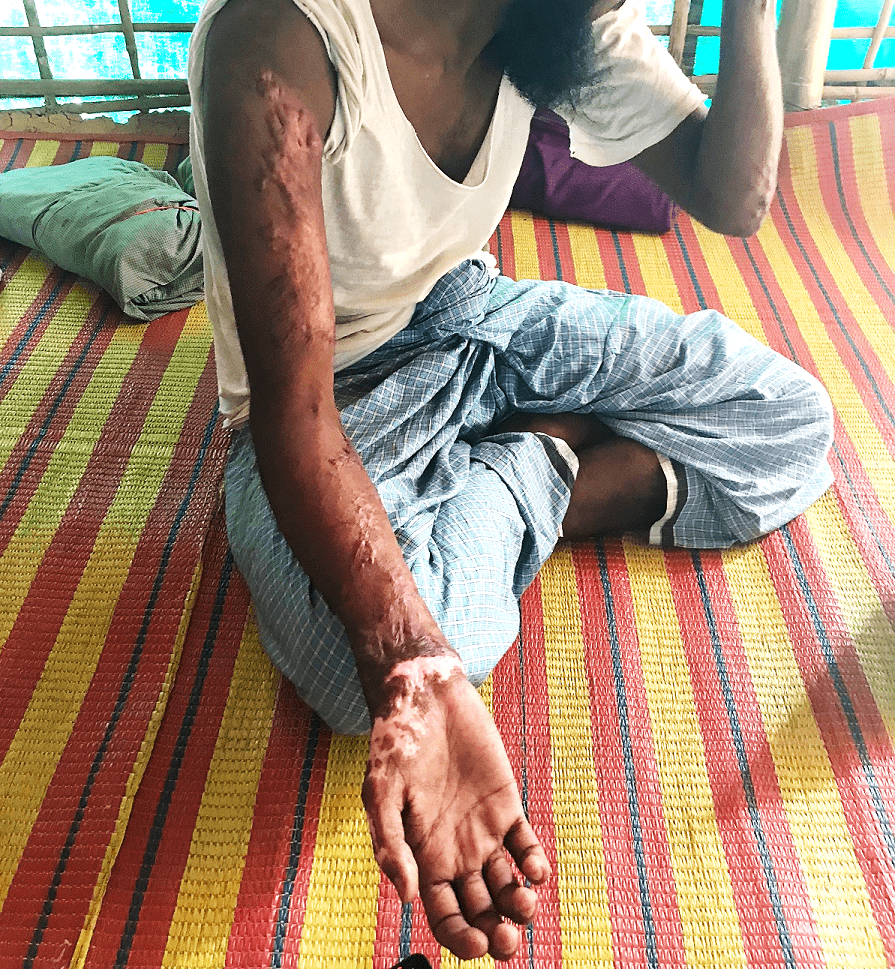
Twenty-five-year-old Monzur Alom (Profile 17) was a teacher at a mosque in the village of Tin May. He was at home asleep with his wife and three children when he heard shooting. He saw military and Border Guard Police, which he recognized by the uniforms they wore, entering the village and shooting guns. He and his family ran out of the house to escape the attack, but Alom turned back when he realized they had left behind his eight-month-old son. He saw Myanmar security forces firing a rocket launcher in the direction of fleeing villagers but made a dash for it with his son held to his chest. Seconds later, something exploded directly in front of him, hitting and instantly killing his son. The explosion inflicted shrapnel wounds and severe burns on Alom. Despite his wounds, he ran until he lost consciousness. Eventually, he was transported to Bangladesh with the help of his family. Extensive scarring to his hands and wrists will make it difficult for him to do any kind of physical labor, as those injuries prevent him from fully flexing or making a fist with his right hand.
Abu Tayub (Profile 25), a 25-year-old farmer from Gu Dar Pyin, was fleeing approaching Myanmar security forces on August 25, 2017 when he was hit by the blast from a landmine. The explosion killed five other fleeing villagers around him and seriously injured his left arm. He hid in the forest for three days before traveling to another village, where somebody helped him bandage his wound. After seven days there, he traveled to Bangladesh, where he was sent to a hospital and received skin grafts. He has lost all function in his left hand, likely rendering him unable to perform many of his previous farming activities. “I used to be a hard laborer,” said Tayub. “I can’t work now, I can’t even lift the small water pot that is used at the latrine…. I feel so sorry that I can’t use my hand anymore.”[51]
“I used to be a hard laborer…. I can’t work now, I can’t even lift the small water pot that is used at the latrine…. I feel so sorry that I can’t use my hand anymore.”
Abu Tayub, 25, landmine injury
Human Rights Analysis
Crimes Against Humanity
The Rome Statute, the treaty which established the International Criminal Court (ICC) and defines core international crimes, enumerates murder, torture, rape and other forms of sexual violence, enforced disappearances, and the forcible transfer of populations as crimes against humanity. The Statute extends the definition of crimes against humanity to “inhumane acts … intentionally causing great suffering, or serious injury to body or to mental or physical health.”
The August 2017 attacks by Myanmar security forces against the country’s Rohingya minority, which left the 43 survivors whose cases are documented in this report – and quite possibly many more – with long-term disabilities, fit this definition.
These crimes have been thoroughly documented by Physicians for Human Rights (PHR) and other credible organizations: 88 percent of the 604 village leaders surveyed by PHR in August 2018 reported violence in their hamlets in or around August 2017, clearly showing that the attacks were widespread and followed notable patterns. Among many other crimes, security forces shot at villagers who were fleeing attack or randomly shot into forests and other places where survivors sought refuge.
PHR’s research demonstrates that the Myanmar military’s actions must be investigated per the Rome Statute or another ad hoc tribunal with jurisdiction to try individuals for serious international crimes, including crimes against humanity and genocide. While Myanmar is not among the 124 nations that are party to the Statute, the Statute allows the United Nations Security Council to refer non-signatories to the court.[52]
Genocide
The Convention on the Prevention and Punishment of the Crime of Genocide (commonly referred to as the “Genocide Convention”),[53] which Myanmar ratified in March 1956,[54] specifically criminalizes acts “committed with intent to destroy, in whole or in part, a national, ethnical, racial or religious group.” The Convention notes that the following acts are punishable: genocide; conspiracy to commit genocide; direct and public incitement to commit genocide; attempt to commit genocide; and complicity in genocide. The crimes committed by Myanmar security forces against the Rohingya and detailed in this report may constitute violations of the Genocide Convention.
Unlawful Use of Landmines
The Convention on the Prohibition of the Use, Stockpiling, Production and Transfer of Anti-Personnel Mines and on Their Destruction, known as the Mine Ban Treaty, to which 164 nations are party, forbids the use of antipersonnel landmines, and further extends this prohibition by banning signatory nations from using, stockpiling, developing, or producing these weapons entirely.[55]
Survivor accounts indicate the possible unlawful use of landmines by Myanmar security forces against Rohingya civilians. Some survivors described seeing, hearing, or being the victims of explosive weapons. Some reported seeing or being hit by a rocket or a grenade, while others had blurred memories and only knew that they had been burned or hit with shrapnel from a nearby explosive. The Myanmar government claims that the Arakan Rohingya Solidarity Army is responsible for placing landmines in Rakhine state, yet numerous reports have documented that the Myanmar military actively placed landmines in the area prior to their attacks on Rohingya villages.[56]
Three survivors, all from the village of Gu Dar Pyin, described surviving or witnessing the use of landmines. Abu Tayub said he had been fleeing the Myanmar forces and running toward the mountains, and when he reached a field outside his hamlet landmines began exploding all around him. He said that five people he was running with died instantly, and that his left hand was injured in the blasts. Mustafa Kamal, a 23-year-old who was severely wounded but not permanently disabled by the attacks, also reported stepping on an object that exploded under his feet, leaving him with a shrapnel wound to his left arm. Rashid Ahmed (Profile 33), a gunshot victim from Gu Dar Pyin, was not hit by a mine himself but said he had seen landmines exploding and saw three people die instantly as a result.
While Myanmar is not a party to the Mine Ban Treaty, its use of landmines is unlawful both in times of conflict and non-conflict, as these weapons do not discriminate between civilians and combatants, thereby affecting a breadth of human rights ranging from the right to life to freedom of movement.
In addition to signing and ratifying the Mine Ban Treaty, Myanmar must guarantee assistance and support for the often extensive rehabilitation that landmine victims require for recovery. The Journal of Conventional Weapons Destruction noted in a 2015 article on landmines in Myanmar that people disabled by landmines are, as a result of their injuries, “poorer than the rest of the community and have a lower level of education. They are also more isolated and less integrated into local society, facing discrimination and stigma,”[57] as is likely to be the case with the survivors included in this report.
Health Services Access Denial
“They [Myanmar security forces] threatened that if they could catch injured people, they would slit their throats.”
Abu Tayub, 25
Myanmar is party to the International Covenant on Economic, Social and Cultural Rights (ICESR), a treaty which requires governments to guarantee the “highest attainable standard of physical and mental health.”[58] This covenant, which the government of Myanmar ratified in 2017, requires states to “ensure the right to access health facilities, goods, and services on a non-discriminatory basis.”[59]
Many survivors of the August 2017 attacks evaluated by PHR reported that they did not have access to medical care, despite facing life-threatening injuries. The lack of timely access to medical services and denial of care constitutes an infringement of the Rohingya’s right to health, as well as a major violation of universally recognized principles of medical ethics.
Several survivors said they had received only rudimentary medical services from local medical clinics with limited resources to treat their injuries, such as wound bandaging and over-the-counter pain med-ications. Many did not get proper medical treatment at all and instead sought treatment from local tra-ditional healers or treated themselves using herbal remedies like turmeric. These remedies were clearly insufficient to treat the life-threatening injuries Rohingya suffered. Several of the survivors said that they had either directly or indirectly heard that medical personnel in Myanmar were compelled to re-port injured people to the Myanmar authorities.
“They [Myanmar security forces] threatened that if they could catch injured people, they would slit their throats,” said Abu Toyub (Profile 25).[60]
As a result of the lack of medical treatment, 17 of the 43 disabled survivors interviewed and physically examined by PHR had to be carried into Bangladesh, while three could walk, but only with assistance. It was only once in Bangladesh that they received adequate medical treatment. Delays in medical attention resulted in overall poor health outcomes, increased complications, including infection, and less recovery of limb function and higher levels of immobility and disability among victims. Two survivors whose wounds became infected while hiding eventually required amputation of their limbs. One gun-shot wound survivor had a recurring limb infection that PHR medical experts suspected was due to an infection that extended from their skin to the bone due to an untreated wound. Bone infections require immediate treatment and months of antibiotic therapy and when inadequately treated often result in permanent limitations in limb movement, changes in sensation in the affected limb, and limb pain. Many survivors also said they still suffered chronic limb pain months after the attacks. Such pain can sometimes result from the delayed or inadequate management of acute pain, wounds (muscle, ligament, nerve, skin, and bone injury), and complications of the original physical injury, such as infections.[61]

Photo: Salahuddin Ahmed for Physicians for Human Rights
As noted above, the Rohingya have long had inadequate and discriminatory access to health care within Myanmar. But the failure to deliver medical care in an emergency situation where an injury is a genuine threat to a person’s life is a major violation of the principles of medical ethics. The World Medical Association, an independent global confederation of medical providers, calls for medical providers to make the health of their patient their first consideration, and not to allow considerations of creed, ethnic origin, or nationality to interfere with their care for patients.[62]
There are indications that discriminatory deprivation of medical services to Rohinyga remaining in Myanmar is worsening, according to reports from aid groups working there. Rohingya have to pay more for treatment, are kept in segregated wards, and even have difficulty obtaining blood donations because of state-sanctioned discrimination against them.[63]
Both the denial of emergency care during the August 2017 attacks as well as ongoing discriminatory access to health care services for the Rohingya in Myanmar constitute serious violations of the right to health.
Deprived of the Ability to Work
“How can I [farm again]? I have to try to do as much as I can, but I can’t hold anything firmly and so I won’t be able to work.”
Abu Tayub, 25, landmine injury
The ICESR also guarantees that all people have the “right of self-determination,” including the right to “freely pursue their economic, social and cultural development.” It also decrees that “in no case may a people be deprived of its own means of subsistence.” This principle is further reinforced by Article 6, which enumerates the right to work, meaning “the right of everyone to the opportunity to gain his living by work which he freely chooses or accepts.” Denial of this right has a ripple effect on a series of other human rights, such as the right to an adequate standard of living.[64]
The Rohingya who remain in Myanmar are already denied this right: the government has continued to target Rohingya by shelling their villages[65] and forcing them to live in camps for internally displaced people, where their freedom of movement and association is highly restricted, depriving them of their ability to pursue a livelihood through farming or other means.[66]

However, even under more hospitable conditions, having a physical disability would make life in rural northern Rakhine state – which was home to all 43 survivors whose stories are recounted in this report – challenging; in a region where farming, fishery, and aquaculture are the main sources of livelihood,[67] amputees or those who no longer have full use of their limbs will clearly be unable to realize their right to work. A survey of four northern Rakhine townships found that 54 percent of households sold crops, livestock, aquaculture, or fishing products in the 12 months before the survey, while casual farm labor accounted for more than a quarter of people’s income.[68] Forty-four percent of people in Rakhine state live below the poverty line, compared to the national average of 26 percent.[69] Subsistence farming is a vital part of everyday life.
Fifteen of 19 survivors who gave information about their or their family’s source of income said they made their money farming, fishing, or doing other types of physical labor. Two survivors were teachers (although one said he also made money by working on the family farm) and two were students. The remaining 24 did not state their source of income.
Given the crucial role of physical labor in the predominantly agricultural economy of rural Myanmar and the purposeful official barriers that the Rohingya face in accessing health services there, these potentially long-term disabilities will change the course not only of the survivors’ lives, but their livelihoods as well. The World Food Programme has noted that while most of Mynamar’s residents struggle to access “sufficient, safe and nutritious food,” people with disabilities face even greater challenges due to “discrimination, including customary laws and traditions.”[70]
A Myanmar government survey published in 2012 revealed that 85 percent of the country’s people with disabilities were unemployed and relied on “casual labor” for their livelihood. As a result, persons with disabilities in Myanmar “are more likely than non-disabled persons to be poor, uneducated, unemployed, to live in poor housing, to be landless, to die prematurely, to have food insecurity, to be unable to access public information, to be excluded from public places, and to be ignorant of their rights.”[71]
The poor employment prospects of disabled Rohingya if and when they have the opportunity for safe and voluntary return to Myanmar are compounded by long-standing barriers to education. Schools are segregated in Rakhine state, and travel bans have prevented Rohingya schoolteachers from accessing government-run teacher training programs, meaning that many Rohingya teachers do not have higher education.[72] This limited and segregated access to education – in and of itself a violation of the right to education guaranteed in the ICESR – has been the status quo for many years.[73] In addition to guaranteeing education, ICESR mandates a right to “technical and vocational guidance and training programs.”[74] Without access to adequate schooling and training programs, Rohingya returnees to Myanmar are unlikely to acquire skills that could help mitigate the impact of their disability on their employment prospects and standard of living.
Disability Rights
The Convention on the Rights of Persons with Disabilities (CRPD) guarantees the rights of disabled people not to be discriminated against, to be actively included in society, and to be guaranteed equal opportunity and accessibility. The CRPD also calls on governments to “promote vocational and professional rehabilitation, job retention and return-to-work programs for persons with disabilities.”[75]
In addition to allowing the independent investigation and prosecution of those responsible for past crimes against the Rohingya, the Myanmar government has forward-looking obligations toward the disabled. As noted above, even able-bodied Rohingya continue to face discrimination in accessing education, health care, and employment opportunities in Rakhine state. If and when the Myanmar government creates the conditions for safe and voluntary return of Rohingya survivors from Bangladesh, disa-bled returnees are likely to face even greater barriers.
Myanmar’s Response
To date, the Myanmar government has denied scrupulously well-documented allegations of widespread and systematic violence by security forces who targeted the Rohingya. It has also blocked international human rights organizations and the United Nations Special Rapporteur on Myanmar, Yanghee Lee, from accessing the country to investigate these allegations. The Myanmar government has also made no public mention of the disabilities inflicted upon thousands of Rohingya by the targeted violence of August 2017. The Myanmar government has also failed to acknowledge its obligation to provide rehabilitation and reparations for disabled Rohingya civilians or to create conditions for their safe and voluntary return.
As of December 2018, the Myanmar government appeared to be cementing segregation by forcing the minority of Rohingya who remain in Myanmar to live in separate and closely monitored camps.[76] Humanitarian aid groups had been banned from providing much-needed food and other assistance to the region[77] and renewed military operations – including the shelling of villages inhabited by civilians – had displaced an additional 5,200 Rohingya in Rakhine state.[78] These operations, in response to alleged attacks by the Arakan Rohingya Solidarity Army (ARSA), have also included official restrictions on the amount of food that Rohingya can transport to their villages due to allegations by military authorities that Rohingya village food stores supply ARSA insurgents.[79]
In September 2018, the UN Independent International Fact-Finding Mission on Myanmar found that the crimes carried out by security forces against the Rohingya in August 2017 should be investigated and prosecuted as genocide, crimes against humanity, and war crimes.[80] In response to these findings, the UN Human Rights Council voted overwhelmingly to extend the mandate of the fact-finding mission so that it could continue gathering evidence for eventual use in criminal proceedings against the Myanmar government.[81] The fact-finding mission recommended that Myanmar be prosecuted by the International Criminal Court (ICC). Though Myanmar is not party to the Rome Statute, which established the ICC, the UN Security Council can refer a non-signatory to the ICC for investigation. However, Russia and China reportedly oppose such proposals.[82] The fact-finding mission also recommended other avenues for prosecuting Myanmar officials, such as an ad hoc international tribunal, and created an independent mechanism “to build on the important work of the Fact-Finding Mission by collecting, consolidating, preserving and analyzing evidence of the most serious crimes and violations of international law committed in Myanmar since 2011.”[83]
Myanmar has refused to cooperate with international attempts to investigate the alleged crimes and has failed to establish truly independent mechanisms to do so within the country. A government-backed commission announced in December 2018 that it had found no evidence to confirm the UN fact-finding mission’s allegations.[84] Eight previous Myanmar-led commissions have failed to find systemic wrongdoing on the part of the security forces,[85] and there is little hope that members of the new council will be impartial. As of January 2019, Myanmar continued to bar entry to UN Special Rapporteur on Myanmar Yanghee Lee.[86]
Myanmar’s refusal to engage with the international community has been reinforced by a crackdown on domestic civil society and media outlets. Two Reuters journalists were arrested for reporting on the massacre of 10 men and boys from a Rohingya village. In September 2018, they were sentenced to seven years in prison. The Myanmar government freed the two journalists on May 7, 2019 after relentless international pressure for their release.[87] The Myanmar government has blocked journalist access to Rakhine state and has denied allegations of human rights abuses confirmed by other media outlets.[88] Most humanitarian organizations have been barred from working in northern Rakhine state.[89] Barring journalists and humanitarian organizations not only harms the civilian population of Rakhine state by depriving them of services, but eliminates potential witnesses to any past or future crimes, leaving civilians even more vulnerable.
In late October 2018, officials from Myanmar and Bangladesh announced an agreement to begin repatriation of Rohingya currently living in Bangladesh back to Myanmar.[90] UN officials condemned the plan,[91] noting that security risks and living conditions for Rohingya within Myanmar are still dire. Many Rohingya inside Myanmar are forced to live in government-run camps for internally displaced persons, where strict travel restrictions and curfews are a daily reality.[92] Plans to relocate the displaced to government housing far from the Rohingya’s native villages have been criticized for attempting to further cement segregation.[93] The government of Bangladesh is pursuing plans to relocate up to 100,000 Rohingya currently in Cox’s Bazar to the nearby uninhabited island of Bhashan Char.[94] UN Special Rapporteur Yanghee Lee in March 2019 publicly questioned “whether the island is truly habitable.”[95]
Conclusion
Based on the accounts in this report of Rohingya women, men, and children suffering severe disabilities as a result of the 2017 attacks by Myanmar security forces, it is clear that Myanmar security forces perpetrated grave human rights violations against the Rohingya, and that Myanmar’s actions should be investigated per the Rome Statute of the International Criminal Court or before other ad hoc tribunals that have jurisdiction to try individuals for serious international crimes, including crimes against humanity and genocide. Additionally, Myanmar should be held to account for other violations of civil and political rights, the right to health, the right to work, and the unlawful use of landmines against civilians.
Moreover, the stories and medical documentation detailed in this supplemental report underscore the importance of enforcing Myanmar’s forward-looking obligations to the Rohingya people. For many years, the Rohingya have been denied the right to citizenship and the right to self-identify as Rohingya, and they have been routinely denied or given discriminatory access to health care services, employment opportunities, and education. This situation continues within Myanmar today, and is bound to confront returnees with long-term disabilities with an even more daunting reality, since their inability to do physical labor will limit their economic prospects.
The Myanmar government is clearly unwilling to investigate, acknowledge, and hold accountable those people responsible for these crimes, or to stop discriminatory practices against the Rohingya. Therefore, international actors must help bring justice to the Rohingya. Among other measures, they must put mechanisms in place to ensure that Rohingya disabled in the attacks receive reparation for the harms they have sustained, and that, wherever they reside, they have the possibility to thrive.
Recommendations
To the United Nations Security Council:
- Implement the recommendations of the UN’s Independent International Fact-Finding Mission on Myanmar, including:
- Investigate and prosecute crimes committed by the Myanmar government by referring the situation to the International Criminal Court, or by creating an ad hoc criminal tribunal;
- Impose an arms embargo against Myanmar until independent international observers certify that the Myanmar government no longer supports or perpetrates gross human rights violations against the Rohingya and other minority groups and vulnerable populations in Myanmar;
- Adopt individual sanctions, including travel bans and asset freezes, against responsible Myanmar officials, including at the highest levels of government and the security forces;
- Support safe, dignified, and voluntary repatriation of refugees only with assurances and international monitoring of safety and individual choice, with explicit human rights protections, including citizenship, for the Rohingya;
- Create a trust fund for victim support, including psychosocial support, legal aid, livelihood support, and other means of assistance.
- Convene a session dedicated to the commission of atrocity crimes in Myanmar, with a specific focus on genocide prevention tools that should guide UN policy toward Myanmar in order to mitigate future risks to Rohingya and other groups in the country.
To United Nations Member States:
- Create an internationally-funded mechanism to provide the resources necessary for sustained treatment, rehabilitation, and vocational training for Rohingya victims physically disabled in the 2017 attacks.
- UN member states who are party to the 1948 Convention on the Prevention and Punishment of the Crime of Genocide (“Genocide Convention”) and who have already recognized the crimes against the Rohingya as genocide – including Canada and Malaysia – should file complaints to the International Court of Justice (ICJ) for the Myanmar government’s violation of the Genocide Convention and press the ICJ to seek reparations.
To the United Nations Special Rapporteur on Disability and the UN Division for Social Policy and Development, which oversees enforcement of the Covenant for the Rights of People with Disabilities:
- Support the creation of a systematic assessment of the Rohingya population disabled in the Au-gust 2017 violence in order to triage the most serious cases for immediate treatment and for longer-term rehabilitation and vocational training with transition to economic dependence, and psychosocial support of those individuals.
- Urge the government of Bangladesh and UN member states supporting Bangladesh’s humanitarian support for Rohingya refugees to respect their obligations under Article 11 of the Convention on the Rights of Persons with Disabilities, which requires state parties to “ensure the protection and safety of persons with disabilities in situations of risk, including situations of armed conflict, humanitarian emergencies, and the occurrence of natural disasters.”
- Urge only safe, dignified, and voluntary repatriation of refugees, including those Rohingya with dis-abilities, and only with assurances and international monitoring of safety and individual choice, with explicit human rights protections, including citizenship, for the Rohingya, in line with Article 15 of the Convention on the Rights of Persons with Disabilities, which requires state parties to “take all effective legislative, administrative, judicial or other measures to prevent persons with disabili-ties, on an equal basis with others, from being subjected to torture or cruel, inhuman or degrading treatment or punishment.”
- Urge UN member states supporting international accountability efforts for Rohingya victims and survivors of the August 2017 violence to respect their obligations under Article 13 of the Convention on the Rights of Persons with Disabilities, which requires states to “ensure effective access to justice for persons with disabilities on an equal basis with others.”
- Urge the government of Bangladesh and UN member states supporting Bangladesh’s humanitarian support for Rohingya refugees to respect their obligations under Article 16 of the Convention on the Rights of Persons with Disabilities, which requires state parties to “take all appropriate measures to promote the physical, cognitive and psychological recovery, rehabilitation and social reintegration of persons who become victims of any form of exploitation, violence or abuses, including through the provision of protective services.”
To the Government of Myanmar:
- Cease segregation of and human rights violations and discrimination against the Rohingya people.
- Appoint an independent third party to investigate and prosecute human rights violations and crimes against humanity committed during the August 2017 attacks as well as other violations committed against the Rohingya and other religious and ethnic minorities in Myanmar.
- Grant access to United Nations officials, agencies, and other international organizations to investi-gate human rights violations in Myanmar, particularly in Rakhine state.
- Provide assistance to all Rohingya people with disabilities, including those disabled in the violence of August 2017, including:
- Creation of a trust fund or other financial mechanism to provide sustained support to those who were injured in the August 2017 attacks and are unable to achieve financial independence as a result;
- Provision of funding for free and comprehensive long-term access to health care and rehabilitative services, with the explicit aim of promoting vocational and professional rehabilitation; and
- Creation of return-to-work programs designed for people with disabilities, and full access to and promotion of educational opportunities for the disabled.
- Guarantee safe, dignified, and voluntary repatriation of Rohingya refugees by explicitly protecting their human rights, including with guarantees of citizenship.
To the Governments of the European Union and the United States:
- Expand existing financial sanctions against the Myanmar government and military, and specifically link the lifting of those sanctions to measurable benchmarks, including the end of human rights violations, discrimination, and segregation targeting the Rohingya and to cooperation with international mechanisms for accountability.
- Expand visa bans and asset freezes to include all senior Myanmar security officials for whom the United Nations Fact-Finding Mission and domestic and international human rights organiza-tions have compiled convincing evidence of those officials’ complicity in grave rights violations against the Rohingya people.
- Impose broader trade sanctions on specific industries within Myanmar, including the loss of tariff-free access to European Union (EU) markets by revoking Myanmar’s EU trade access via the “Everything But Arms” agreement of the Generalised Scheme of Preferences.
- Impose foreign investment bans on businesses with proven close links to the Myanmar military.
- Support resolutions in national and international fora to protect Rohingya refugees from forced repatriation, and to ensure the safe, dignified, and voluntary return of displaced persons. Maintain or expand current suspensions on military relations between Myanmar and the EU or the United States, and specifically condition the full resumption of military relations on specific human rights and accountability benchmarks, including those referenced and recommended in this report.
Profiles
Profile 1: Mohammad Erfan, a 15-year-old male
- Impairment: Gunshot wound resulting in amputation of arm. Treatment delayed due to violence.
- Disability: Unable to perform basic tasks, including manual labor in an agricultural setting without a prosthesis.
In late August 2017, Mohammad Erfan was at home with nine family members in the mid-afternoon when security forces and Rakhine Buddhist civilians surrounded his village. The civilians entered homes and looted valuables. Anyone who resisted or ran away was attacked by security forces, who then began burning down homes.
Erfan ran into the forest with his family and was shot in the left upper arm. He recalled running for a bit and then fainting. When he regained consciousness, he couldn’t see anyone and his village had been destroyed. He had not seen his parents since, but found an uncle and two siblings in the forest near his village. They spent two months there, too afraid to leave, but eventually they traveled to Bangladesh. Erfan had no treatment for his arm and was unable to move it. He had severe pain, but no fever or signs of infection during those two months.
At the border, Erfan was referred straight to the hospital where his left arm was amputated, leaving a stump. He still suffered from itching and ghost limb sensations. His uncle had found his wife and children and had gone to stay with them, leaving Erfan alone in the camp. At the time of the interview, he thought he would be able to leave the hospital soon but did not know how he would find work or do anything without his arm.
PHR Medical Evaluation
Erfan had a total left upper extremity amputation with good granulation (re-growing) tissue around a still open 4 cm area at the stump. Otherwise, the wound was clean, dry, and intact. A review of medical records included labs and chest X-ray which were all unremarkable and a simple surgical report indicating he had an amputation but not noting the reason it was needed.
Profile 2: Fozol Korim, a 28-year-old male
- Impairment: Gunshot wound resulting in bone fracture, nerve injury, rotator cuff tear and limited ability to lift and move arms. Treatment delayed due to violence/incorrectly treated.
- Disability: Unable to perform basic tasks, including holding his newborn child.
One night in September 2017 at around 4 a.m., Fozol Korim heard gun shots in his village of Mirullah. He went outside and saw Myanmar security forces about 500 meters away firing weapons. On the other side of the road, security forces were trying to surround the village and were burning houses. He woke his wife and four children and they ran into the forest.
At around 8 a.m., the security forces started firing randomly into the forest, knowing villagers were hiding nearby. Korim’s nephew was shot in the chest and died immediately. His cousin was shot in the back of the head and died immediately. Korim was shot in the left upper back area. He fell, losing blood and feeling weak. The family carried him for more than four days to Bangladesh.
He went immediately to a hospital where little was done for him. An X-ray showed a broken bone. Korim still could not lift any weight with his left arm and felt very weak. He had a newborn child, who he couldn’t carry in that arm. He had persistent aching chest pain and fatigue.
PHR Medical Evaluation
Korim’s exam was consistent with his narrative. His weakness was obviously visible and represented a more than superficial injury to the limb’s bone, nerves, and muscles, which includes a rotator cuff tear.
Korim had an entry and exit bullet wound in the left upper back just over the superior scapula (shoulder bone). The entry wound is about 1.5 cm and circular. The exit wound is oval-shaped with the medial (middle) area appearing with a scab and an extended lateral oval area, consistent with a bullet injury. The scab area, according to the patient, is very itchy and he scratches it regularly. He had no history of bone or soft tissue infection or pus draining from the limb. The wound appeared clean, dry, and intact and was forming a small scab. He had no pain when examining the wound by the examiner’s hands or no tenderness to palpation. His scapula (shoulder bone) and clavicle (collar bone) appeared intact.
Korim had significantly limited range of motion and could not lift his left arm above his head and has limited posterior (backward) movement, a severe limitation that constitutes a disability (per WHO definitions).[96] The length of time since the initial injury, coupled with the lack of progress made over time, classifies this as a long-term, and likely permanent, disability.
Profile 3: Abdul Wahid, a 6-year-old male
- Impairment: Gunshot resulting in leg injuries, causing inability to walk without a limp or run. Treatment delayed due to violence.
- Disability: Unable to perform basic tasks including walking and rice farming.
Abdul Wahid’s family were rice farmers in the village of Morikorum. Wahid’s father said the Rohingya had experienced increasing persecution and had not been allowed to leave their town to buy things. On September 3, 2017, after already hearing that the military was attacking all nearby Muslim villages, the family saw Rakhine Buddhist civilians and security forces entering the village. They ran in the forest and walked for two days, when they heard gunshots nearby. Wahid was hit in the left leg, but nobody else in the group was hit.
Wahid remembered being shot but then fainted. His father carried him another two days through the forest to Bangladesh. Wahid was bleeding from several wounds in his scalp and on the left side of his leg, buttocks, and back. His leg was shattered. In Bangladesh, he had surgery and spent a month in the hospital before returning to the camp on crutches. He could walk independently but had a limp and could not run.
PHR Medical Evaluation
(Patient’s) wounds were significant and consistent with the manner of injury described in the history, specifically a projectile injury, either from a shotgun or ricochet of bullet fragments.
Wahid had several scars over his left leg, hip, and buttocks and on his scalp that appeared a few months old. He had a valgus deformity (bone angled away from leg) on his left leg and walked with a limp. He had a 3 cm stellate burst (star-shaped) scar with an 8 cm surgical wound superior to (above) it over the anterior (front) left mid-shaft of the leg. He also had similarly aged wounds of 0.5 to 2 cm over the right superior tibia area (top of lower part of leg) and the medial (middle) aspect of the right knee. He also had a 0.3 cm right frontal scalp wound just past the hairline. He had two wounds to the left buttock consistent with a projectile injury (circular) and a 3.5 cm by 0.75 cm healed wound just superior to (above) the penis in the groin area.
Profile 4: Mohammad Eliyas, a 20-year-old male
- Impairment: Explosive blast resulting in deformities of left eye, loss of fingertips, and other hand injuries. Treatment delayed due to violence/untreated.
- Disability: Difficulty with any basic tasks with his hand, including gripping and loss of sight.
Mohammad Eliyas reported that his village, Landha Khali, was attacked on August 27, 2017 by Myanmar security forces. He was at home with 11 family members. As he heard shouting outside, Eliyas was hit by something hot and heard a loud explosion at the top of his house. He reported falling to the ground and being confused. He then recalled being picked up by his family and helped out of the house. At that time, he had pain in his right hand and left eye and also in his arms and chest. He could not see from his left eye thereafter. His house was full of smoke and flames, and smoke and flames were coming from other houses as well. His family led him out of the village and they walked to Bangladesh, which took two days.
Eliyas was sent to the hospital for his hand injuries, but no surgery was possible, and he had not seen medical staff about his eye. He reported that he could only see light and dark from his left eye, not shapes or colors. He also reported constant tearing which got worse if he went out during the day.
PHR Medical Evaluation

Eliyas’s physical examination revealed numerous injuries that are highly consistent with his account of blast injuries secondary to an explosive/incendiary device being detonated in or on his home. The injuries to his right hand revealed a traumatic loss of bone and skin that was imprecise and resulted in varying degrees of damage to his fingers. The multiple scars on Eliyas’s hands, arms, and chest were also consistent with multiple fragments from various types of materials impacting his body all at the same time.

Eliyas’s left eye revealed blurring of the perimeter of the iris from the 2 o’clock to 10 o’clock positions. This blurring included a loss of border between the sclera and iris and also included a brown ring of pigmentation. The sclera was injected (reddened) in the inferior half of the eye and the pupil appeared largely opacified and the border between the iris and pupil was not apparent.
Eliyas’s right hand revealed damage to the tips of his fingers and thumb. His thumb was grossly deformed from the interphalangeal joint distally (end joint). The bone of the distal phalanx was palpable under the palmar surface of the thumb, with bone extending to the tip of the thumb, but also at 90 de-gree angle toward the thumb pad. The thumb nail was largely absent and heaped up scar tissue was present on the dorsal surface of the thumb’s distal phalanx. Eliyas’s third (middle) finger revealed total loss of the distal phalanx with scar tissue growing around the distal aspect of the proximal phalanx (end of the first joint). Eliyas’s right wrist revealed a curving linear scar of 4 cm that extended from the mid-line of the wrist to the lateral aspect, well approximated. His left hand revealed a 0.5 cm linear scar well approximated near the base of the index finger on the palmar aspect.
His thorax revealed two parallel raised and irregular scars, approximately 0.5 and 1 cm in length located approximately 2 cm lateral to the right clavicular notch of the sternum.
Profile 5: Muriam Khathu, a 5-year-old female
- Impairment: Sustained pelvic fracture with nerve injuries from being thrown against a wall, kicked, and stomped on. Has ongoing pain and is unable to move legs or bear weight on them. She was untreated after the incident.
- Disability: Unable to walk or stand, resulting in the inability to perform basic tasks independently, which her mother now must do for her.
According to an account provided by her mother, Muriam Khathu was in her house with her mother, father and both grandparents on the day their village was attacked, sometime in September 2017. Security forces approached the village and began firing their rifles and throwing grenades at some of the homes. Khathu’s mother stated that their house was burned down but did not specify how it was set alight.
When the attack started, Khathu and her family ran out of their house. Her father was shot and killed by security forces. Once outside, a member of the security forces grabbed Khathu (who appears to weigh about 40 pounds) and threw her against a wall. That man and three other members of the security forces then began to kick and stomp on her with combat boots. Khathu’s mother reported that this physical attack lasted several minutes, during which she and Khathu’s grandparents pleaded with the security forces to stop. Khathu’s mother reported that she picked up the child when the security forces stopped and ran away from the house with the grandparents. They carried Khathu to Bangladesh on a makeshift stretcher. Khathu cried every time they moved her for many weeks.
PHR Medical Evaluation

Photo: Salahuddin Ahmed for Physicians for Human Rights
Khathu appeared to suffer from a pelvic fracture with nerve injuries. Her current physical limitations are consistent with her mother’s account of pelvic and abdominal blunt force trauma. It appears that her injuries have gone essentially untreated. Her ongoing pain and inability to walk or bear weight two months after her injury indicated a poor prospect for physical recovery. During the exam, Khathu did not appear to move her lower limbs spontaneously. When asked about her ability to move her legs, Khathu responded that she could move them “only a little” but that she could not bend her legs, let alone stand or bear weight on them.
Khathu’s mother stated that Khathu’s pain had diminished but that her daughter had pain whenever she moved and that she could not stand or walk. Khathu’s mother was responsible for all of her daily needs.
Profile 6: Ali Huson, a 45-year-old male
- Impairment: Gunshot wound resulting in bullet lodged in knee and fractures of the fibula and tibia. Treatment delayed due to violence.
- Disability: Unable to walk.
Ali Huson stated that he was at home with his family in the village of Dunz Para sometime in October 2017 when security forces entered his village and began firing rocket-propelled grenades at houses. His house was surrounded by security forces with rifles. He and his family fled on foot, but as he was run-ning Huson was hit in the left lower leg and fell. His family helped him up and carried him away. Huson was unable to walk during the journey to Bangladesh but his family carried him using a makeshift stretcher. He was taken directly to the hospital upon arrival in Bangladesh.
PHR Medical Evaluation
Huson’s injuries were consistent with his report of being shot with a rifle while fleeing. The presence of a bullet in his knee was fully consistent with an entry point from behind, with total destruction of the fibula and complete and displaced fracture of the tibia.
Huson’s inability to bear weight, persisting point tenderness, and X-ray showing only repair of the tibia suggested that fibula repair would be more complicated. An X-ray of Huson’s right lower leg showed that the fibula was shattered in numerous pieces just below the head of the fibula. The tibia was also fractured. A fully intact bullet could be seen still lodged in the soft tissue of the knee. A subsequent x-ray showed a surgically repaired tibia with rods and screws but not a repaired fibula. Upon examination, the front of Huson’s right knee had a surgical scar approximately 22 cm in length. The surgical wound appears to be healing well, with no signs of infection or re-opening. Huson had no pain during the physical exam of the knee and a 2 cm hard object can be felt under his skin on his right knee cap. He has a healing, irregular 2×2 cm wound on the back of his lower leg. He reports that he is unable to walk or bear weight on his leg.
Profile 7: Fozol Ahmed, a 35-year-old male
- Impairment: Beating of both legs with rifle butts resulting in multiple displaced fractures, subsequent leg deformities and shortening of the right leg, and extensive soft tissue damage with bruising and scarring.
- Disability: Unable to walk without pain and difficulty walking due to different lengths and thicknesses of legs caused by the injuries.
Fozol Ahmed reported that his village was attacked sometime in October 2017. He fled with his family after security forces attacked his home with rocket-propelled grenades. He reported that he was approximately 500 meters from his house when the security forces stopped him and several others. The security forces tied their hands with rope while the others continued to flee.
Ahmed reported that once his hands were bound, four or five security force members took turns striking him with rifle butts. Ahmed reported being on the ground during the assault with his hands tied behind his back, trying to roll away from the blows but being held in place. He reported being struck several times on his legs and back, causing extreme pain. He pleaded with the security forces not to kill him and promised that if they did not kill him, he would flee to Bangladesh and never come back. Ahmed reported that, as soon as he said this, the security forces stopped beating him and pushed him into a field. They beat other men in the same manner.
PHR Medical Evaluation
Ahmed’s injuries to his legs were consistent with his account of being beaten with rifle butts. The presence of skin wounds combined with displaced fractures to the long bones of his leg are characteristic of being struck with a rifle butt. Ahmed appeared to require repair of his femur and profound swelling of the right thigh likely represents a combination of bruising and soft tissue injuries.
Ahmed’s right leg appeared grossly shorter than the left. He shared several X-rays which showed dis-placed fractures of his bilateral tibias as well as a right femoral fracture. On physical examination, Ahmed’s left leg revealed a 20 cm surgical wound, healing well, along the middle of his lower leg. His left leg also had a 7 cm irregular, linear wound in the early stages of granulation tissue (growing new tissue) on the front of his shin. Ahmed’s right leg was noticeable for a grossly swollen thigh, approximately twice the circumference of his left thigh. His right thigh was swollen and tender to the touch but not warm. A 6 cm irregular, linear scar was present on the side of his thigh, healing with granulation tissue present.
Ahmed reported that his right thigh has been painful since the injury, but that the pain was now “only when [he] moved.” On physical examination, his right leg revealed a 22 cm surgical scar, healing well, along the middle of his lower leg.

Photo: Salahuddin Ahmed for Physicians for Human Rights
Profile 8: Abdu Goffar, 18-year-old male
- Impairment: Shrapnel from explosive detonation resulting in metal being lodged in left eye and ear and a 6 cm-deep hole into skull through left ear. Treatment delayed due to violence.
- Disability: Unable to hear and see on left side; unable to feel due to facial nerve loss; difficulty with basic communication as a result of sight and hearing loss.
Abdu Goffar reported that around 5:30 p.m. on a Friday in August 2017, he was walking home from school with other students in his village of Thombajur-Kundpara when approximately 10-15 security forces armed with guns began shooting. Goffar reported feeling a fire and explosion on the left side of his face and head, and he fell into a field. Two other students were shot, one in the arm and another in the leg. Goffar lost hearing on the left side and had diminished vision in his left eye.
Goffar’s brother said that Goffar’s friends brought him back to the village. Goffar was not awake. That evening they fled. Goffar was unable to walk and was carried by his family into the forest, where they hid for about three days with other villagers. While in hiding, he saw a fire where the school had been located. Goffar’s brother said that Goffar had several pieces of metal lodged in his left eye and ear and that there was a lot of blood all over the left side of his face. He described a hole in Goffar’s ear and said he was able to stick his index finger into this hole, and estimated the depth to be about 6 cm. When he did so, he felt something hard beneath his finger. The family walked about one day to Bangladesh and Goffar was taken to a hospital, where he stayed for two months.
PHR Medical Evaluation
Goffar’s physical examination revealed a linear scar that is consistent with the temporal (temple) area craniotomy (surgical opening of skull) for removal of bone fragments. He had numerous scars consistent with a penetrating injury to his left ear. The multiple small scars on his face and ear were consistent with lacerations caused by impact of a sharp foreign body. His loss of facial nerve function and visual loss were highly consistent with an intracranial injury in the area of his left ear.
On inspection of Goffar’s face at rest, no gross asymmetries were noted. Extraocular motions (eye muscle movements) were grossly normal. Goffar had a dysfunction of the cranial nerve in distribution of the left cranial nerve VII (facial nerve), with asymmetry noted with weakness in wrinkling the brow, show-ing teeth, frowning, and an inability to close the left eye tightly.

Photo: Salahuddin Ahmed for Physicians for Human Rights
On visual inspection of the left ear, Goffar had several, well-healed hypopigmented (lightened) scars of less than 5 mm linear along the antihelix (visible curved cartilage). His auditory canal was closed-over with flesh-colored skin. On inspection of the posterior (rear) of the ear, Goffar had a small flesh-colored nodule approximately 5 mm in diameter. He had a well-healed, hypopigmented linear scar approximately 1 cm anterior, inferior to the tragus (external part) of his left ear that runs superior to (above) his hairline. It is approximately 7 cm in length. There were approximately six hypopigmented linear scars bisecting the aforementioned scars at intervals approximately 1 cm apart. Inferior (below) lateral to his lower eyelid, he had a small depression of his skin.
Goffar’s left pupil had minimal reactivity to light, with afferent pupillary defect (minimized constriction of pupil) on the left, increasing from approximately 2 mm to 3 mm. His vision was grossly tested on left – with inability to identify two fingers held at a distance of 24 inches from his face. On examination of peripheral vision, Goffar was able to see an object at 45 degrees from the sagittal (midline) plane on the left side, and 90 degrees on the right side from the sagittal plane.
Profile 9: Saif Rafman, 22-year-old male
- Impairment: Gunshot wound resulting in the inability to use left leg. Treatment delayed due to violence.
- Disability: Unable to walk without crutches.
Saif Rafman reported that his village of Mirullah was attacked sometime in late 2017. He reported that he was at home sleeping, was awakened by the sound of guns, and came out of his house. He saw a couple hundred security forces and was immediately shot twice. One bullet hit him in the front of his right thigh and went through to the back; another bullet hit him in the back of his left thigh and came out of the front. He lost consciousness.
Rafman’s brother and a friend carried him to the forest, where he regained consciousness. They hid in the forest and along roads for seven days while making their way to Bangladesh. During this period, they saw many dead and injured people. In Bangladesh, he was seen at an MSF (Médecins Sans Fron-tières) hospital where he received surgery on both of his injuries and received both IV and oral medications.
Rafman reported having an iron rod inserted into his left thigh. The long surgical wound on the left thigh took about four months to recover. He reported that the left thigh injury still occasionally bleeds. His right hip had not gotten better. He could not use his left leg at all. He could not put any weight on this leg and it was very stiff. He used crutches to walk.
PHR Medical Evaluation
Rafman’s injuries were highly consistent with gunshot wounds to his right hip and to the back of his left thigh that have been medically and surgically treated. The length of time of recovery needed for this left thigh surgical wound seemed longer than normal and was concerning. The lack of range of motion and limited strength of his left leg were highly consistent with inactivity and lack of physical therapy post-injury. His left leg had visible muscle atrophy compared to the right. Measured difference of the circumference of the calf two inches from the base of the patella (kneecap) was more than 1 cm.
The anterior (front) of the left thigh had a nearly healed semi-linear, raised, hypertrophic (enlarged) and keloid (raised) surgical scar 13 cm in length over his femur. There were visible, well-healed suture scars bisecting the surgical scar. The proximal (close end) and distal (far end) parts of the surgical would were well-healed. In the middle of this surgical wound, there was visible granulated (growing) tissue that was moist and was contiguous with an oval lesion that was 4 cm in length and 3.5 cm in width with irregular borders. This wound had whitish granulated tissue forming, and it was moist with clear fluid at the medial (middle) aspect of the scar that is contiguous with the surgical scar.

Photo: Salahuddin Ahmed for Physicians for Human Rights
On the lateral (outside) left thigh, there was a well-healed surgical scar 15 cm in length, the most proximal end (nearest) of the wound is contracted, forming an indentation.
He also had two scars distal to the left (away from) the lateral surgical scar, approximately 1.5 cm in length by 1 cm in width which are hyperpigmented (darkened). He had one scar proximal (near) to his lateral left thigh scar which is 1.5 cm by 1.5 cm.
Rafman could not actively raise his left leg from the ground and could not move side to side. With assistance he could minimally flex and rotate his hip. With assistance he could flex and extend his left knee but his range of motion was limited and his strength was decreased. His right hip and leg strength and range of motion seemed to be within normal limits.
Profile 10: Mohammad Esouf, 19-year-old male
- Impairment: Gunshot injuries resulting in limited use of right arm and hand, inability to use right fingers, atrophied left arm, and abdominal injury. Treatment delayed due to violence.
- Disability: Difficulty with any basic task involving prolonged walking or use of right hand.
Mohammad Esouf reported that security forces came to his village of Rajabill in the early morning hours of August 22, 2017. He was a student at the madrassa and was praying in the mosque when he heard gunshots. He ran back to his house. While running, he was shot twice. One bullet entered the middle surface of his arm near the elbow and exited his right elbow, and the other hit the left side of his abdomen. His father and brother helped carry him to the river and sheltered him in the forest for four days.
Esouf said the security forces stayed near his village for five to six days. One doctor came to him in the forest and gave him liquid to pour on his wounds, wrapped his wounds with cloth, and gave him some tablets. Esouf’s family left for Bangladesh and walked for ten days. Upon arrival, he was sent to an MSF (Médecins Sans Frontières) hospital, where he received surgery on both his right arm and abdomen. He stayed in the hospital for four months.
PHR Medical Evaluation
Esouf’s physical exam findings were highly consistent with his testimony. Esouf’s right forearm had visible atrophy compared to the left: its circumference was 4 cm less than the left forearm at the widest part of the forearm.
On the right arm, around the region of the ulna/medial epicondyle (ligament attachment) there was a 7.5 cm well-healed, rope-like scar from the medial epicondyle area to the upper arm, medially (in the middle). It was a hyperpigmented (darkened), hypertrophic (enlarged) scar and keloid (raised scar) formation. Some areas of the scar were purplish in color, and the 1-2 cm keloid formation extends medially from the main scar to the triceps region.
On the right arm, dorsal (underside) surface, lateral to the elbow joint was a well-healed, serpentine, surgical keloid formation, 7 cm long by 2 cm wide. Approximately five well-healed suture scars were visible, bisecting the surgical scar. On the right foreman, ulnar (elbow) side, was a raised circular scab about 1 cm long.
Esouf could externally/internally rotate his right elbow with difficulty. The digits of his right hand could not extend and were permanently contracted as compared to his left hand.
Esouf also had two visible scars on his abdomen. He had minimal pain after prolonged walking. His right arm took about four months to recover and he still had occasional bleeding from an area with a scab. He cannot use his right hand or arm very well.



Photos: Salahuddin Ahmed for Physicians for Human Rights
Profile 11: Zoko Reah, 33-year-old male
- Impairment: Gunshot injury resulting in amputation of right thumb and limited range of motion in right hand and inability to make a fist. Treatment delayed due to violence.
- Disability: Difficulty with any basic tasks involving use of right hand.
Zoko Reah reported one day in late 2017, he and others were having tea in his village of Arobshapada when security forces stopped in front of his shop. He saw two military buses full of security forces. They started firing and Reah, along with 10-15 others, ran away. Reah was running with his hands closed in fists and was shot in the right hand. The bullet entered near the base of his thumb and exited between his first and second fingers. He lost consciousness. He was carried by others for two days until reaching Bangladesh.
When he arrived at the hospital, his thumb was black. Medical personnel amputated his right thumb and placed three rods in [his right hand] It took approximately three months for his right hand to heal, and he reports that he still cannot move right hand fully as he could before the injury.
PHR Medical Evaluation
Reah’s physical findings on this hand, digits, and nail plates were highly consistent with his report of a gunshot to his right hand and the medical treatment he received. His limited range of motion in his right hand is consistent with the location of the injury, lack of use and lack of physical therapy. He also has signs of diminished perfusion (blood flow) to the amputated digit.
Reah’s right hand had an area along the phalanxes (finger bones) that were hyperpigmented (dark), dusky appearing compared to his left hand.
He had an amputation of the right thumb, above the interphalangeal joint. The skin on the tip of the remaining distal phalanx (bone) of the thumb was shiny, atrophied and had darkened areas. The stump tip had three small wounds, 2-3 mm long, that appeared to be scabbing.
Reah had a linear scar, 9 cm in length, from the palm of his right hand, running medially to the thenar eminence (base of thumb) that ran to the dorsal (back) right hand, medial to the first digit metacarpal bone. The scar was hyperpigmented (darkened) on the palmar surface, and hypopigmented (lightened) along the dorsal surface, with three to four visible bisecting liner scars, 1 cm in length, resembling suture scars.

Photo: Salahuddin Ahmed for Physicians for Human Rights
He had another prominent scar, on the dorsum (back) of the third digit proximal phalanx (finger bone), approximately 5 cm in length. It was contracted, hypopigmented (lightened) and its shape varied from almost linear (dorsum) to irregular borders (along lateral side of the third proximal phalanx). His fingernails of the second and third digits were irregular. The second digit nail plate was hypertrophic (enlarged), disfigured and discolored. The third digit nail plate had a transverse depression at the distal (far end) portion. He had decreased flexion of the digits of the right hand, with limited mobility of the distal (far end) and proximal (near end) interphalangeal joints of his second and third digits, and inter-phalangeal and metacarpal joint of his first digit. With his right hand, Reah could not make a fist.
Profile 12: Halek Husson, 26-year-old male
- Impairment: Gunshot injuries resulting in amputation of left leg, right leg injury, and bullet lodged in right shoulder. Treatment delayed due to violence.
- Disability: Difficulty with any basic task involving standing or walking.
Halek Husson was awakened by gunshots in his village of Mirullah one morning around 6 a.m. He came out of his house and saw 150-200 security forces. He started running away from his house. He was shot twice. One bullet hit his left leg, penetrating through and hitting his right thigh, while the other hit his upper right chest. He fell to the ground.
Husson’s brother carried him to the forest, where he saw many others injured like him. They traveled for six days to Bangladesh, and during that time he received no treatment. His leg was “black” all the way to his mid-thigh. In Bangladesh, he was referred directly to Chittagong hospital, where he stayed for about one month and had an above-the-knee amputation of the left leg.
Husson reported that it took about three months for the surgical wound to recover. He returned to the camp after one month. After returning to the camp, doctors removed the bullet that had penetrated his right upper chest and was lodged in his right shoulder area. He walks with crutches. He can stand on his right leg for a few minutes without the support of the crutches. He felt pain in his left leg after the above-the-knee amputation, mostly at night, but not every night.
PHR Medical Evaluation
Husson’s physical findings of his left thigh amputation, right thigh scar and right axillary (armpit) scar were highly consistent with his report of two gunshot wounds and the treatment that he received at the hospital.

Photo: Salahuddin Ahmed for Physicians for Human Rights
He had a 2.5 cm long by 1 cm wide hyperpigmented (dark), hypertrophic (enlarged) scar in the region of the right arm/shoulder, in the area of anterior axillary (armpit) fold. Within the mid-axilla (armpit), Hussan had another scar, 2.5 cm by 1.5 cm, with irregular borders, discolored compared to other axillary skin. The scar was contracted and had no hair growth. These two scars were separated by approximately 4 cm.
There was a well-healed 17 cm scar across the stump of the amputated leg. The stump had no obvious swelling or deformity or pain upon palpation (touching) of the scar. In the right inner thigh, he had a scar that was 1 cm wide and 1.5 cm long. The scar was contracted and hyperpigmented (dark).
Profile 13: Shahid Usman, 23-year-old male
- Impairment: Gunshot injury to lower right leg resulting in inability to bear weight and walk normally and subsequent leg infection while fleeing. Treatment delayed due to violence.
- Disability: Difficulty with any basic tasks involving use of legs; cannot walk for more than 10-15 feet.
Shahid Usman stated that on the day of the attacks in his village of Mirullah, more than 100 security forces units arrived in trucks and drove down the main road of the village. They first burned the madrassa, then the market, and then homes. They used rocket launchers to set fire to homes, and shot at fleeing villagers.
Usman fled east to a paddy field and was shot in the right lower leg while running. He fell and was found by his uncles, who carried him to a nearby village to receive basic treatment including bandaging and some kind of injection. They decided to flee to Bangladesh. Usman was unable to walk and was carried by his uncles. They saw many burned homes, mosques, and vehicles along the way. En route, Usman’s leg became infected. Usman and his family arrived in Bangladesh and presented themselves at an MSF (Médecins Sans Frontières) clinic on August 31, 2017.
Usman was stabilized when he had arrived at the MSF Clinic, given food and clothing, and then sent to Chittagong Medical College (CMC) where he had surgery on his leg with an external rod attached. He also had a skin graft from his thigh to his shin.
PHR Medical Evaluation
Usman’s physical exam was highly consistent with his story of being shot while fleeing, with an entry point anteriorly (to the front) and exit wound posterolaterally (to the back and lateral) resulting in an open fracture and skin damage that became infected, requiring antibiotics for a prolonged period of time, surgery, and skin grafting. The patient may have a chronic bone infection that may result in inadequate healing at the site of the surgery. This is corroborated by recurrent infections and continued pain when walking, despite the surgery having been done five months prior to the evaluation.
Usman continued to use crutches and could only walk 10-15 feet. He continued to have severe pain and could not bear full weight on his injured leg. His leg had been warm, but had improved with antibiotics. He still had itching at the site of the scar on his leg. The site of his surgical scar and the site where the skin graft was taken appeared well-healed. There was a bulge protruding from the skin graft an there is a small ulceration with some yellow discharge on this examination
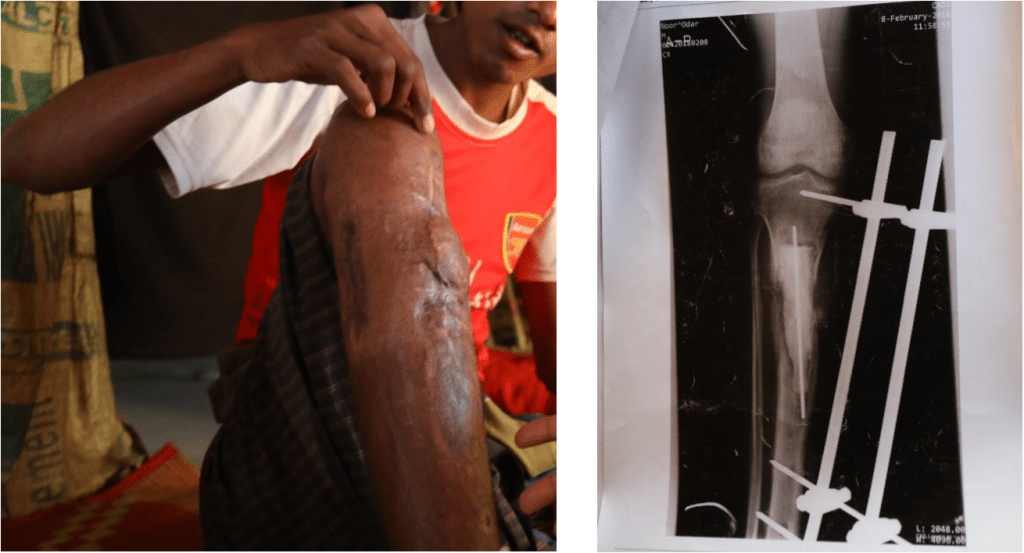
Photos: Salahuddin Ahmed for Physicians for Human Rights
Profile 14: Anowar Sadak, 28-year-old male
- Impairment: Gunshot injuries to right shoulder and chest resulting in atrophy of right arm. Treatment delayed due to violence.
- Disability: Unable to work due to loss of use of dominant hand.
Before daylight on of August 26, 2017, Anowar Sadak was at home in his village of Mirullah when he heard gunshots. He went outside and saw that other homes in his village were burning. Myanmar security forces were moving through the village, setting fire to homes and shooting. Sadak lived on the edge of his village, and he fled to a nearby village with his family. They returned home one day later, only to hear gunfire again. Sadak ran away with his three young daughters, infant son, and his wife.
As he came to a rice paddy, he saw two trucks with 10-12 security personnel inside. He slid behind an embankment with his three girls and hid, waiting for the military trucks to pass. As he looked up to see if they had passed, he was shot in the right shoulder. He lost consciousness. He was later told that his six-year-old daughter traveled to the next village and told her uncles what had happened. They came and rescued Sadak. He received basic care in a nearby village, and eventually the family decided to go to Bangladesh, where they arrived on August 30, 2018.
He was referred to the hospital. He had x-rays done that showed that the bullet had entered his shoulder and ended up in the lower right chest area. He underwent two surgeries to remove the bullet.
PHR Medical Evaluation
Sadak’s injuries were highly consistent with his story and supported by medical documentation. He has lost function of his right arm completely. He had the bullet that caused this injury and x-rays confirming the bullet in his chest.
Sadak had an 8 cm lower and a 4 cm upper linear scar with suture marks from the first failed surgery to remove the bullet from his right chest. From his second surgery, he also had a 9 cm surgical scar posterior (behind) his right chest wall that appears well-healed.
He had a 4 cm by 2 cm linear scar with cross-hatching from removed sutures at the apex of his right shoulder. He also has a 10 cm by 3 cm raised keloid (raised), red scar on the lateral side of his upper right extremity.
Sadak had continued pain and aching in his right arm, and abdominal pain. He had no motor strength in his upper right arm and complete atrophy of all muscles. The only movement he can produce from this limb is from his shoulder. As he is right-handed his injury will prevent him from being able to work.

Photo: Salahuddin Ahmed for Physicians for Human Rights
Profile 15: Bi Bi Zuhra, 40-year-old female
- Impairment: Beatings and stabbing with a knife resulting in wounds, elbow deformity, and limited right wrist function. Treatment delayed due to violence.
- Disability: Difficulty with all daily activities; limited ability to complete any basic tasks involving right hand.
On the morning of August 30, 2017, Myanmar security forces came to Bi Bi Zuhra’s village of Tula Toli. She saw helicopters. Rohingya residents fled to the river, but the security forces followed them. Men were lined up with children and security forces killed all of them, using guns and machetes. Her husband was killed in front of her, as were five out of six of her children (two boys and three girls). The men and children were put into mass graves and their bodies burned with petrol.
The security forces took Zuhra in a group of six women into a home by force. When she entered the home, she was hit on the head with a stick and knocked to the ground but remained conscious. Zuhra’s three-month-old baby was in her arms and when the girl was laid down next to Zuhra a member of the security forces sliced the infant’s throat.
The security forces tried to rape the six women in the house with Zuhra, as well as her, but the women initially fought back against this. The forces then beat the women severely, undressed them and raped them. Zuhra’s wrist was broken at this time. After she was raped, the man who raped her used a knife to cut her throat in two places. She was left to die. Many of the women around her were dead. The security forces left the women inside the house, closed the door and set the house on fire.
The fire took hold of the house quickly and Zuhra got up and grabbed a child (whom she believed to be her child) and ran out of the house. When she ran some security forces outside spotted her. They yelled at her, but seeing that she was bleeding, they let her go. She went into a house and put down the baby she was carrying and realized it wasn’t hers and that it was dead. Zuhra said she is haunted by the possibility that her baby was still alive in the house where she had been raped and that the baby had burned in the house. She went to the forest and stayed there alone for three nights. On the fourth day she went to a nearby village and spent one night in a home with a family. They gave her medicine and carried her to a small boat which transported her to Bangladesh.
PHR Medical Evaluation

Photo: Salahuddin Ahmed for Physicians for Human Rights
Zuhra’s psychiatric exam, scars, and bony deformity on her arm were highly consistent with exposure to severe trauma, beatings and rape.
Zuhra appeared very distressed and became tearful at several points during the recounting of her story. She stated that she cannot sleep and was constantly thinking of what had happened.
She had two linear scars on the right side of her chin and neck. One was 4 cm long, the other 6 cm long. They were well-healed. The scars were consistent with knife wounds. Her right distal ulna (end of fore-arm) had a bony deformity consistent with a healed fracture which gave her limited wrist function in that arm.
Profile 16: Yasin Arafath, 17-year-old male
- Impairment: Gunshot injuries to upper right thigh and right hand with limited range of motion in right thumb and atrophy at base of thumb. Treatment delayed due to violence.
- Disability: Difficulty with any basic activity involving the use of the right hand.
In the early morning hours of August 26, 2017, Yasin Arafath heard gunshots in his village of Mirullah. He came out of his home, saw people running, and fled with his family. He took his father, who is blind, to safety in the field east of his home, as security forces came from the west. As he was going back home, he saw security forces shooting and was hit in the upper right thigh. He lost consciousness. At some point, he was also shot in the right hand but was unclear about how that had happened. Arafath was taken to another village, where someone took the bullet out of his thigh. He later regained consciousness but doesn’t remember the 20 hours he was in the village before waking up.
Arafath was brought to Bangladesh by his brother and another person with a makeshift stretcher. His legs were tied together for transport. They arrived in Bangladesh one day later, and he was taken to the hospital.
PHR Medical Evaluation
The scarring on Arafath’s thigh was highly consistent with his story. The scarring on his hand was consistent with his story as well, although it seemed unlikely this was a through-and-through wound as he had suggested. It is likely this was a wound through the flesh between the first and second fingers of the right hand with an associated graze or other wound. He had atrophy at the base of his thumb and a limited range of motion of the thumb, which will cause him long-term problems as he is right-handed.
Arafath had a 2.5 cm circular scar with raised edges and hyperpigmentation (darkening) in the lateral upper right thigh. There was a medial (middle) exit wound, with a 1 cm ovoid scar, where the bullet was lodged and cut out while the patient was unconscious.
Between the first and second fingers of his right hand, there was a 1.5 cm stellate (star-shaped) scar at the base of his thumb which limited the right thumb’s range of motion. On his wrist he had a 1 cm hyperpigmented scar. He had atrophy of the muscles at the base of his thumb, and limited strength and sensation with all range of motion over the right thumb.

Photo: Salahuddin Ahmed for Physicians for Human Rights
Profile 17: Monzur Alom, 25-year-old male
- Impairment: Burns all over the body and shrapnel from explosive detonation resulting in loss of right hand function. Treatment delayed due to violence.
- Disability: Inability to work caused by extensive scarring and loss of function in wrist, making it impossible to hold objects.
Monzur Alom was a teacher at a mosque who lived with his wife and three children in the village of Tin May. One night at around 1 a.m. when everyone was sleeping, Myanmar security forces entered the village and began shooting guns. Alom and his family came out of their house and tried to flee. But Alom realized his 8-month-old son was still in the house, and turned back to get him. He saw the military shooting rocket grenade launchers at fleeing people and setting houses on fire. As Alom ran back out of his house with his son held to his chest, fire hit his son, killing him instantly. Shrapnel from the explosion hit Alom in the face and head. His face, hair, lips, ears, and beard were burned and he fell to the ground and lost consciousness.
After about an hour, the military left the village and Alom’s family carried him away. He spent one night in another village and one night in yet another village before the group left for Bangladesh, which they reached the next day. Alom reported burns to his hands and forearms, shrapnel injuries on his back, and burns on his stomach. He had lost the hair on his head and face. The rocket launcher shrapnel had hit his hands first but fire went all over and burned his whole body. He received medical treatment in Bangladesh.
PHR Evaluation
Alom’s injuries were highly consistent with a blast/burn from a frontal attack as described. The extensive scarring to his hands and wrists will make it difficult for him to work. He was unable to flex or make a fist with his right hand, making him unable to do fine motor skills such as hold objects, write, or chop.
His right arm and hand had extensive burns and scars with keloid (raised scar) and hypopigmentation (lightening) visible of the hand wrist, forearm, and upper arm. The dorsum (back) of the wrist and medial (middle) forearm had extensive scarring from burns, as did the upper arm on the right. The wrist burns were circumferential (around the wrist) and limited movement significantly. Alom had limited flexion/extension of his right wrist, with normal movement at the right elbow and shoulder, but was unable to fully flex or to make a fist with his right hand. There was atrophy of the intrinsic muscles of the right hand. He is right handed.
On his left side, he had extensive burns to his hand, forearm, and upper arm. Again burns were primarily on the dorsum (back) of the left hand with limited ability to flex and make a fist. He had atrophy of the intrinsic muscles of the left hand. The forearm, elbow, and upper arm had extensive burns, which limited flexibility of the elbow.

The top of left ear was deformed with evidence of healed burn. He has two keloid scars on his back: one is 6 cm by 2 cm overlying his right scapula (shoulder blade). The other is 2.5 by 1.5 cm overlying his left scapula. Alom also has two abdominal scars from burns, on his right abdominal flank and lower abdomen. On the right abdominal flank there is a faint triangular hyperpigmented (dark) area, 10cm by 5cm. Adjacent to that and lower on the abdomen on the right is a 9cm by 2cm hyperpigmented and faint scar. Alom also had a burn to his lower leg: a 13cm by 6cm hyperpigmented (dark) well-healed scar with one small area of keloid.
Profile 18: Salim Uddin, 18-year-old male
- Impairment: Gunshot injuries to both legs resulting in limited movement and function. Treatment delayed due to violence.
- Disability: Difficulty walking resulting in lack of ability to resume work as a farm laborer.
Salim Uddin worked as a farm day laborer and lived with his parents, five brothers, wife and son in the village of Chita Para. In late afternoon on a day in late August 2017, Uddin’s extended family was at home and saw nearby houses burning and guns being fired. They fled the house and saw military personnel in dark green uniforms shooting and burning houses.
As Uddin was running toward the mountains, he was shot in both legs. He felt pain immediately and then lost consciousness. He was carried to Bangladesh on a makeshift stretcher and received some injections on the way from a local Rohingya healer. He arrived in Bangladesh after four days of travel and was given medical care.
PHR Evaluation

Uddin’s injuries were consistent with receiving gunshot wounds in both legs. He believed the bullet entered and exited on the right and grazed his left leg. He had some type of surgery in Bangladesh but could only state that they “scraped” some of his bone on his left side. He had no records, and no clear description or understanding of the surgery.
He had a 1 cm circumferential (surrounding) scar on this right upper outside thigh that is believed to be an entry wound and a stellate (star-shaped) four by 3-4 cm scar on the upper inside thigh. The scars were healed.
He had a 14 cm scar on his left upper inner thigh, with signs of sutures. The scar was well-healed and appeared to be post-surgical. He did not know what type of surgery was performed.
He could not move his legs normally and had difficulty walking.
Profile 19: Yacub Uddin, 20-year-old male
- Impairment: Gunshot injury to left hand resulting in muscle atrophy and decreased sensation. Treatment delayed due to violence.
- Disability: Loss of left hand function resulting in inability to return to work as a laborer.
Yacub Uddin was a daily laborer who brought firewood from the mountain to sell in his village, Don Gu Lar. He lived with his mother, three siblings, and a niece. He was asleep at home when he heard shooting from another hamlet. Before the sun came up, security personnel surrounded Uddin’s own hamlet and began shooting.
Uddin had left his house to go to the mosque and pray. When he left the mosque, he saw that houses were on fire and the security forces were moving toward his house and burning homes on the way. Rakhine Buddhist civilians were also participating in the attack. Villagers came out of their homes and fled. Uddin joined them and went into the mountains, spending a day there to see if the situation would improve. The next day after the sun came up, they saw the situation in the village had only gotten worse, and they decided to flee to Bangladesh. Uddin said there were some 3,000 people in this group.
About three kilometers from Bangladesh, the group encountered the military and a mob. The military shot at them, and Uddin was shot in the left hand. He wrapped a cloth around his hand, but he was in intense pain and lost consciousness. When he regained consciousness, he was near Bangladesh and made it safely across the border, where he received medical treatment.

PHR Evaluation
Uddin’s injuries to his hand were consistent with his narrative. He had a linear scar on the left hand palm surface just below the wrist. The 5 cm scar was located at the crease between the wrist and hand. There were no scars on the back of the hand. He had decreased sensation in digits one to four on his left hand. He could grasp with that hand, but it was difficult. He had general weakness of the intrinsic muscles in that hand and decreased nerve sensation.
Uddin stated that the wound to his left hand was a graze wound, without the bullet lodging. He is right handed but will have difficulty working with his left hand.
Profile 20: Akram Hassan, 18-year-old male
- Impairment: Gunshot injury to chest resulting in difficult sitting and lifting objects. Treatment delayed due to violence.
- Disability: Loss of ability to sit and lift objects resulting in inability to return to work as a farmer.
Akram Hassan lived with his parents and worked the fields of the farm they owned in the village of Don Gu Lar. One night on or around August 25, 2017, Hassan and his family were asleep at home at 3 a.m. when they heard far-off gunshots. They woke and went to the mosque to pray. On their way home they saw that their village had started burning. Hassan went to see what was happening. He saw fire and recognized those shooting guns as military and Border Guard Police. Rakhine Buddhist civilians were also participating.
Hassan went home to get his parents, including his disabled father. While carrying his father Hassan was shot in the chest, and they fell to the ground. He lost consciousness.
Neighbors came to get him and carried him in a makeshift stretcher to a neighboring village, where he regained consciousness. A local Rohingya healer gave him injections but he remained in severe pain.

He and his neighbors traveled through several villages to the river ferry that would take them to Bangladesh, and reached Bangladesh the next day. Hassan received medical treatment at an MSF (Médecins Sans Frontières) clinic and was then taken to a hospital for an operation.
PHR Evaluation
Hassan’s injuries were consistent with his narrative. He had a 1 cm by 0.5 cm linear scar where the bullet entered below with right axilla (armpit area). This scar was well-healed.
He had an ovoid, depressed scar, 3 cm by 2 cm in his left lateral (outside) neck where the bullet exited. The scar was well healed. There was a 1 cm hyperpigmented (darkened) scar on his upper back, medially (middle), where a drain was placed and there was a small circular scar.
Hassan was disabled; specifically, sitting was difficult, lifting objects was difficult, and working was not possible.
Profile 21: Shawm Shida, 38-year-old female
- Impairment: Gunshot injury to left hand resulting in ongoing pain and inability to grip. Treatment delayed due to violence.
- Disability: Loss of left hand function resulting in an inability to return to work as a farmer.
Shawm Shida worked on her family farm and taught Arabic to children. She lived with an extended family of nine in the village of Chin Kali. At 6 a.m. on August 25, 2017, Shida first heard the sound of gunshots. When she left her house, she saw other houses on fire. Border Guard Police and military started to shoot and burn everything and people were running everywhere. Shida gathered her family and ran toward the mountain.
Before reaching the mountain, Shida was shot in the left hand. She had a great deal of pain but was able to receive an injection from a local healer. When they encountered the military, they hid in the mountains again. They spent one day there before walking north. They walked for twelve days before arriving in Bangladesh.
PHR Evaluation
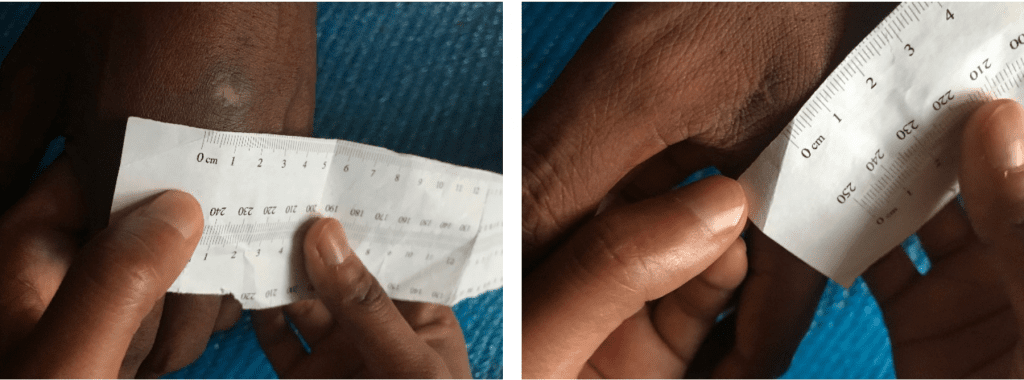
Shida’s injuries were highly consistent with her narrative of being shot in her left hand.
On her left hand, the entry and exit wounds were unclear. She had a 1.5 cm circular wound on the dorsum (back) or the hand below the second and third digit mid-hand. Between the first and second digit there was a small scar in the fold. Her sensation was decreased over distal (end) third digit over the dorsum, but otherwise strength and sensation were grossly intact. She had a weaker grip in her left than her right hand.
She continued to have pain in her left hand and had sensory changes (evidence of nerve injury), including tingling, if she held something.
Profile 22: Yasmin Ara, 3.5-year-old female
- Impairment: Shrapnel from explosive detonation injury to right (dominant) hand resulting in inability to use it. Treatment delayed due to violence.
- Disability: Loss of function in dominant hand resulting in an inability to feed herself.
Yasmin Ara’s father worked as a fisherman, and she lived with her parents and two siblings in the village of Chin Kali. Her mother recounted that on August 25, 2017, the family was sleeping when they heard gunshots and explosions. As the gunfire got closer, Ara’s mother carried her out of the house and ran toward the mountains.
While running, Ara’s mother saw explosions and houses burning, and a piece of shrapnel from a rocket launcher hit her daughter. Ara began bleeding and had injuries in three places on her arm, and also was hit by a small piece of shrapnel in her right foot.
In the mountains, they treated her with herbal remedies. The bleeding stopped and one or two days later, the injury became enlarged. After the bleeding stopped, some pus exited the wound. The family stayed in the mountains for 15 days, returning occasionally to the hamlet to get food. Ara’s mother took care of her and cleaned her wound two or three times per day. Eventually relatives helped carry Ara to Bangladesh, where she received medical attention.
PHR Evaluation
Ara’s injuries were consistent with the narrative recounted by her mother that she was injured by fire from a rocket launcher. Ara could open and close her right hand but not fully, and could not eat rice with that hand. She was right-hand dominant and was learning to eat with her left hand.
On the dorsal (top) aspect of Ara’s right forearm there were two scars that both were deep skin and muscle defects. There was a 1 cm circular and hyperpigmented (darkened) area and a 3.5 cm by 1 cm loss of brachioradialis (a muscle of the forearm). She had an incomplete ability to supinate (turn up) hand, and it was held in pronation position.
There was missing muscle flesh (brachioradialis and other muscles of forearm) 5cm by 3.5 cm into the antecubital fossa (elbow pit).
The scarring on Ara’s right arm was severe, and a large portion of muscle was missing from her forearm, which made it impossible for her to supinate this hand. She will never have full use of this hand and arm, and the disability is expected to worsen with age as the scar grows larger.
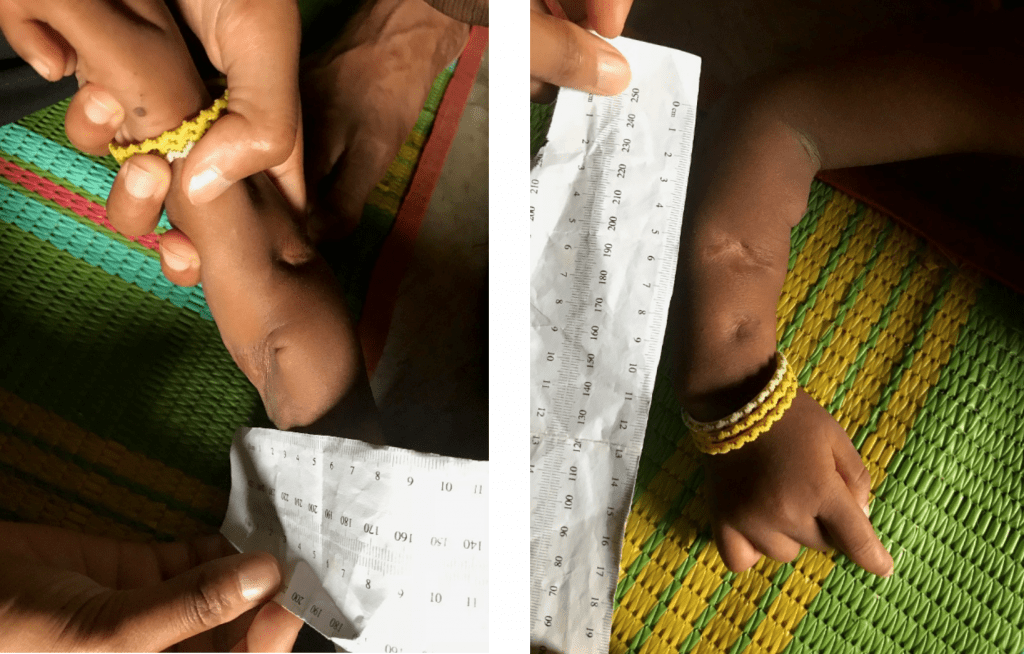
Profile 23: Abdul Salam, 33-year-old male
- Impairment: Shrapnel from explosive detonation causing left eye injury resulting in loss of sight and injury to back of neck resulting in ongoing pain. Treatment delayed due to violence.
- Disability: Unable to accomplish basic tasks, lift and carry bags of rice, and work.
Abdul Salam’s village of Tin May is located near a military camp, and personnel from the camp came to the village two days prior to the attack. They told villagers not to leave their homes at night and to inform them of any “terrorists” living in the village. They entered houses at random asking for everyone who lived there. If the male of the house was not present, they asked to see his identification papers and wrote down his name as being part of Arakan Rohingya Salvation Army.
Around August 25, 2017, at 11p.m., Salam woke up to the sounds of shooting. He ran outside with his seven-month-old daughter and fled toward the mountains. People around him were shot as they ran. An explosion hit his infant daughter, killing her. He was hit by shrapnel from the explosion and a bullet scraped the back of his neck. He could not see from his left eye after the explosion. He and other villagers hid during the night.
When the shooting stopped in the morning, the villagers saw military personnel leaving the village. They made their way home and found 30 people who had been killed by gunshots or knife wounds. They attempted to bury the dead bodies but saw military personnel returning and shooting, so they left the dead bodies and ran away.
Salam reached Bangladesh in three days. Other people had to help him walk up and down hills. In Bangladesh, he received medical care.
PHR Evaluation
Salam had physical findings highly consistent with injuries described in his testimony.
On the left side of his neck he had a raised, slightly hypopigmented (lightened) oval lesion with darker regular borders, approximately 2 cm by 0.5 cm.
On the back of his right arm he had a smooth rectangular scar with some irregularity and contracture.
Salam was told by doctors not to lift heavy things because of his neck wound, where he still had pain. This prevents him from working as he was a farmer and does not know how to do anything else. This also prevents him from helping to pick up food such as bags of rice as he cannot carry them.
He did not have records from his visit to Ukhiya hospital but states that they did X-rays and gave him treatment. They explored the wound on the neck to ensure there were no remaining foreign objects. His eye injury was also treated and he could see from the left eye but he continues to have problems with his eyesight when exposed to gas or heat.
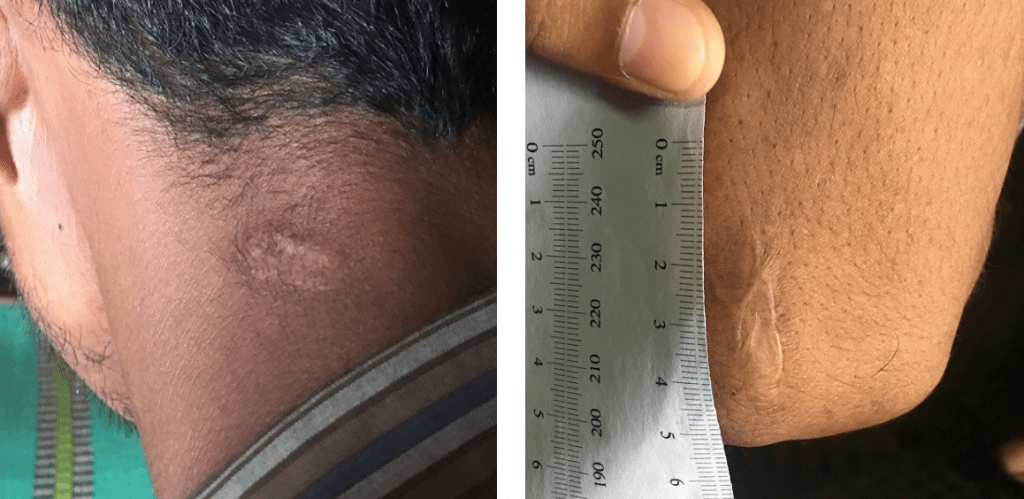
Profile 24: Mohammad Kabir, 24-year-old male
- Impairment: Gunshot injuries to both legs and right buttock resulting in ongoing pain, PTSD, and gait disturbance. Treatment delayed due to violence.
- Disability: Unable to walk long distances and work.
Mohammad Kabir was a wood carver and also farmed. He lived with his wife and three children in the village of Gu Dar Pyin. Sometime around August 25, 2017, the military entered his village and started shooting and throwing explosives. Kabir and his family fled to another village. Kabir and other young men periodically went back to their village to check on the situation. While doing so, they saw Rakhine Buddhist civilians looting the market and homes. Myanmar security forces then started shooting at the men, who attempted to flee. Kabir was shot three times in both legs and his right buttock. He remembers people carrying him to another village, but he lost consciousness during this time. After regaining consciousness, he saw his village and the market burning.
Kabir was then taken to a clinic at a nearby village, where he was given an injection and medicine for his injuries. He stayed there for 15 days in hiding and continued to receive care, until villagers told him the military was looking for people with bullet wounds and that it was not safe for him to stay there. He decided to flee to Bangladesh. People carried Kabir while his family followed on foot. The journey took six days.
PHR Evaluation
Kabir had physical and psychological findings highly consistent with injuries and abuse described in his testimony. His neurovascular exam revealed damage to vasculature and nerves on the right lower extremity consistent with injuries described. His scars were consistent with injuries described. His psychological evaluation was highly consistent with PTSD and depression. Kabir had a gait disturbance (abnormalities in walking and balance). His gait was antalgic (pain-avoiding). He had difficulty ambulating for long distances. On his right thigh he had a circular, raised hyperpigmented (darkened) scar approximately 1 cm in diameter and a circular slightly raised hypopigmented (lightened) scar with uneven borders, approximately 1 cm in diameter. He also had a circular, raised hyperpigmented scar approximately 1 cm in diameter on his left thigh and an irregularly shaped raised hypopigmented scar with hyperpigmented borders, approximately 1.5 cm by 0.5 cm on his right buttock.
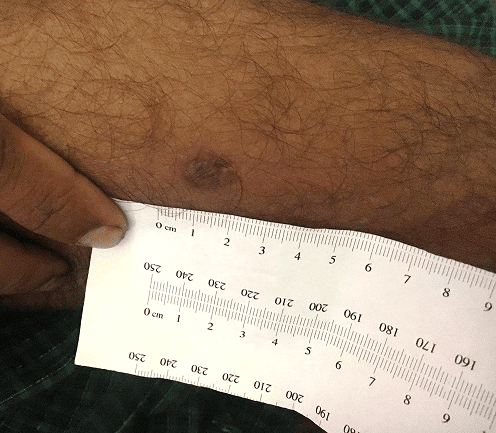


Profile 25: Abu Tayub, 25-year-old male
- Impairment: Shrapnel from explosive detonation resulting in injury to left arm and loss of function in left hand. Treatment delayed due to violence and treatment delayed in Bangladesh also.
- Disability: Unable to work due to loss of hand function.
Abu Tayub was a farmer and said he was financially well off. On August 25, 2017 at around 2 p.m., four or five military personnel entered his village of Gu Dar Pyin on motorbikes. Half an hour later, 100 military personnel, 50 Border Guard Police, and 30-40 Rakhine Buddhist civilians followed.
Tayub was at home when the security forces started shooting and throwing explosives. He ran outside, but while running he was hit on the left arm by shrapnel from a mine that exploded nearby. In the group of 17 people running with him, five died and two were injured. He managed to hide in the forest.
From the forest, Tayub could see houses burning with people inside. He saw Rakhine Buddhists slitting the throats of those who were injured but not yet dead and saw them stealing cattle and items from houses. He saw a grave with some 100 bodies in it. He stayed in the forest for three days. Then he traveled to a nearby village where he stayed for seven days, receiving some elementary medical treatment from a shop. But security forces arrived and threatened to arrest anyone who was not from that village, and Tayub decided to flee to Bangladesh. He traveled for one day to the river and then caught a boat. He was unable to walk due to the injury, and was carried throughout the journey by two people. In Bangladesh, he did not receive adequate medical care for three months. Ultimately, he had a surgery to reattach a broken bone and a skin graft.
PHR Evaluation

Tayub had injuries highly consistent with a blast injury followed by delayed treatment. Tayub was now disabled and had no function of his left hand. He was unable to farm due to the injury and would not be able to use his left hand in the future to farm.
He had a healed skin graft lesion on left forearm, loss of function of the left wrist and left hand as well as malunion of his left distal ulna (forearm bone). Existing medical records revealed that he had been treated with radial debridement (removal of tissue) and a forearm split thickness skin graft. He required this treatment after having an open wound for three months without adequate treatment.
He had no active ROM (range of motion) of his left wrist with minimal passive movement (by the examining doctor) laterally and medially. He had some active movement of his fingers but no grasp.
Tayub had a large lesion on his dorsal (top) left forearm extending from the wrist 14cm proximally towards the elbow, with a width of 5cm. There was a loss of subcutaneous tissue throughout the lesion, with the lesion indented. There was a thin epidermal layer.
Profile 26: Anowar Hussein, 14-year-old male
Impairment: Gunshot injury to right shoulder resulting in limited range of motion and inability to lift arm 90 degrees; depression and anxiety. Treatment delayed due to violence. Disability: Unable to carry out any basic tasks involving use of right arm or resume work handling cattle.
Anowar Hussein lived with his parents and worked watching cattle owned by others. Around August 25, 2017, Myanmar security officials entered his village of Gu Dar Pyin and started shooting. Hussein was playing cane ball and many villagers were watching when the security forces began attacking. Hussein ran into a nut garden and was shot in the right shoulder as he ran. From there, he saw houses burning. He saw a helicopter dropping explosives, and saw four or five Rakhine Buddhist civilians, one of whom was beating and killing people, while the others looted Rohingya houses. Hussein saw people who were injured but not yet dead having their throats slit.
The shooting continued for a few more hours. After it stopped, Hussein ran into the forest where his family was. They put turmeric on his wound and stayed in the forest for seven days before traveling to a nearby hamlet. After 15 days, they moved on to another hamlet but were told by security personnel there that those from other villages would be killed if they stayed. Hussein’s family left for Bangladesh. It took them six days to get there, and Hussein walked with the support of his younger brother.
PHR Evaluation

Hussein had physical scars highly consistent with bullet entry and exit wounds. His psychological symptoms were consistent with a diagnosis of depression and anxiety.
He had limited ROM (range of motion) of his right shoulder, with limited external and internal rotation, and limited abduction (difficulty raise arm above 90 degrees). His right upper extremity was weaker than his left upper extremity. The area around his injury was sometimes itchy and it hurt if someone pushed on it.
He had an oval, smooth hyperpigmented (darkened) scar approximately 3 cm by 2 cm on his right back shoulder and a somewhat irregular, circular hypopigmented (lightened) scar with hyperpigmented borders, approximately 1 cm in diameter.
Profile 27: Faizal Islam, 28-year-old male
- Impairment: Gunshot injury to left arm resulting in inability to grasp and hold objects in left hand. Treatment delayed due to violence. Disability: Unable to resume work as farmer due to difficulty with any basic tasks involving use of left hand.
Faizal Islam was a farmer and lived with his wife and two children in the village of Don Gu Lar. On August 25, 2017 at around 3 a.m., Islam was at home asleep when he woke up to the sound of shooting and explosions in a village near his, which borders a Border Guard Police camp. At around 4 a.m., Islam heard people from that village fleeing into his hamlet.
At around 6:30 a.m., after praying, he saw Myanmar security forces entering his hamlet. He saw homes burning and saw the security forces shooting and torching houses. All of the villagers began fleeing and many were killed. Islam believed some 200-250 people had died based on the number of bodies he saw.
Islam was shot in the left hand as he ran. He held onto the wound and kept running into the hills, where he stayed for five-six days with fellow survivors. After six days Myanmar security officials entered the forest and so the villagers were forced to flee to Bangladesh. It took them five days to get there, and Is-lam was taken to the hospital upon arrival.
PHR Evaluation
Islam had well-healed scars on his left dorsal (back) hand and left volar aspect (palm side) of his wrist that were highly consistent with a bullet entry and exit wounds as described in the narrative. Neurological exam reveals damage to both sensation and motor function as a result of the injury. His description of his psychological symptoms was highly consistent with PTSD and depression.
He had limited range of motion of his wrist. He has decreased sensation and strength in his left hand that would affect his ability to work. He is unable to grasp and hold objects with his left hand.
He has an irregularly shaped and colored partially-raised lesion, approximately 2.5 cm by 0.5 cm on his left volar wrist. He also has an irregularly shaped, hypopigmented (lightened) lesion approximately 1 cm by 0.5 cm on his left dorsal mid-hand.
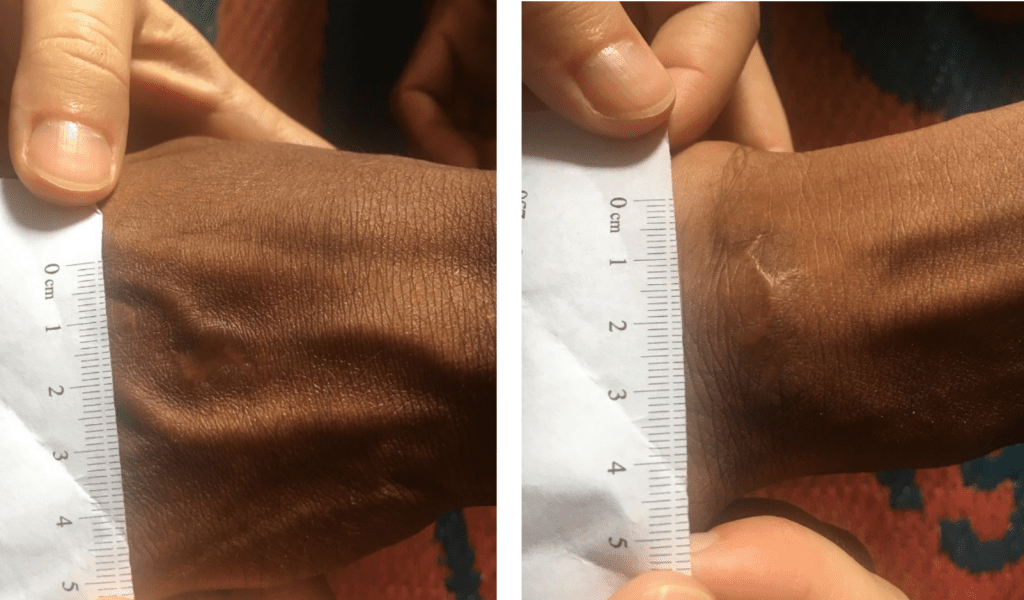
Profile 28: Abdu Shukkur, 19-year-old male
- Impairment: Gunshot injury to arm resulting in loss of majority of function of right (dominant) hand. Treatment delayed due to violence.
- Disability: Unable to resume work as day laborer due to loss of function in right hand.
Abdu Shukkur was a daily laborer who did farming and fishing in his village of Kyaunk Pan Du. He was sometimes called to work without pay at a nearby police camp. If someone could not go when asked, the police took money from them and sometimes beat them.
Around August 25, 2017 at 8 a.m., Shukkur was in his house when Myanmar security forces surrounded his village and started shooting. He ran out of the house toward the forest and was hit in the arm. He saw the bullet, which was golden, hit the ground. He continued running into the forest, and once there, he tied his arm in a sling. From the forest he saw that his home was burning. His family stayed in the forest for six-seven days, and then they fled to Bangladesh. The journey took them 24 hours.
PHR Evaluation
Shukkur had physical wounds consistent with an injury from a large bullet. Due to the extent of the internal damage, he had lost most of the function of his right (and dominant) hand. He could not grasp or hold things with his right hand and could not eat with his right hand. He continued to have pain. His psychological symptoms were highly consistent with ongoing depression and anxiety.
Shukkur’s right wrist had a decrease in flexion and some in side-to-side movement. He had decreased sensation to touch below the injury and decreased strength in his right upper extremity. He also had decreased external and internal rotation of right shoulder.
His right elbow had limited flexion and he was unable to fully extend his elbow. He has some active movement of his fingers, but with weak grasp.
He had an oval, indented, atrophied scar approximately 4.5 cm by 1.5 cm on his right upper extremity.
Profile 29: Sayed Amin, 35-year-old male
- Impairment: Gunshot injury to right lower shin resulting in difficulty walking and decreased sensation. Treatment delayed due to violence.
- Disability: Unable to resume work as a farmer, shop owner, and teacher due to difficulty with walking.
Sayed Amin attended a religious school, worked as a religious teacher, and also had a small shop and farm where he worked with his brothers in the village of Kyaunk Pan Du. One morning at approximately 11 a.m., on or around August 25, 2017, villagers were farming in the paddy field when they saw the military coming from a security camp nearby. The farmers informed the other villagers that the military was coming and they needed to hide.
Amin was in the shop when the farmers arrived. He closed his shop and went home, but his family had already left. He entered his house to take clothes and things for his children. Within minutes, the military was moving through the village. When they reached the center of the village, they started shooting. Amin started running along with many others.
Nine villagers from the group Amin was running in were shot and died. Amin was hit by a bullet as he ran, and he felt a bone break as he fell. He was hit when he was already out of the village, so the military didn’t see him. He was able to call his brothers with his mobile phone, and when the military left, his brothers came and carried him to the forest, where the rest of his relatives were. They stayed there for nearly 10 days until the security forces returned to an area near the forest. The villagers then decided to flee to Bangladesh, arriving there two days later.
While still in Myanmar, Amin had used betadine and septadine from a village medicine shop to clean his wound and also got some medicine to reduce pain. He also used some leaves on the wound. In Bangladesh, he was sent to the hospital and was there for over one month for a surgery on his leg.
PHR Evaluation

Amin had physical scars highly consistent with bullet entry and exit wounds. He was disabled by his injury, could only walk with a limp, and had decreased sensation on his right lower leg. His medical record indicated that he underwent a right ORIF (open reduction and internal fixation). He had two x-rays from October 2017 and April 2018 which revealed the metal rods placed to fixate a broken femur.

On his left lateral thigh, he had an oval, slightly scaly scar with hyperpigmented (darkened) borders, approximately 1 cm by 0.5 cm. He also had a circular, hyperpigmented scar on his left medial (middle) thigh, approximately 0.5 cm in diameter.

On his right lateral thigh, he had a hypopigmented (lightened) scar extending distally (downward) to the knee. He also had on his interior right thigh a circular scar, with slight indentation, hypopigmented with hyperpigmented borders, that was approximately 2 cm by 1.5 cm.
He also had an irregularly shaped scar, hypopigmented with hyperpigmented borders, approximately 5 cm by 2 cm on his right lateral posterior thigh.
Profile 30: Azizul Hauqe, 17-year-old male
- Impairment: Gunshot injury to back resulting in pain after speaking and eating and difficulty with basic tasks. Treatment delayed due to violence.
- Disability: Unable to resume work as fisherman and farmer due to pain from injury.
Before the attacks, Azizul Hauqe’s main activities were fishing and farming. He was at home sleeping with ten other family members in his village of Allay Than Kyaw around 11 p.m., when his mother began shouting that the military was coming. Hauqe heard gunshots and ran out of the house. He recognized the military’s uniforms. As he ran he was hit by a gunshot in the back, and the bullet came out on the right side of his body. He lost consciousness and woke up in the bushes sometime later. His brother then took him near a river.
Resource: Shot While Fleeing: Rohingya Disabled by Myanmar Authorities’ Targeted Violence






When the military left the area, his brother carried him to Bangladesh. Hauqe was awake but was not speaking. Upon arrival in Bangladesh, Hauqe was taken directly to the hospital and spent one month there. He received IV drips and wound packing, but no surgical treatment.
PHR Evaluation
Hauqe’s two lesions suggested a through-and-through gunshot wound, consistent with his narrative. The distinct borders of the wound on his lower right back were typical of an entry wound. The exit wound was cleaner than in similar cases, but that can depend on bullet type and proximity.

Mohammad Esouf was praying at the mosque when Myanmar security forces attacked his village. He was shot in the arm and abdomen as he fled; upon arriving in Bangladesh, he received surgery for both and was hospitalized for four months. He has difficulty using his right arm. 
Mohammad Esouf was praying at the mosque when Myanmar security forces attacked his village. He was shot in the arm and abdomen as he fled; upon arriving in Bangladesh, he received surgery for both and was hospitalized for four months. He has difficulty using his right arm. 
Mohammad Esouf was praying at the mosque when Myanmar security forces attacked his village. He was shot in the arm and abdomen as he fled; upon arriving in Bangladesh, he received surgery for both and was hospitalized for four months. He has difficulty using his right arm.
Hauqe could not walk for long distances. He had pain where the gunshot wound was, especially when he talked for a long time or had a full stomach. He ate only small meals and ate slowly.
On his right lower back, Hauqe had a well-healed 1.5 cm by 0.5 cm wound, oval in shape, with distinct hyperpigmented (darkened) borders and a raised linear scar, paler than the wound, within the center of the lesion.
On his right chest wall, in the lower thoracic region, intercostal region around the seventh or eighth rib, lateral to midline, there was a well-healed 1.5 cm by 1 cm irregular-shaped lesion of unclear superior borders.
There was no paresthesia (tingling sensation) in the area of both wounds. Hauqe did report pain with palpation (touching the area) along the area of both wounds. He reported pain in the area of the wound while extending his right arm more than 120 degrees.
Profile 31: Hafsa Baegum, 30-year-old female
- Impairment: Beating to lower back while six months pregnant resulting in miscarriage with prolonged uterine bleeding; two inch deep knife wound in neck; limited use of right arm and hand due to injury from beating. Treatment delayed due to violence.
- Disability: Unable to carry out domestic activities or perform basic tasks due to difficulty with all basic tasks involving use of right hand and arm.
The military entered Hafsa Baegum’s village, Allay Than Kyauw, at around 9 a.m. on a Saturday. She was washing clothes near a well and could see them coming. She watched from a distance as the military looted the shop where she worked. She went home, but the military soon arrived there, detaining her and her four children. A soldier grabbed her hand and twisted her arm, injuring it. He then kicked her in the back and she fell to the ground. Baegum said she saw the security forces take an old man into the street and kill him by stabbing him multiple times in the stomach and then shooting him.
The women were gathered together in a place near the school. The security forces then chose some women and took them, including Baegum, to a narrow street. They took her shawl and threw it away, and put a knife to her neck. She called on Allah to save her, despite soldiers’ demands that she stop. A soldier kicked her forcefully in the lower back. Eventually one soldier came and took her back to where the rest of the women were. While Baegum was being taken to the narrow street, she saw the military kicking, holding, punching, and beating women with guns. At around 3 p.m., the military burned down houses. Baegum found her family and fled toward Bangladesh, where they arrived three days later. She was six months pregnant during the attack and when she left for Bangladesh, and was bleeding all through the journey there. She had a miscarriage at a hospital in Bangladesh, and bled for about 40 days after.
PHR Evaluation
The injury to Baegum’s right arm was highly consistent with an acute traumatic injury of ulnar (forearm bone) side of wrist in the region of the flexor capri ulnaris (forearm muscle) and its tendon. She did not receive any care for the injury. She now had only limited use of her right arm. Her husband has had to take over various domestic duties, such as cooking and cleaning.
The knife wound/injury was about two inches deep. It took about 15 days to close. The doctor gave her cream and no surgery.
On her right chest, above the right breast, there was a well-healed, skin-colored, hypertrophic (raised) lesion, 1 cm by 1 cm.
On the right forearm/right arm, when in a supinated (turned) position, there was a visible soft tissue mass along the ulnar side of the wrist, no ecchymosis (discoloration) visible, no laceration, and mild pain on palpation (touching).
On her right hand, the thenar and hypothenar eminence (thumb area) appeared atrophied as compared to her left hand (she was right-handed prior to this injury). As she attempted to pronate (turn palm down) her right hand, the subluxation of the presumed flexor carpi ulnaris tendon was palpable and visible. Upon pronation of her hand, her right-hand deviates radially. She had obvious weakness as she attempted to pronate her hand: there was suspected injury to the flexor carpi ulnaris.
Baegum’s right hand had decreased strength and her right wrist has decreased flex and extension. Sensation was grossly intact.
Profile 32: Ramzan Ali, 50-year-old male
- Impairment: Gunshot injury to left arm resulting in permanent contraction of fingers on left hand. Treatment delayed due to violence.
- Disability: Unable to return to work as farmer and fisherman due to difficulty with all basic tasks involving use of right hand and arm.
Ramzan Ali was a farmer and fisherman and lived with his wife and seven children in the village of Kyaunk Pan Du. Early in the morning on August 27, 2017, they were awoken by the sound of gunshots. He and his family ran away from their hamlet alongside other villagers. While running, Ali saw an estimated 60 military personnel. He was shot from behind in the left arm and fell to the ground. He lost consciousness, but his children carried him to the surrounding hills. When he recovered consciousness, he heard from others that 10 other villagers had been killed in the attack.
They stayed in the hills for three days, until the military entered the area and started shooting and firing rocket launchers. Ali’s family started running and decided to head toward Bangladesh. They walked seven to nine days until they crossed the border, at which point Ali was admitted to the hospital for two months, receiving treatments and skin graft surgery to his left arm.
PHR Evaluation
Ali’s injuries to his left arm and hand were consistent with his narrative of being shot. On his left hand, his fingers remained contracted, and are assessed to remain like this permanently, with loss of function of the hand. On his left ventral (front) forearm, there was a well-healed wound, approximately 9-10 cm in length and 2.5 cm in width, with well-demarcated thickened, cord-like raised borders. The skin within the border was without obvious hair growth but hair follicles were present. The more proximal (closer) portion of the wound had a linear appearance of about 1.5 cm. On his left dorsal (underside) forearm he had a semi-stellate (star-shaped), well-healed, pale lesion that is 2 cm by 1.5 cm large.
Profile 33: Rashid Ahmed, 30-year-old male
- Impairment: Shrapnel from explosive detonation resulting in left leg injury.
- Disability: Unable to continue work as a farmer or handle cattle due to leg injury.
Rashid Ahmed worked as a farmer and owned a number of cattle. One day around noon Ahmed, who was at home in his village of Gu Dar Pyin because of government-imposed movement restrictions, heard gunshots. He and others left their houses to see what was happening. Some were shot immediately, while Ahmed and others attempted to flee Myanmar security forces, who they could see some distance away. As they ran across a field, some people stepped on landmines. Ahmed saw three people near him step on mines and die immediately.
At the border of the hamlet, there was a small river which fleeing villagers, including him and his family, were able to cross by boat. When Ahmed re-crossed the river to give the boat to others, he was shot or hit by shrapnel in his left thigh and fell down near the edge of the river. He found a banana tree trunk and was able to use it to get back across the river. He hid in some bushes on the other side of the river and lost consciousness. When he woke up several hours later, he saw that everything in the village had been burned.
Ahmed stayed on the other side of the river for about one month and received some treatment for his injury. He was then reunited with his family and they decided to leave for Bangladesh, joining a large group of people who were traveling there. They faced continued harassment by the Myanmar security forces along the way. They reached Bangladesh eight days later.
PHR Evaluation
Ahmed’s injuries to his left thigh were consistent with his narrative of being hit by a gunshot or shrapnel. He still faced daily pain in the area, especially when carrying something. He could not work like he did before.
On his lateral (outside) left thigh, he had a 0.5 cm by 0.5 cm circular, skin-colored lesion with distinct borders.
On his left medial (middle) thigh he had a 1.5 cm by 0.5 cm lesion, hyperpigmented (darkened) around its borders, shiny-appearing, contracted and depressed.
Profile 34: Rabia Basri, 21-year-old woman
- Impairment: Gunshot injury to left leg and right arm resulting in limited range of motion (inability to flex right knee) and atrophy.
- Disability: Unable to walk or bear weight on her left leg without crutches and unable to use her left leg when transferring from chair to floor.
Rabia Basri was at home with 14 relatives in the village of Chut Pyin when they heard gunfire and tried to run to the surrounding rice fields. Five of them were shot dead while trying to escape. Basri fell when she was struck in the left leg and right arm. She reported being in and out of consciousness while she lay bleeding. She recalled pretending to be dead when six or seven Myanmar security forces and Rakhine Buddhist villagers approached her. They stole her valuables and left her in the field, where she stayed well into the night until neighbors carried her to a nearby village. Two days later, Basri left for Bangladesh, where she underwent surgery on her leg with orthopedic external fixation.
PHR Medical Evaluation
The physical findings were highly consistent with Basri’s report of being shot while running.
Over her arm, a small round lesion on the antecubital fossa (interior crease of the elbow) connected to a 6 cm linear defect with suture scars on either side was highly consistent with a gunshot injury from a low velocity bullet that did not pass completely through the arm, and which resulted in extraction of a bullet and suturing (surgical closing of the wound) afterwards.
The lower leg displayed a group of scars consistent with a single bullet entry wound, causing fracture to the tibia and fibula, and subsequent surgical repair. A single 1 cm by 2 cm oval scar was apparent on the anterior/medial aspect of the tibia (large bone of the lower leg), approximately 8 cm below the patella (kneecap), with some blurring of the margin inferiorly, likely representing the entry wound of the projectile. Irregularity of the bone structure of both the tibia and fibula (large and small bones of the lower leg, respectively) is appreciable on palpitation of the scar. The lower left leg had a longitudinal surgical lesion with punctate suture scars on either side. The gastrocnemius and soleus muscles (calf muscles) of the left leg appeared grossly atrophied when compared with those of the right leg.
Basri could hold her knee at 120° but could not flex her knee more than 30° in any direction. The resultant atrophy and inability to walk likely reflects significant injury to the bones and the neurovasculature of the leg – most likely due to initial injury and subsequent underuse of her calf muscle. The limited range of motion of the knee joint was most likely an indirect consequence of the initial injury, due to lack of access to post-operative physical therapy. Basri now was unable to walk or bear weight without crutches; when transferring from a chair to the floor, she could not use her left leg at all.
Profile 35: Mohammed Isaq, 17-year-old boy
- Impairment: Explosive blast injury to right leg resulting in neuromuscular injury that has been unable to heal despite surgery.
- Disability: Unable to walk or bear weight without crutches and ongoing pain in right leg.
As Mohammed Isaq walked home from afternoon prayers, he saw his village of Chut Pyin being surrounded by Myanmar security forces and Buddhist Rakhine villagers. He then heard gunshots and security forces ordering people to come out of their homes. He sought shelter in a house, where he was then struck by a projectile shot from outside. The house was then set on fire and Isaq came out dragging his leg. He then hid by a pond until 4 a.m., when his father rescued him and took him to a neighboring village. Isaq also said the Myanmar military shot people, and Rakhine Buddhist villagers then stepped on and slit the throats of the injured. He also reported that the attackers set dead bodies on fire.
After remaining in a neighboring village for a week, Isaq began a 12-day journey to Bangladesh, where he was hospitalized for five months and underwent multiple surgeries with rods and screws in his leg. Six months later, he still could not bear weight on the injured leg and required crutches to walk.
PHR Medical Evaluation
The lesions present on Isaq’s right leg were highly consistent with an explosive blast injury, with multiple shrapnel scars and a long linear surgical scar to extract fragments and surgically repair his femur (large bone of the upper leg) with internal fixation.
The right anterior thigh displayed numerous linear scars on the lateral aspect of the mid-thigh, measuring 2 cm to 5 cm in length and slightly raised, indicating multiple blast fragment scars typical of a grenade injury. A single irregular 1.5 cm by 1 cm scar was present on the medial aspect of the thigh just superior to the patella (above the kneecap), with an irregular border, consistent with an exit wound from a fragment.
This leg also had a vertical linear surgical scar that started on the anterior thigh near the level of the iliac crest (highest part of the sacrum, also known as the “hipbone”) and extended down the anterior thigh ending inferolateral to (below and to the side of) the patella. This scar was approximately 40 cm in length, varying in width from 0.5 cm and relatively clean approximation (wound closure) to a hypertrophied (enlarged), poorly approximated, and 4 cm wider region near the patella. The surgical defect was consistent with internal fixation of the femur bone and the removal of shrapnel in certain places. A second line of sutures was present along part of the original surgical scar, indicating that this likely did not heal and required a second effort to close. Isaq’s continued pain, inability to bear weight, and reliance on crutches suggested that he suffered from significant bony and neurovascular injury that has not healed well, despite surgery.
Profile 36: Nur Asha, 20-year old woman
Impairment: Gunshot injury in left wrist with nerve injury, resulting in decreased sensation and feeling in her first, second, and third fingers. Disability: Limited function of and ongoing pain in fingers and wrist.
Nur Asha said that on the day of the Chut Pyin attack, four Myanmar security forces surrounded her house and ordered her to come out. When she came out with her four-month-old daughter and two-year-old son, they burned Asha’s house down
Asha managed to flee by running, but she and her son were shot when they reached the rice field. The bullet killed the child and then entered Asha’s left wrist. After she was shot, she said military came and kicked her three times to check whether she was dead. Asha lay in the rice field and estimated that she was surrounded by roughly 100 other women doing the same. She said her sister-in-law, lying nearby, refused to surrender her baby boy when the military tried to wrest him from her; they shot the mother dead, and, when the baby fell from her hands, they shot the baby as well. “The bullet entered the head and it didn’t exit.” Asha said scores of people were killed in the rice fields around her. “People died like small fish in a dried pond…. I myself alone, had to cross 25 dead bodies.” She made it to the next village and then walked approximately 11 days to reach Bangladesh, where she underwent surgery on her wrist.
PHR Medical Evaluation
Asha’s clinical exam was highly consistent with her report of a surgically treated low-velocity gunshot wound, such as one that would have been caused by a bullet traveling through her son before striking her.
An examination of her left hand showed a hyperpigmented and raised lesion extending from the radial side of the forearm to the dorsum of the wrist. The wound was approximately 8 cm long and 2.5 cm wide. It had jagged borders and areas of skin contraction, indicating that the scarring pattern was irregular, consistent with the injury being caused by a lower-speed projectile.
Asha had a grossly decreased sensation of her first, second, and third digits (thumb, index, and middle fingers) from the palm to the proximal interphalangeal (middle finger) joints, which was typical of a radial nerve injury. She rested her hands with over-flexion of the fingers and had limited range of motion and pain with active movement (moving her wrist and fingers herself vs the medical examiner) of the fingers and wrist.
Profile 37: Somaiya Akter, 9-year-old girl
- Impairment: Gunshot wound to the upper right leg with complications of an infection of the skin and soft tissue with suspected bone involvement.
- Disability: Requires a cane to walk and has significant pain when bearing weight on her leg with limited function of her right leg.
Somaiya Akter was at home with her mother (Profile 19), brother, and father when they heard gunshots and saw smoke coming from many nearby homes. They ran out of their house when it, too, was set on fire, and Akter’s father and brother were shot dead just 20 to 30 yards from their home. Akter was shot in the leg and could not continue running, so she stayed by the bodies of her father and brother. Myanmar security forces took Akter’s mother to one of the places where the military were gathering women. They hit her on her head and back with sticks, but she managed to escape and return to where her husband, daughter (Akter), and son were shot. Both Akter and her mother then fled into the fields and later spent 10 days traveling to Bangladesh, where Akter had surgery on her leg, which had become infected. Six months later, he wound had not healed properly and akter still had to walk with a stick. She reported no fevers.
PHR Medical Evaluation
The scars on Akter’s leg were highly consistent with her and her mother’s testimony. Akter’s right thigh had scars from bullet entry and exit lesions, and from surgical treatment. The mid-thigh reveals two bullet wounds: a 2 cm by 2 cm circular, well-healed entry wound on the posterolateral aspect (back) of the mid-thigh and an irregular 2 cm by 4 cm oval hypertrophied (enlarged) exit wound on the anteromedial aspect (front) of her thigh. Akter also had circular puckered wounds near the patella (kneecap) and at the superior aspect of the thigh, typical of surgical scars from an external fixator used to immobilize a leg after surgery. Akter required a cane/stick to walk and had significant pain when bearing weight on her leg. This suggested that she has gait disturbances which included abnormal walking and not being able to balance. Six months after the incident on the examination today, the exit wound which was open and has broken skin and had a slow drainage of purulent fluid and a red, inflamed appearance. This was evidence of an active infection which involved the skin and soft tissue with suspected bone involvement. An infection of the bone can further reduced her leg function, worsen leg pain, and contributed to permanent disability.
Profile 38: Sayed Alom, 21-year-old man
- Impairment: Gunshot wound to lower left leg with the need for surgery.
- Disability: Requires a cane to walk and has persistent pain.
Sayed Alom ran out of his home when he heard shooting and yelling and ducked into a neighbor’s home as gunfire began and he saw how many Myanmar security forces were in Chut Pyin. He was shot in the left lower leg and managed to hide in the nearby rice fields, where he reported being surrounded by 10 to 20 people, some shot and others with slit throats, as well as a dead woman with a mutilated breast. He also said that his congenitally disabled uncle had been stabbed and killed by gunshot. Alom lay in the field until his brother found him the next day and brought him to a nearby village. Alom was then carried to Bangladesh, which took 10 to 12 days. Once he reached Cox’s Bazar, Alom spent five months in the hospital for leg surgery.
PHR Medical Evaluation
The physical examination of Alom’s left leg revealed a single scar on the anterior tibia and surgical scars on the lower leg that were highly consistent with his report of a gunshot injury that was surgically repaired. A single oval scar measuring 1 cm by 1.5 cm, typical of a bullet entry wound, was present on the anterior surface of the left lower leg, approximately 5 cm below the patella (kneecap). The left leg also shows evidence of surgical repair of the tibia (large bone of the lower leg), with a linear wound running the entire length of the lower leg from the patella to the ankle. There also were scars consistent with placement and subsequent removal of fixator screws along the anterior and lateral axes of the lower leg. Alom reported that he required a cane/stick to walk and had moderate, persistent pain.
Profile 39: Sultan Ahmed, 19-year-old man
- Impairment: Gunshot wound to left ankle, resulting in significant injury to neurovasculature and bone of the lower left leg and subsequent amputation of lower left leg.
- Disability: Requires crutches to walk on his remaining leg.
On his way home from prayers on the day of the attack, Sultan Ahmed saw Myanmar security forces gathered inside and outside the village. Once home, he heard orders for everyone to leave their houses. As he tried to flee, Ahmed was shot in the left ankle and right shoulder. He also said he was grazed on the head by two bullets. Ahmed was able to hide in a shallow pond near his house for many hours until neighbors rescued him. During this time, he saw dozens of women and girls being taken inside the school, where many were raped and killed. He heard them crying “Oh, father, oh, mother, come and save us!” and saw a woman with mutilated breasts. Ahmed also reported overhearing orders that all Rohingya men and boys be killed; those who did not die from bullet wounds had their throats slit. While hiding, he said he saw children being thrown into a fire, as well as dozens of dead bodies. After 10 hours of hiding, neighbors carried Ahmed to a nearby village, where he stayed for seven days before traveling to Bangladesh. Once in Bangladesh, he was hospitalized for 14 days. Doctors amputated his left lower leg and surgically removed the bullet that was lodged in his left shoulder. Ahmed added that neighbors told him that his father was taken and killed, but he does not know any further details.
PHR Medical Evaluation
Ahmed’s injuries were highly consistent with his testimony of having sustained a head wound, multiple gunshot injuries, and the amputation of his left leg. He had a 7 cm by 4 cm oval scar on his right deltoid (shoulder) area, oriented in an anterior/posterior direction with hypertrophied (enlarged) and irregular margins and hyperpigmentation. The scar had suture sites on the lateral aspects, consistent with surgical removal of the projectile at the site of entry, with no bullet exit wound. The wound appeared poorly healed, likely secondary to delayed treatment. Ahmed also has a 0.5 cm by 1 cm linear scalp scar with broad margins to the left side of the head consistent with his report of being struck on the head. The cause of the head injury cannot be determined, as the testimony with regard to it was unclear. The amputation of his left leg below the knee was consistent with Ahmed’s report of being shot in the lower leg, and then being unable to walk because of significant injury to the neurovasculature or bones of the leg. The surgical scar was closed and well approximated (cleanly healed); the entire area was free. He required crutches to walk on his remaining leg.
Profile 40: Jahan Ara, 17-year-old girl
- Impairment: Gunshot wound to left shoulder, resulting in fracture and deformity of clavicle. Delay in treatment and surgery.
- Disability: Limited function of her left arm and shoulder with persistent pain.
Jahan Ara was in her house with five other relatives when they heard gunfire. Her uncle was struck in the head by a bullet while inside the house; the rest of the family escaped toward the fields. As they were running, Ara’s cousin was shot and fell to the ground. Ara was struck by a bullet in her left shoulder and fell. Ara reports that she was in and out of consciousness while she lay in the field, but remembers that a group of three Rakhine Buddhist civilians and one soldier walked by her. They kicked her and she pretended to be dead, so they took her jewelry and left. Ara said that more than a dozen dead bodies surrounded her in the fields. After the massacre, her grandmother and others carried her to a nearby village, where they stayed for roughly six days. They then went to Bangladesh, where Ara was hospitalized for more than a month.
PHR Medical Evaluation
Ara’s physical examination was highly consistent with her report of gunshot injury with entry to the left deltoid (shoulder muscle) and damage to the soft tissues of the shoulder and the clavicle (collarbone) – and, possibly, the scapula (shoulder blade) – before exit. On her anterolateral (front-side) deltoid area, Ara had a 2 cm by 3 cm scar with a teardrop shape and a poorly differentiated margin. There was an appreciable deformity in the mid-clavicle, but the scapula appeared intact by palpation. Ara had a second scar on her left scapular area, triangular in shape and approximately 3 cm by 4 cm, with poorly differentiated margins and hypertrophy (enlargement) near the inferior aspect (bottom) of the wound. Based on the physical evaluation, the bullet likely entered her shoulder on the side, hit and broke her clavicle, bending the curve of the bullet, which then angled out of her upper back near the scapula. Ara had a limited range of motion in her shoulder. She was able to elevate her arm 45° above horizontal in the anterior plane (forward) and only 30° above horizontal in the lateral plane (side). Her report of improvement after surgery, subsequent deterioration in mobility and range of motion, and persistent pain reflected a lack of access to post-operative care and physical therapy.
Profile 41: Anayath Korim, 20-year-old man
- Impairment: Blast injury resulting in significant burns to legs and permanent scarring.
- Disability: Difficulty moving joints, difficulty walking and has a limp, and has ongoing pain.
Anayath Korim was in his home just outside the village of Chut Pyin when he heard gunshots coming from the village, and several children ran into his house for shelter. As nine people hid inside Korim’s home, a large explosion occurred and he lost consciousness. He awoke a short time later as neighbors were carrying him to a neighboring village.
PHR Medical Evaluation
The physical findings were highly consistent with Korim’s testimony of sustaining a significant blast injury which resulted in burns to his leg. The entire lateral aspect (side) of the right leg, from the groin to the ankle, was covered with extensive burn scars. These areas appeared mottled with areas of hyper- and hypopigmentation (mixed discolora-tion), irregular texture, lack of hair, and contractures typical of a full-thickness burn injury. There were some areas that appeared to have undergone surgical grafting of skin from other non-affected areas to replace some of the missing skin. This type of extensive, full thickness burn suggested a significant blast injury that resulted in Korim becoming unconscious and unable to remove himself from the burning home quickly enough. He suffered from permanent scarring, pain, and difficulty moving his joints, and he walked with a limp.
Profile 42: Mohammed Yusuf, 5-year-old boy
- Impairment: Explosion resulting in injury to face, right eye, and right ear.
- Disability: Complete blindness in the right eye and hearing loss in the right ear.
Mohammed Yusuf and his family live in a village that is roughly a 10-min walk from Chut Pyin. He and his older brother were playing near Chut Pyin when he heard gunfire and explosions close to him, followed by a sudden pain in his right eye. His brother carried him home to their mother, who saw that Yusuf’s eye was covered with blood. She cleaned him up, but Yusuf said his head still hurt. Over the next four days, Yusuf did not get up and ate very little. Since then, he has not been able to see out of his right eye and cannot hear out of his right ear. Concerned that their village would be attacked, Yusuf’s family decided to walk to Bangladesh, which took seven days. Once they arrived, Yusuf’s mother took him to a hospital in Cox’s Bazar.
PHR Medical Evaluation
The physical examination findings of blindness in Yusuf’s right eye and hearing loss in his right ear were consistent with his testimony of exposure to explosions and blast trauma. Yusuf’s right eye exhibits a loss of the border between the iris and pupil, which were both grey in color and difficult to distinguish. He was completely blind in the right eye and could not see light/dark or any colors. The pupil was not reactive to light. There was a single linear deformity that was oriented vertical-ly from the 1 o’clock location of the iris through the pupil to the 5 o’clock position of the iris. Eye move-ment was intact. No injury was apparent to the soft tissues around the eye. These findings were highly consistent with an ocular injury with damage to the pupil. This was consistent with the effects on the eye of small foreign bodies that can be blown into the air during blasts from grenades and other explo-sive military weapons. The right ear did not exhibit any external signs of trauma. No otoscope was available for this evaluation, so visualization of the inner ear and tympanic membrane was not possible. Two medical exams were administered to test for hearing loss. The Weber hearing tuning fork sound is heard equally loudly in both ears when hearing is normal; however, Yusuf’s test lateralized to the right ear, while the Rinne hearing test found that Yusuf heard the tuning fork better over air in the left ear (normal) and better in the bone in the right ear (abnormal). In sum, these findings detected a conductive hearing loss in the right ear, likely secondary to blast wave trauma to the middle ear or cochlea. Post-traumatic conductive hearing loss is highly consistent with Yusuf’s testimony of blast trauma.
Profile 43: Abdul Roshid, 22-year-old man
- Impairment: Beating of the back and gunshot wound to left upper leg, resulting in nerve, muscle, and ligament injuries.
- Disability: Atrophy of calf and thigh muscles, weakness of the left leg, walks with a limp, on-going back pain, and depression.
Abdul Roshid was shot as he ran through gunfire during the attack on Chut Pyin. He then hid by a pond, from where he witnessed people being killed and women being raped. Three men then found him; while a soldier with a gun held him down, Roshid was stepped on and kicked in the left side of the chest, tor-so, and leg. The men eventually left Roshid in the field, and he was found in the evening by neighbors who took him to a nearby village. There was no available doctor to see him, so Roshid used local reme-dies such as garlic and turmeric to treat his wounds. He remained in the village for six days and the gunshot entry wound became red and swollen with in-fection, draining pus and developing a foul odor. Over three days, Roshid’s brother and father carried him to the Bangladesh border, where his wound was washed and he was given medication at a hospital.
PHR Medical Evaluation
Overall, the physical findings were highly consistent with Roshid’s report of being shot in the left leg while fleeing and of then being beaten. His left leg examination was a textbook example of a gunshot wound with nerve destruction. A 1.5 cm circular depressed and hyperpigmented (darker) wound on the medial upper left thigh is typical of a bullet entry wound with enlargement secondary to a skin infection. A 1 cm by 0.5 cm wound with a skin protuberance on the left posterior upper thigh below the buttock represented the bullet exit wound. The bullet likely traveled through Roshid’s medial thigh to the posterior area, damaging the peroneal nerve and disrupting muscles and ligaments along the way. There was also atrophy of the calf and thigh muscles, and Roshid has a limp. Upon neurological exami-nation, he displayed weakness of the left leg (4/5 strength in the upper leg and 0/5 strength in the an-kle/foot), with a left foot drop and sensory deficits (lack of sensation) of anterior and medial aspects of the lower left leg (on the inside of the calf) typical of a peroneal nerve injury. The finding of muscle ten-derness over the back was also highly consistent with his testimony of being kicked and stepped on while lying, curled up, in a defensive position. He reported left hip and back pain with tenderness to palpation on the left paraspinal muscle along the fourth and fifth lumbar region, as well as muscle ten-derness over the iliac crest (hip), probably secondary to being beaten. Although PHR did not conduct a full psychological assessment, Roshid had a poor affect and shows symptoms of depression and post-traumatic stress disorder (PTSD) that are highly consistent with his experience. He reports that he is married with two sons, but that he now cannot provide for his family.
Acknowledgments
This report was co-written by Laura Mills, research consultant for Physicians for Human Rights (PHR), as the principle author, and Rupa Patel, MD, MPH, DTM&H, assistant professor in the Division of Infectious Diseases and director of the HIV Pre-Exposure Prophylaxis (PrEP) Program at Washington University in St. Louis.
Initial research design and data collection was conducted by the following PHR medical experts: Rohini J. Haar, MD, MPH, research fellow at the Human Rights Center at UC Berkeley’s School of Law; Parveen Parmar, MD, MPH, chief of the Division of International Emergency Medicine and associate professor of clinical emergency medicine at the University of Southern California’s Keck School of Medicine; Rupa Patel; Satu Salonen, faculty physician and refugee clinic assistant director, Family Health Center of Worcester, MA and clinical instructor, University of Massachusetts; Homer Venters, MD, MS, former PHR director of programs; and Karen Wang, MD, MHS, instructor of medicine at Yale University School of Medicine. They worked with a team of local fixers and interpreters who remain anonymous for safety reasons.
Staff of PHR contributed to the writing and editing of this report, including DeDe Dunevant, director of communications; Phelim Kine, deputy director of programs and director of research and investigations; Donna McKay, executive director; Tamaryn Nelson, senior researcher; Elsa Raker, program assistant; and Susannah Sirkin, MEd, director of policy.
External review was provided by a range of experts in the fields of medicine, law, and human rights in Myanmar, including Laurie Ahern, president, Disability Rights International; Cristián Correa, senior associate, International Center for Transitional Justice (ICTJ); Andrea Gittelman, program manager, Simon-Skjodt Center for the Prevention of Genocide; Elena Naughton, program officer, ICTJ; Adam Richards, MD, PhD, MPH, PHR board member and assistant professor in the Division of General Internal Medicine and Health Services Research at University of California, Los Angeles; and Eric Rosenthal, executive director, Disability Rights International.
The report was edited by Claudia Rader, MS, PHR senior communications manager and prepared for publication by Claudia Rader and PHR communications interns Theresa McMackin and Angelica Rossi-Hawkins.
PHR would also like to acknowledge the support of MedGlobal in conducting forensic examinations and is grateful to all local partners who provided support, including Rohingya partner Htike Htike and the Cox’s Bazar-based civil society organization “Friends in Village Development Bangladesh,” who helped coordinate field activities. PHR is especially indebted to the Rohingya people who were willing to share their experiences for this report. We have used pseudonyms throughout for security reasons.
Endnotes
[1] United Nations Human Rights Council. “Report of the independent international fact-finding mission on Myanmar,” A/HRC/39/64, September 18, 2018, https://www.ohchr.org/EN/HRBodies/HRC/Pages/NewsDetail.aspx?NewsID=23575&LangID=E.
[2] UN Refugee Agency, Bangladesh Operational Update, January 15, 2019, https://data2.unhcr.org/en/documents/download/67736.
[3] Physicians for Human Rights, “Please tell the World what they have Done to Us” – The Chut Pyin Massacre: Forensic Evidence of Violence Against the Rohingya in Myanmar, July 19, 2018, https://rohingya.phr.org/resources/chutpyin/.
[4] World Health Organization, World Report on Disability, 2011, https://www.who.int/disabilities/world_report/2011/report.pdf?ua=1 (p. 4). The International Classification of Functioning, Disability and Health (ICF), adopted as the conceptual framework for this report, defines disability as an umbrella term for impairments, activity limitations, and participation restrictions. Disability refers to the negative aspects of the interaction between individuals with a health condition (such as cerebral palsy, Down syndrome, depression) and personal and environmental factors (such as negative attitudes, inaccessible transportation and public buildings, and limited social supports).
[5] United Nations Human Rights Council, “Report of the independent international fact-finding mission on Myanmar.”According to the UN fact-finding mission, “Thousands of Rohingya were killed or injured. Information collected by the mission suggests that the estimate [by MSF] of up to 10,000 deaths is a conservative one.”
[6] UN Office of the High Commissioner for Human Rights (OHCHR), “Basic Principles and Guidelines on the Right to a Remedy and Reparation for Victims of Gross Violations of International Human Rights Law and Serious Violations of International Humanitarian Law,” December 16, 2005, https://www.ohchr.org/en/professionalinterest/pages/remedyandreparation.aspx
[7] UN General Assembly, “Rome Statute of the International Criminal Court (last amended 2010),” July 17, 1998, http://www.refworld.org/docid/3ae6b3a84.html.
[8] Syed S. Mahmood, Emily Wroe, Arlan Fuller, and Jennifer Leaning, “The Rohingya people of Myanmar: health, human rights, and identity”, vol. 389, issue 10081,(May 2017), 1841-1850:DOI: 10.1016/S0140-6736(16)00646-2.
[9] Republic of the Union of Myanmar Ministry of Health and Sports, “Hospital Statistics Report 2014-16,” Na Pyi Taw, Myanmar, 2018, https://themimu.info/sites/themimu.info/files/documents/Report_Hospital_Statistics_Report_2014-16_MOHS_Jun2018.pdf.
[10] Caregiver Action Network, “Caregiver Statistics,” https://caregiveraction.org/resources/caregiver-statistics#Impact%20on%20Family%20Caregiver’s%20Health.
[11] UN Office of the High Commissioner for Human Rights (OHCHR), “Report of OHCHR Mission to Bangladesh: Interviews with Rohingyas fleeing from Myanmar since 9 October 2016,” February 3, 2017: https://www.ohchr.org/Documents/Countries/MM/FlashReport3Feb2017.pdf (p. 7-13).
[12] Fortify Rights, “UN Security Council: Refer Myanmar to the International Criminal Court,” May 8, 2018, http://www.fortifyrights.org/publication-20180508.html.
[13] Physicians for Human Rights, “Please Tell the World What They Have Done to Us” – The Chut Pyin Massacre: Forensic Evidence of Violence against the Rohingya in Myanmar, July 19, 2018, https://phr.org/resources/please-tell-the-world-what-they-have-done-to-us/.
[14] Physicians for Human Rights, Widespread and Systematic: Violence against the Rohingya in Myanmar, August 30, 2018, https://phr.org/resources/widespread-and-systematic/.
[15] UN Refugee Agency, “Bangladesh Operational Update.”
[16] United Nations Human Rights Council, “Report of the independent international fact-finding mission on Myanmar.”
[17] Much of this section was taken and adapted from the Physicians for Human Rights July 2018 report “Please Tell the World What They Have Done to Us” – The Chut Pyin Massacre: Forensic Evidence of Violence against the Rohingya in Myanmar, July 19, 2018, https://phr.org/resources/please-tell-the-world-what-they-have-done-to-us/.
[18] World Health Organization, International Classification of Impairments, Disability and Health, Geneva, Switzerland, 2001, https://www.who.int/classifications/icf/en/.
[20] Stephanie Nebehay, “UN Calls for Myanmar Generals to be Tried for Genocide, Blames Facebook for Incitement,” Reuters. August 27, 2018, https://www.reuters.com/article/us-myanmar-rohingya-un-idUSKCN1LC0KN.
[19] United Nations Human Rights Council, “Report of the independent international fact-finding mission on Myanmar.”
[21] Ibid.
[22] Poppy McPherson, “Myanmar Rejects ‘False Allegations’ in U.N. Genocide Report,” Reuters, August 29, 2018, https://www.reuters.com/article/us-myanmar-rohingya-un/myanmar-spokesman-rejects-u-n-genocide-report-idUSKCN1LE0AC.
[23] Parveen Parmar, Jennifer Leigh, Homer Venters, and Tamaryn Nelson, “Violence and mortality in the Northern Rakhine State of Myanmar, 2017: results of a quantitative survey of surviving community leaders in Bangladesh”, Lancet Planetary Health 2019: 3: e144-53, (2019), https://www.thelancet.com/action/showPdf?pii=S2542-5196%2819%2930037-3.
[24] Htet Naing Zaw, “Commission Invites Victims of Violence in Rakhine State to Submit Evidence,” The Irrawaddy, December 12, 2018, https://www.irrawaddy.com/news/commission-invites-victims-violence-rakhine-state-submit-evidence.htmlfbclid=IwAR0HLtdervyxJLR9Wtg8CF8Dca9bPcJzne4phUkljHGp489o_5npNrvSkuc.
[25] Human Rights Watch, “Myanmar: Disband Panel on Crimes Against Rohingya – Rakhine State Commission Delays Efforts at Justice; Claim of ‘No Evidence’ Shows Bias,” December 19, 2018, https://www.hrw.org/news/2018/12/19/myanmar-disband-panel-crimes-against-rohingya.
[26] Michelle Nichols, “U.N. Security Council mulls Myanmar action; Russia, China boycott talks,” Reuters, December 17, 2018, https://www.reuters.com/article/us-myanmar-rohingya-un/u-n-security-council-mulls-myanmar-action-russia-china-boycott-talks-idUSKBN1OG2CJ.
[27] Parveen Parmar et al., “Violence and mortality in the Northern Rakhine State of Myanmar, 2017.”
[28] The PHR clinical team used an adapted version of the “The Manual on Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment.” Known as the Istanbul Protocol, this document is available at http://physiciansforhumanrights.org/issues/torture/international-torture/istanbul-protocol.html.
[29] World Health Organization, World Report on Disability.
[30] World Medical Association, World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects, 2013, https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
[31] World Health Organization, “Disability and Health,” 16 January 2018, https://www.who.int/en/news-room/fact-sheets/detail/disability-and-health.
[32] Médecins Sans Frontières (Doctors Without Borders), “Rohingya Trauma and Resilience,” October 8, 2018, https://www.msf.org/rohingya-trauma-and-resilience.
[33] International Crisis Group, “Myanmar: A New Muslim Insurgency in Rakhine State,” Asia Report,no. 283, December 15, 2016, https://www.crisisgroup.org/asia/south-east-asia/myanmar/283-myanmar-new-muslim-insurgency-rakhine-state.
[34] Much of this section was taken and adapted from the Physicians for Human Rights July 2018 report “Please Tell the World What They Have Done to Us,” The Chut Pyin Massacre: Forensic Evidence of Violence against the Rohingya in Myanmar, July 19, 2018, https://phr.org/resources/please-tell-the-world-what-they-have-done-to-us/.
[35] Human Rights Watch, “Burma: End Abuses Against Rohingya,”May 25, 2009, https://www.hrw.org/news/2009/05/25/burma-end-abuses-against-rohingya.
[36] Adrian Edwards, “One year on: Displacement in Rakhine state, Myanmar,” UN Refugee Agency, summary of press briefing, June 7, 2013, http://www.unhcr.org/en-us/news/briefing/2013/6/51b1af0b6/year-displacement-rakhine-state-myanmar.html.
[37] Aman Ullah, “Politics of Changing Colour of Cards,” The Stateless Rohingya, February 3, 2017, http://www.thestateless.com/2017/03/politics-of-changing-colour-of-cards.html.
[38] Megan Specia, “The Rohingya in Myanmar: How Years of Strife Grew Into a Crisis,” The New York Times (New York, NY), September 13, 2017, https://www.nytimes.com/2017/09/13/world/asia/myanmar-rohingya-muslim.html.
[39] Jonah Fisher, “Myanmar’s 2015 Landmark Elections Explained,” BBC News, last modified December 3, 2015, https://www.bbc.com/news/world-asia-33547036.
[40] Shashank Bengali, “Myanmar’s long-suffering Rohingya Muslims hoped that Aung San Suu would make them full citizens. They were wrong,” Los Angeles Times (Los Angeles, CA), April 9, 2017, http://www.latimes.com/world/la-fg-myanmar-rohingya-2017-story.html; “Politics of Changing Colour of Cards.”
[41] “Who Are the Rohingya?,” Al Jazeera, last modified April 18, 2018, https://www.aljazeera.com/indepth/features/2017/08/rohingya-muslims-170831065142812.html#gone.
[42] Fiona MacGregor, “As Tragedy Unfolds in Myanmar, the People’s Heroine Stokes the Flames of Hatred – Foreign Policy,” Foreign Policy, September 2017; Megan Specia, “The Rohingya in Myanmar: How Years of Strife Grew Into a Crisis.”
[43] Alal O Dulal Collective, “Burma’s Muslims and the War on Terror,” The Wire, September 2017, https://doi.org/10.1080/10576100490275094.
[44] “Myanmar Police Claim Rohingya Torched Their Own Homes,” South China Morning Post, September 7, 2017, http://www.scmp.com/news/asia/south-asia/article/2110155/they-burned-their-own-houses-and-ran-away-myanmar-police-tell; Tom Miles, “Myanmar says it would like to see ‘clear evidence’ of genocide,” Reuters, March 8, 2018, https://www.reuters.com/article/us-myanmar-rohingya-rights/myanmar-says-it-would-like-to-see-clear-evidence-of-genocide-idUSKCN1GK2JH.
[45] United Nations Human Rights Council, Report of the independent international fact-finding mission on Myanmar.
[46] Public International Law and Policy Group, Documenting Atrocity Crimes Committed Against the Rohingya in Myanmar’s Rakhine State, September 2018, https://www.publicinternationallawandpolicygroup.org/rohingya-report.
[47] Human Rights Watch. “Burma: Widespread Rape of Rohingya Women, Girls: Soldiers Commit Gang Rape, Murder Children,” November 16, 2017, https://www.hrw.org/news/2017/11/16/burma-widespread-rape-rohingya-women-girls.; Amnesty International, “’They Rape Everyone’: Widespread Use of Sexual Violence in Myanmar,” June 14, 2018, https://www.amnesty.org.uk/blogs/country-specialists/they-rape-everyone-widespread-use-sexual-violence-myanmar.
[48] Interview with Salim Uddin, Balakuli Camp, Bangladesh, July 21, 2018.
[49] Interview with Faizal Islam, Thangkali Camp, Bangladesh, July 21, 2018.
[50] Interview with Anowar Hussein, Balakuli Camp, Bangladesh, July 20, 2018.
[51] Interview with Abu Tayub, Balakuli Camp, Bangladesh, July 20, 2018.
[52] UN General Assembly, “Rome Statute of the International Criminal Court (last amended 2010),” July 17, 1998, http://www.refworld.org/docid/3ae6b3a84.html.
[53] UN General Assembly, “Convention on the Prevention and Punishment of the Crime of Genocide,” December 9, 1948, Treaty Series, vol. 78, https://www.refworld.org/docid/3ae6b3ac0.html (p. 277).
[54] Ibid.
[55] United Nations, Convention on the Prohibition of the Use, Stockpiling, Production, and Transfer of Anti-Personnel Mines and on Their Destruction, 18 September 1997, available at https://treaties.un.org/Pages/ViewDetails.aspx?src=IND&mtdsg_no=XXVI-5&chapter=26&clang=_en.
[56] Human Rights Watch, “Burma: Landmines Deadly for Fleeing Rohingya: Military Lays Internationally Banned Weapon,” September 23, 2017, https://www.hrw.org/news/2017/09/23/burma-landmines-deadly-fleeing-rohingya.
[57] Fasth, Roger and Simon, Pascal (2015) “Mine Action in Myanmar,” The Journal of ERW and Mine Action, Vol. 19, Iss. 2, Article 6, https://commons.lib.jmu.edu/cisr-journal/vol19/iss2/6.
[58] UN General Assembly, “International Covenant on Economic, Social and Cultural Rights, International Covenant on Civil and Political Rights and Optional Protocol to the International Covenant on Civil and Political Rights,” A/RES/2200, December 16, 1966, https://www.refworld.org/docid/3b00f47924.html.
[59] UN Committee on Economic, Social and Cultural Rights (CESCR), “General Comment No. 14: The Right to the Highest Attainable Standard of Health (Art. 12 of the Covenant),” August 11, 2000, E/C.12/2000/4, https://www.refworld.org/docid/4538838d0.html.
[60] Interview with Abu Tayub, Balakuli Camp, Bangladesh, July 20, 2018.
[61] The American Society of Anesthesiologists, “Types of Pain: Injury,” https://www.asahq.org/whensecondscount/pain-management/types-of-pain/injury/.
[62] World Medical Association, “International Code of Medical Ethics,” October 1949, https://www.wma.net/policies-post/wma-international-code-of-medical-ethics/.
[63] Timothy McLaughlin and Shibani Mahtani, “Myanmar’s Buddhists Block Rohingya Muslims from Blood Supplies, Report Says.” The Washington Post, December 24, 2018, https://www.washingtonpost.com/world/asia_pacific/myanmars-buddhists-block-rohingya-muslims-from-blood-supplies-report-says/2018/12/23/d08157c8-02af-11e9-8186-4ec26a485713_story.html?noredirect=on&utm_term=.de1d9fd5b24b.
[64] UN General Assembly, ICESCR.
[65] Michael Safi, “Myanmar Army Shelling Villages in Rakhine State, Rights Group Told.” The Guardian, February 10, 2019, https://www.theguardian.com/world/2019/feb/11/myanmar-army-shelling-villages-in-rakhine-state-rights-group-told.
[66] Thu Thu Aung and Simon Lewis, “‘We Can’t Go Anywhere’,” Reuters.
[67] Food and Agriculture Organization of the United Nations. “Central and Northern Rakhine State Case Study: Revisiting Emergency Response and Recovery Project in Disaster and Conflict Affected Communities,” July 2017, http://www.fao.org/3/I8564EN/i8564en.pdf.
[68] Livelihoods and Food Security Trust (LIFT) Fund and CARE International, Myanmar, Tat Lan Sustainable Food Security and Livelihoods Program: Baseline Assessment, November 2014. Print.
[69] UNICEF. “Rakhine State: A Snapshot of Child Wellbeing,”, https://www.unicef.org/myanmar/Rakhine_State_Profile_Final.pdf.
[70] The World Food Programme, “Myanmar,” https//www1.wfp.org/countries/myanmar.
[71] Shwe Yee Saw Myint, “Labour Discrimination Billion Dollar Detriment to Myanmar’s GDP: NGOs,” The Myanmar Times, December 14, 2012, https://www.mmtimes.com/national-news/3554-labour-discrimination-billion-dollar-detriment-to-myanmar-s-gdp-ngos.html.
[72] Kate Mayberry, “Rohingya Facing ‘Lost Generation’ of Children Out of School,” Al Jazeera, December 12, 2018, https://www.aljazeera.com/news/2018/12/rohingya-facing-lost-generation-children-school-181212082048462.html.
[73] Joshua Carroll, “Myanmar’s Rohingya Deprived of Education,” Al Jazeera, August 4, 2014, https://www.aljazeera.com/indepth/features/2014/08/myanmar-rohingya-deprived-education-201484105134827695.html.
[74] UN General Assembly, ICESCR.
[75] UN General Assembly, “Convention
on the Rights of Persons with Disabilities,
A/RES/61/106, January 24, 2007, https://www.refworld.org/docid/45f973632.html.
[76] Thu Thu Aung and Simon Lewis, “‘We Can’t Go Anywhere’: Myanmar Closes Rohingya Camps but ‘Entrenches Segregation’,” Reuters, December 5, 2018, https://www.reuters.com/article/us-myanmar-rohingya-segregation-insight/we-cant-go-anywhere-myanmar-closes-rohingya-camps-but-entrenches-segregation-idUSKBN1O502U.
[77] Nyan Lynn Aung, “Aid Groups Barred from Rakhine Conflict Zones,” The Myanmar Times, January 14, 2019, https://www.mmtimes.com/news/aid-groups-barred-rakhine-conflict-zones.html.
[78] Amnesty International. “Myanmar: Fresh Evidence of Violations Amid Ongoing Military Operation in Rakhine State,” February 11, 2019, https://www.amnesty.org/en/latest/news/2019/02/myanmar-fresh-evidence-violations-military-operation-rakhine-state/.
[79] Ibid.
[80] United Nations Human Rights Council. “Report of the independent international fact-finding mission on Myanmar,” A/HRC/39/64, September 18, 2018, https://www.ohchr.org/EN/HRBodies/HRC/Pages/NewsDetail.aspx?NewsID=23575&LangID=E.
[81] United Nations General Assembly, Situation of Human Rights of Rohingya Muslims and other Minorities in Myanmar, A/HRC/39/L.22, September 25, 2018, http://undocs.org/A/HRC/39/L.22.
[82] Poppy Elena McPherson and Ruma Paul, “Myanmar Army Chief Must be Prosecuted for Rohingya ‘Genocide’: U.N. Rights Envoy,” Reuters, January 25, 2019, https://www.reuters.com/article/us-myanmar-rohingya-un/myanmar-army-chief-must-be-prosecuted-for-rohingya-genocide-u-n-rights-envoy-idUSKCN1PJ1AK.
[83] United Nations Office of the High Commissioner of Human Rights (OHCHR), “UN Independent International Fact-Finding Mission on Myanmar advances accountability and initiates new investigations,” March 14, 2019, https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=24334&LangID=E.
[84] Htet Naing Zaw,“Commission Invites Victims of Violence in Rakhine State to Submit Evidence,” The Irrawaddy, December 12, 2018, https://www.irrawaddy.com/news/commission-invites-victims-violence-rakhine-state-submit-evidence.html.
[85] Human Rights Watch, Myanmar’s Investigative Commissions: A History of Shielding Abusers, September 2018, https://www.hrw.org/sites/default/files/supporting_resources/201809myanmar_commissions.pdf.
[86] United Nations Office of the High Commissioner of Human Rights (OHCHR), “Myanmar: UN Human Rights Expert to Visit Thailand and Bangladesh,” January 11, 2019, https://www.ohchr.org/en/NewsEvents/Pages/DisplayNews.aspx?NewsID=24060&LangID=E.
[87] Cape Diamond and Timothy McLaughlin, “Myanmar Court Rejects Appeal of Reuters Journalists Jailed Under State Secrets Act,” The Washington Post, January 11, 2019, https://www.washingtonpost.com/world/asia_pacific/reuters-journalists-challenge-conviction-under-myanmar-state-secrets-act/2019/01/11/0c09a4d8-14d7-11e9-ab79-30cd4f7926f2_story.html?noredirect=on&utm_term=.398e8a164e4d.
[88] Todd Pittman, “Myanmar Government Under Suu Kyi Cracks Down on Journalists,” The Associated Press, February 15, 2018, https://www.ap.org/ap-in-the-news/2018/myanmar-government-under-suu-kyi-cracks-down-on-journalists.
[89] Nyan Lynn Aung, “Aid Groups Barred from Rakhine State,” Myanmar Times, January 14, 2019, https://www.mmtimes.com/news/aid-groups-barred-rakhine-conflict-zones.html.
[90] Hannah Ellis-Petersen and Shaikh Azizur Rahman, “Rohingyas to be Repatriated Despite UN Genocide Warning,” The Guardian, October 30, 2018, https://www.theguardian.com/world/2018/oct/30/bangladesh-and-myanmar-agree-to-start-rohingya-repatriation-in-mid-november.
[91] UN News, “Halt ‘Rushed Plans’ to Return Rohingyas to Myanmar, Pleads UN Expert Fearing Repeated Abuses,” September 7, 2018, https://news.un.org/en/story/2018/11/1025161.
[92] Thu Thu Aung and Simon Lewis, “‘We Can’t Go Anywhere’,” Reuters.
[93] Ibid.
[94] Physicians for Human Rights, “PHR to UN Rapporteur: Press for Rohingya Safety and Justice,.” January 16, 2019, https://phr.org/news/phr-to-un-rapporteur-press-for-rohingyasafety-and-justice/.
[95] Stephanie Nebehay, “U.N. Envoy Fears ‘New Crisis’ For Rohingya if Moved to Bangladesh Island,” Reuters, March 11, 2019, https://www.reuters.com/article/us-myanmar-rohingya-un/u-n-envoy-fears-new-crisis-for-rohingya-if-moved-to-bangladesh-island-idUSKBN1QS147.
[96] World Health Organization, World Report on Disability, 2011, https://www.who.int/disabilities/world_report/2011/report.pdf?ua=1 (p. 4). The International Classification of Functioning, Disability and Health (ICF), adopted as the conceptual framework for this report, defines disability as an umbrella term for impairments, activity limitations, and participation restrictions. Disability refers to the negative aspects of the interaction between individuals with a health condition (such as cerebral palsy, Down syndrome, depression) and personal and environmental factors (such as negative attitudes, inaccessible transportation and public buildings, and limited social supports).
[97] The distal phalanges are the bones at the tips of the fingers