
Executive Summary
Since 2021, eastern Democratic Republic of the Congo has experienced an acute escalation in conflict-related sexual violence that has exacerbated suffering from decades of conflict driven by regional tensions among various armed groups and struggles over valuable mineral resources. The reemergence of the March 23 Movement (M23) rebel group in 2021[1] has fueled the crisis, leading to widespread displacement, a weakened health system, food insecurity, and an alarming increase in sexual and gender-based violence. The withdrawal of peacekeeping forces like the United Nations Organization Stabilization Mission in the DRC (MONUSCO) and the East African Community Regional Force (EAC-RF) has raised concerns about further escalating the humanitarian crisis[2].
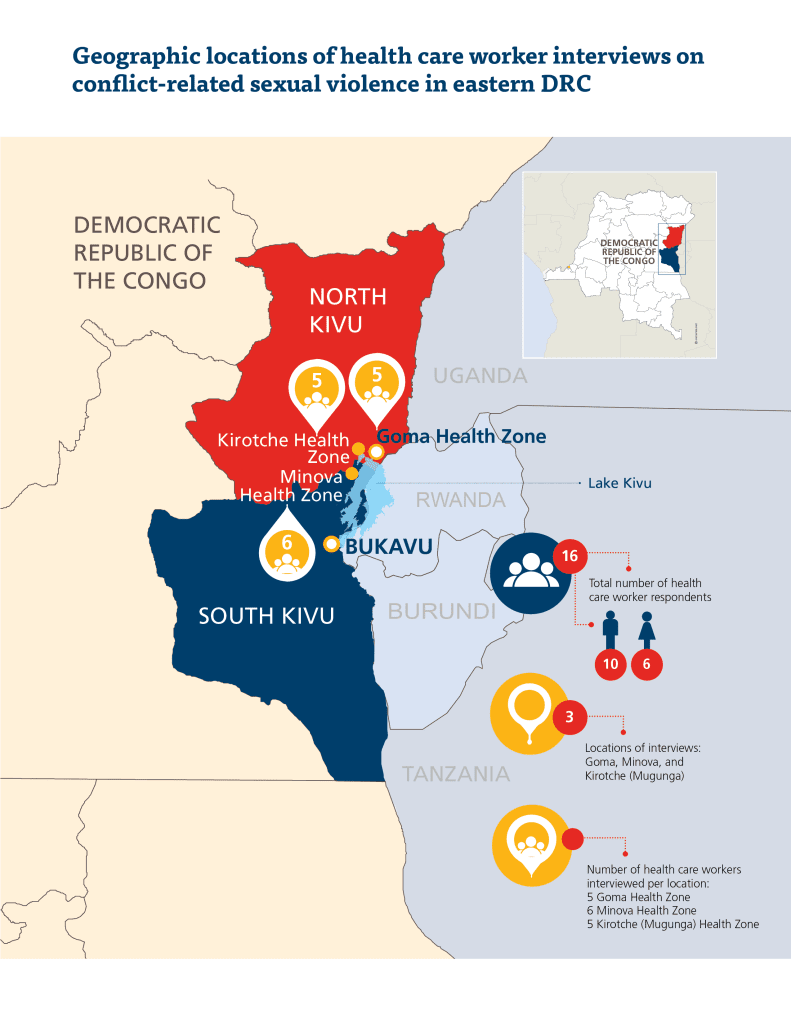
In this report, Physicians for Human Rights (PHR) documents conflict-related sexual violence targeting adults and children in eastern DRC. These findings are based on semi-structured interviews with 16 health care professionals and humanitarian workers in conflict-affected areas of North and South Kivu. These interviews detail the experiences of health care workers as they provided care to survivors using survivor-centered research methodology.
PHR’s research findings establish widespread and severe conflict-related sexual violence – including rape and sexual slavery – and barriers in access to health care and accountability, indicating violations of international human rights law, as well as international humanitarian law.
Health care workers have reported a “massive influx of cases” of conflict-related sexual violence among adults and children. Survivors often sought care following very violent encounters with armed groups, which included armed sexual assault by multiple perpetrators, penetration with foreign objects, and forced captivity. The physical and emotional toll on survivors was complex and long-lasting. Survivors presented at health facilities with a range of medical and psychological needs, including lacerations, sexually transmitted infections, unwanted pregnancies, incontinence, paralysis, post-traumatic stress disorder, depression, and developmental delays. In describing the complex trauma seen in their clinic, one health care worker reported that survivors:“They may undergo physical traumas, organ [traumas], destruction…of the genitalia… sexually transmitted diseases that endanger their lives, their future. They can contract unwanted pregnancies. And with those unwanted pregnancies, face the risk of becoming disabled…”
Members of multiple armed groups, including those supported by the DRC’s neighbors and the DRC military itself, were identified by survivors as perpetrators who used sexual violence to instill fear, intimidate, and control affected communities. While violence and displacement caused by armed groups drove survivors away from their communities, clinicians received survivors living in IDP camps who had been forced to travel to insecure areas to access basic resources and who were attacked while searching for food or firewood around IDP camps. As one nurse recounted, “The child had told me that she went to the field in order to look for food. Then, arriving at the field, she ran into two soldiers. Then the soldier told her: I’m going to have sex with you. If you refuse, I will kill you.”
“They may undergo physical traumas, organ [traumas], destruction…of the genitalia… sexually transmitted diseases that endanger their lives, their future. They can contract unwanted pregnancies. And with those unwanted pregnancies, face the risk of becoming disabled…”
Children are frequent targets of sexual violence, with one health care professional reporting treating a survivor as young as three years old. While the patterns of violence against children are similar to those against adults, there are also some indications that the insecurity caused by conflict was seen as an opportunity for acquaintances and others to commit acts of violence against children.
Compounding these challenges, health care providers struggled to cope with the crisis as they experienced supply chain issues and severe human resource constraints which have left them without adequate training, supplies, staffing, or compensation to manage the acute influx of survivors.
The resurgence of violence and related displacement has led to staggering levels of sexual violence, with the UN reporting over 113,000 cases registered in 2023. Documented cases of conflict-related sexual violence more than doubled in the first half of 2024, compared to the same period in 2023.[3] Local health care workers have been central to the response to support survivors of sexual violence by providing medical and mental health care, including medicolegal documentation of sexual violence. However, the conflict has severely strained the DRC’s health care system, which already suffers from a lack of resources and personnel. Attacks on health care facilities have reduced access to essential services, particularly for survivors of sexual and gender-based violence[4]. The ongoing conflict has also increased the incidence of communicable diseases, including mpox – declared a public health emergency of international concern by the World Health Organization (WHO) in August 2024[5] – in the country’s growing internally displaced persons (IDP) camps. The capacity of the DRC health system to respond to sexual and gender-based violence has been compromised, with many survivors unable or unwilling to seek care due to stigma, facility closures, and fear of further violence.
“The child had told me that she went to the field in order to look for food. Then, arriving at the field, she ran into two soldiers. Then the soldier told her: I’m going to have sex with you. If you refuse, I will kill you.”
PHR’s research findings establish widespread and severe conflict-related sexual violence – including rape and sexual slavery – and barriers in access to health care and accountability, indicating violations of international human rights law, as well as international humanitarian law (IHL). The report calls for coordinated efforts by the DRC government, other parties to the conflict, regional and international actors to take urgent action to prevent the use of sexual violence in war and improve security and access to essentials in IDP camps. The study emphasizes the urgent need for better medical care, psychosocial support, and forensic documentation to address conflict-related sexual violence while highlighting the challenges faced in the health sector. Despite the DRC government’s creation and adoption of laws and policies to provide access to justice for survivors and reparations, no further steps have been taken to implement them. There is an immediate need to strengthen monitoring, investigation, and documentation of conflict-related sexual violence, and to promote accountability and justice for violations by all parties.
PHR makes the following recommendations:
To all parties:
- Fully comply with IHL and international human rights law (IHRL) in all aspects of operations throughout the conflict.
- Ensure that local armed forces and police forces, as well as various armed groups involved in the hostilities, do not engage in sexual violence, including by issuing clear directives prohibiting such violence, investigating and removing from service known perpetrators, and referring the perpetrators of these crimes to the appropriate courts to combat impunity.
- Implement the priority actions contained in regional diplomatic efforts, including the Luanda Process and the East African Community (EAC)-led Nairobi Process with a view to promote de-escalation and create the conditions for lasting peace in DRC, the repatriation of all foreign armed groups and foreigners, and compliance by local armed groups with the DRC’s Disarmament, Demobilization, Community Recovery and Stabilization programme.
To the government of the DRC:
- Take all measures to prevent sexual violence and establish conditions to enable IDPs to return to their living environments, including multisectoral coordinated care for survivors, emergency humanitarian aid and community recovery.
- Immediately improve access to food and firewood or cooking fuel inside of camps to prevent sexual violence against IDPs that occurs outside of the camps.
- Strengthen security in and around routes where displaced populations are fleeing and within the IDP camps to prevent sexual violence.
- Ensure survivors’ access to justice and reparation for conflict-related sexual violence.
- Support survivors who wish to report conflict-related sexual violence.
- Investigate, remove from service, and prosecute actors responsible for violations of IHL and IHLR including Congolese military and political figures, through the judicial services of the DRC.
- Ensure accessible, available, acceptable, and quality health care for survivors of sexual violence, including post-rape care and prophylaxis, sexual and reproductive health care including stigma-free abortion care, mental health care, and child- and adolescent-friendly care.
- Take all measures to cooperate with regional and international legislative bodies to seek accountability and justice for human rights violations.
To the international community:
- As committed by DRC in the June 2024 Security Council session, refrain from authorizing the withdrawal of MONUSCO in North Kivu until progress is made to de-escalate the fighting and instability and when violence has come down meaningfully. And ensure robust monitoring of the situation in South Kivu where MONUSCO withdrawal has occurred, including rates of conflict-related sexual violence in border areas between North and South Kivu.
- Fully fund the 2024 DRC Humanitarian Response Plan[6], including the prevention of sexual violence by strengthening the provision of basic necessities (food, cooking fuel, and others) in IDP camps and by supporting survivors’ healing and access to justice through materials and training for post-rape care, forensic documentation of sexual violence, and comprehensive health care for survivors including mental health, infectious disease including mpox and sexually transmitted infections, and sexual, and reproductive health care.
- Increase international human rights cooperation and support to the government of DRC to promote stronger documentation and evidence-gathering of grave human rights abuses, with a special focus on conflict-related sexual violence and medicolegal documentation and care.

Background
The DRC has a long history of internal conflict and regional tensions amongst numerous armed groups driven, in part, by struggles to control valuable mineral assets[7] , ethnic tensions[8], regional political dynamics[9], and aggravated by intervention by neighboring States[10], which have resulted in wide-reaching impacts including a death toll estimated to be in the millions[11], mass displacement[12], a weakened health system, food insecurity, and sexual and gender-based violence against men, women, and children.[13] Since 2022, the resurgence of the M23 rebel group has significantly escalated the conflict in the region and has pushed rates of displacement and sexual and gender-based violence to record levels. Originally active between 2012 and 2013, when the group occupied the city of Goma in eastern DRC, M23 re-emerged in late 2021 following failed peace discussions. Despite regionally led peace talks and ceasefire agreements, M23 has continued to be involved in ongoing clashes with the Congolese military, displacing thousands and exacerbating the humanitarian crisis. M23’s resurgence has drawn regional attention, with accusations of external support from other states, further complicating peace efforts in eastern DRC. In addition, the growth of foreign investment for the exploitation of natural resources in the DRC and the explosion of illicit trade of precious minerals has fueled territorial tensions in the region and financially funded the growth of rebel movements in recent years, notably, reports have said that M23 has also been accused of smuggling minerals out of the DRC.[14] The UN has expressed concern about “the heavy fighting …between M23, alongside the Rwanda Defence Force (RDF), and the Armed Forces of the Democratic Republic of the Congo (FARDC) together with the Wazalendo coalition of local armed groups, the sanctioned Forces démocratiques de libération du Rwanda (FDLR), and Burundi National Defence Force troops.” The UN Group of Experts on the DRC note that Uganda has not prevented the presence of M23 and RDF troops on its territory or passage through it and sources witnessed Ugandan soldiers crossing into the DRC … and operating in M23-controlled areas.[15] More armed groups have since moved into the region and now over 120 militia groups occupy the eastern DRC with the Congolese army (the FARDC) frequently employing them as proxies in close combat with M23[16]. They include the Nyatura (an umbrella term for predominantly Hutu self-defense militias who fight against M23, and various Mai-Mai groups opposed to the presence of Rwandophone Hutus in eastern DR Congo), Kinshasa-hired eastern European mercenaries[17]. Moreover, international stabilization and peacekeeping forces have also operated in the region, including MONUSCO, EAC-RF and more recently the Southern African Development Community Mission in the DRC (SAMIDRC)[18].
In November 2023, the newly elected Congolese government signed a memorandum calling for MONUSCO to cease operations in the DRC. As of June 30, 2024, MONUSCO had already pulled all but essential personnel from the province of South Kivu. There is widespread concern that MONUSCO’s departure, scheduled to be complete by the end of 2024, will further escalate the humanitarian emergency and leave vulnerable communities at increased risk.[19] This comes shortly after the EAC-RF began withdrawing from the region after the DRC government chose not to renew the force’s mandate in 2023. The EAC-RF was replaced at the end of 2023 by a force from the Southern African Development Community (SADC), but there have been concerns regarding the SADC’s ability to tackle M23 and the continued resistance to pursuing non-military solutions in the region.[20]
Public Health
The ongoing conflict has affected the health systems, rates of communicable diseases, maternal and child health, and access to services for survivors of sexual and gender-based violence.[21] The DRC has a ratio of 1.05 doctors, nurses and midwives per 1000 population, significantly lower than the Sustainable Development Goals index threshold of 4.45 physicians, nurses and midwives per 1000.[22] The health system has also been impacted by facility closures, reduced health care staffing, cost of care, and threat of violence. In 2022, there were 159 attacks on health care facilities, forcing these centers to reduce care provisions or cease operating for up to a month.[23] Attacks on health reduced the number of deliveries occurring at health facilities, decreased the quality of care, and lowered the number of child vaccinations.[24] The already understaffed health system is under additional pressure from previous mpox, yellow fever, cholera, and malaria.[25] In North Kivu, cholera and diarrheal diseases are on the rise in internally displaced persons (IDP) water, sanitation, and hygiene facilities are lacking. The conflict has also dramatically increased reports of sexual and gender-based violence; in the first quarter of 2023, reports of sexual and gender-based violence increased 37 percent as compared to that time in 2022.[26] Survivors of sexual violence often avoid seeking health care because of facility closures, reduced health care staffing, cost of care, threat of violence, stigma associated with sexual violence, and fear of jeopardizing their marriage or other social relationships. Survivors who are able to or choose to seek care often require specialized medical care, psychological care, prenatal or abortion services, and forensic documentation services, in addition to services provided by social, judicial, and legal actors.[27]
Conflict-Related Sexual and Gender-Based Violence
Civilians on the ground have also faced significant conflict-related sexual violence by Congolese forces as well as numerous other military actors as part of attacks on villages and communities, while fleeing violence, and in displacement camps. Due to many factors, including significant cuts in food assistance, gender-based violence cases have increased dramatically over the last year, and M23 has encircled Goma – a humanitarian hub – isolating the city from the rest of the province.[28] Women and children are particularly vulnerable. Women and girls accounted for almost 90 percent of all cases, with incidents of sexual violence against children increasing by 40 percent.[29] In the Bulengo IDP camp, a few miles from the city of Goma, one facility’s medical staff report that an average of five to seven survivors of sexual violence arrive every day for treatment, averaging six child and adolescent survivors of sexual violence under the age of 18 each week.[30] Increased crowding in IDP camps, insufficient humanitarian assistance, and aid distribution policies, as well as underlying poverty and food insecurity, have also exacerbated vulnerabilities to sexual violence and sexual exploitation, including survival sex, including with peacekeeping forces, is well documented and has continued to grow as a coping mechanism and a 2023 mapping project identified 145 brothels in eastern DRC, at least half of which are located in IDP sites.[31] Children are also frequently employed in these brothels and there have been reports of women and girls selling sex for as little as US$0.20.[32] Rates of sexual violence and exploitation have been increasing over recent years with a substantial increase in documented cases from about 40,000 in 2021 to over 113,000 in 2023.[33] Cases of sexual violence, particularly conflict-related sexual violence are expected to continue to rise in 2024 due to the resurgence in violence and increased displacement. United Nations Office for the Coordination of Humanitarian Affairs (UNOCHA) estimates that a staggering 685,000 people are at risk of sexual and gender-based violence and may require specialized care in 2024.[34]
In the face of these staggering levels of sexual violence, local Congolese health workers mounted a robust response to support the health care needs of survivors of sexual violence in North Kivu and surrounding areas affected by conflict in the DRC. Local clinicians and the organizations that they work for are providing IDPs with a comprehensive suite of medical and mental health services, including reproductive health care, access to contraception, and psychological support for the mental health consequences of sexual violence.[35] Local and international organizations have also worked to meet survivors’ basic needs by deploying teams to provide food, hygiene and dignity kits to people living in camps near Goma.[36]
Health care workers have been central to the response to support survivors of sexual violence. Locally trained clinicians have expanded the forensic documentation of sexual violence, including through the introduction of MediCapt, a mobile application to collect and secure forensic evidence of sexual violence.[37] To support the needs of children, facilities have opened child-friendly spaces to help children access holistic care and referrals and children who have experienced sexual violence.[38]Besides, health care workers have joined forces with other sectors including legal and law enforcement professionals in multisectoral networks to collaborate on cases and better implement locally driven responses.[39]
Access to Justice
While the high levels of conflict-related sexual violence persist, access to justice has historically been limited or non-existent for these survivors. In 2023, the DRC government adopted a Draft National Transitional Justice Policy to establish judicial mechanisms to address human rights violations. However, no further steps have been taken yet to operationalize the commitments outlined in the policy.[40] Following a request for investigations into alleged crimes committed by rebels in North Kivu, including M23, the Office of the Prosecutor of the International Criminal Court (ICC) committed to investigate all crimes in its jurisdiction, however it is unclear how these accountability efforts will take place in practice.[41]
Alongside a weak and overwhelmed national justice system, survivors of sexual violence have had limited access to reparations, despite continued promises from national and international actors. Even with the creation of the National Fund for the Reparation of Victims in 2022[42] and national consultations to develop a transitional justice policy, only interim reparations have been available to survivors of conflict-related sexual violence through a non-governmental organizations[43]. Ongoing challenges of victim identification and the lack of transitional justice systems have impeded the DRC government’s ability to address survivor needs and facilitate access to justice. Documentation of conflict-related sexual violence incidents and collection of forensic evidence is carried out but is scattered and often incomplete. There is a lack of coordination amongst the actors involved in the care of survivors and documentation of crimes, primarily due to insufficient training, staff shortages, and limited resources[44].
Against this backdrop of the intensifying conflict, PHR conducted research to understand the recent patterns of perpetration of conflict-related sexual violence in eastern DRC.[45] To document the rapidly deteriorating situation, PHR sought to capture the experiences and needs of health care professionals working to support survivors of sexual violence through their unique perspectives, expertise, and experience.
Methodology
PHR conducted one-on-one semi-structured interviews to capture the experiences of 16 health care professionals and staff working at IDP camps, employed at health facilities and humanitarian organizations, who provided direct services to survivors of sexual violence in the three key health zones in North Kivu and South Kivu provinces affected by conflict-related sexual violence and displacement since March 2022. Qualitative research approaches allowed for the study to capture the experiences, context, and depth of health care worker experiences in DRC, however, it is not able to provide estimates of prevalence or more generalizable typical of data collected using quantitative methods.
In addition, the team complemented these interviews with desk research. To summarize evidence from previously published and unpublished reports, news and media reports, and peer-reviewed studies on the nature and scale of conflict-related sexual violence, attacks on health care and IDP camps and possible associations between attacks on health care and IDP camps and conflict-related sexual violence the study team reviewed published reports in media and reviewed published and unpublished documents from international, national, governmental and non-governmental organizations.
The research team included PHR staff and external experts from the DRC, the United States of America, and France, and other nationalities with expertise in medicine, public health, law, human rights, and investigations as well as physicians who have experience documenting or responding to sexual and gender-based violence in the region. Data was collected in May and June 2024. The PHR Ethics Review Board reviewed and approved the study.
To mitigate vicarious trauma, the team implemented regular meeting sessions, allowing members to debrief their experiences and share emotional support. Interviewers in the field received vicarious trauma training prior to data collection. PHR staff involved in the project regularly participate in vicarious trauma training activities. These strategies helped to maintain the mental health and resilience of the team while navigating potentially traumatic subject matter.
Study Population
Semi-structured qualitative interviews (16) were conducted with health care professionals, and staff working at IDP camps, or humanitarian aid workers in conflict-affected health zones in North or South Kivu such as Minova, Kirotche, and Goma. Inclusion criteria included being an adult health care worker of any discipline, staff working at an IDP camp, or humanitarian aid worker who also has experience working with a population in or around the health zones impacted by conflict after March 2022, the date identified as the start of the current phase of violence. As is standard in qualitative research, the final number of interviews collected as part of this study continued until ‘data saturation’ – or the point at which new themes or information ceased to emerge from the data – rather than quantitative methods for statistical representation to determine the final sample size of 16 health care workers.[46] The health care workers interviewed for this study represent three different health zones in North and South Kivu, six health specialties, and perspectives of both male and female health care workers, providing a diversity of experiences and insights, which are critical for understanding the nuanced impact of conflict on health care delivery in the region (see Table 1 for respondent demographic data).
The selection of health care professionals was a deliberate strategy to capture the unique perspectives of professionals who provided support to survivors. The health care professionals interviewed for this study have extensive experience working with multiple survivors over extended periods, enabling them to identify patterns and trends across their patient populations. Their insights could corroborate and contextualize survivor experiences reported by other sources. This approach aligns with the principles in the Murad Code,[47] as it allows for data to be collected from other sources in a manner that “poses less risk for survivors, and …mitigate[s] over-reliance on survivor information.” Participants were not compensated for their participation in the study.
Informed Consent
Professionals interviewed by PHR as part of this project gave written or verbal informed consent prior to participating in the interview. Study subjects each received a written informed consent form, which was derived from the Global Code of Conduct for Gathering and Using Information about Systematic and Conflict-Related Sexual Violence, also known as the Murad Code.[48] The consent form introduced participants to the researcher collecting the data, outlined the purpose of the study, and explicitly stated the benefits and risks of participation. It was emphasized in the informed consent form that participation in the research was voluntary and based on active, ongoing consent.
Data Instruments
PHR developed a semi-structured interview guide to scaffold questions and ensure that they addressed the domains related to the key research questions. This guide drew from previously developed guides as part of completed projects and published reports in other settings such as Myanmar and Ethiopia.[49] The semi-structured interview guide included questions related to health care and humanitarian workers’ experiences treating patients, child and adolescent survivor experiences, perpetration of human rights violations, challenges in addressing trauma and care, and attacks on health. A brief demographic form was used to capture health professionals’ education, employment, and work experience.
Data Collection and Management
PHR identified and recruited an interviewer, prioritizing clinical experience and training in conflict-related sexual violence research and documentation, as well as familiarity with the methodologies employed. Before interviews began, the interviewer received training on procedures, confidentiality protocols, safety measures, ethical considerations during interviews to minimize re-traumatization, and the specific study aims and sampling methodology. The interviewer was also trained on all the tools and underwent practical training to familiarize themselves with them before interviews began. To ensure that emerging data iteratively informed the interviews with Congolese health care workers. PHR held regular meetings to review interview transcripts to identify additional probes, refine lines of questioning, and strategize ways to enhance the interviews with health care workers. These meetings also assessed the research’s progress towards reaching data saturation and collectively processing interview content, mitigating the potential trauma for the research team, including interviewers in DRC.
After obtaining informed consent, all interviews were recorded, transcribed in French and reviewed by at least two researchers to ensure accuracy. Recordings of interviews were immediately deleted to maintain the privacy, safety, and security of participants. Once transcribed, the interviews were de-identified.
Data Analysis
In accordance with common qualitative research methodology, de-identified interviews were uploaded to Dedoose, a qualitative data management and analysis software for analysis and review.[50] All interviews were coded by at least two researchers in the original language of the interviews, French. Coders used a coding dictionary to provide a consistent way to organize the content within the transcripts for review and analysis. The coding dictionary was flexible and iterative to allow for more codes to be added as new findings emerged from the data. All changes to the coding dictionary were discussed and implemented across coders.
The data analysis comprised a three-step process. First, open coding categorized data within and across interviews into common areas of interest. Second, data were compiled into theme tables to record key themes that emerged from the data. Finally, summaries were created to describe and integrate the key elements within each theme. This process enabled the research team to review the coded data, identify cogent themes and patterns, and create a cohesive narrative responsive to the project’s research objectives and reflective of the data. The analysis process was an iterative and collaborative effort, inclusive of all team members incorporating their diverse and broad areas of expertise.
Limitations
As a qualitative study, the interpretation and analysis of data is subject to interpretation biases introduced by the researchers. The research team was multidisciplinary, drawn from various cultural backgrounds, and worked collaboratively to address potential biases in the interpretation of results. A qualitative inter-rater reliability exercise to check for consistency in the application of codes in the data analysis phase was used to address this potential limitation.
This study is limited to the perspectives of health professionals interviewed for this study. Health professionals interviewed as part of this study can recount their experiences treating survivors of conflict-related sexual violence but are not able to directly share survivor experiences, as they were not typically present at the times when survivors had violent experiences. Study respondents were asked to recall patient histories and their experiences from events dating as far back as 2022, which means that recall bias is inherent in the data presented. However, professionals were able to review notes and other clinical materials at their disposal to refresh their memory.
This study may not be able to capture all forms of sexual violence experienced by survivors in this conflict, as all information may not be divulged to health care workers. For example, survival sex[51] may not be reported to health care workers because individuals may feel they are consenting or that they will face criminal charges for reporting it.
As with all qualitative research, our sample was relatively small and not random. Therefore, there are limitations in terms of the generalizability of this data regarding the experiences of the many health care workers and their organizations involved in the humanitarian efforts in the Democratic Republic of Congo.
Findings
Increase in Sexual Violence Cases
Many respondents in Minova, Kirotche, and Goma health zones interviewed for this study reported a stark increase in cases since 2022.
“If we go back in time, the conflict didn’t start today, obviously, but we started to see a massive influx of cases starting from the year 2023. That’s when the war started really taking on a larger scale… And that’s when we started receiving a lot of rape cases, victims of sexual violence and many other related assaults, but also injured persons… But it’s since 2023 that we’ve seen a real explosion of references to cases originating from these consequences of war.” Nurse working in Goma health zone
“The resemblance, the similarity that we’ve already observed is that during periods of conflicts, of clashes, there’s an influx in cases. The number of cases increases in comparison to the situation in a normal context.” Nurse working in Minova health zone
Survivor Characteristics
Age
The health professionals interviewed for this study described treating survivors of all ages, from adults to children as young as three years. There was a wide range of responses regarding the primary age of the survivors that health care professionals treated, and responses seemed to vary by facility. However, most respondents had experience treating both adults and children on a regular basis.
“Sometimes, it’s under 18 years old, sometimes, it’s 18 years old or older… almost every age is affected.” Public health expert working in Goma health zone
There was a broad age range reported in the patient population, with participants reporting seeing patients as young as three years old. Though most frequently the child survivors seen were between the ages of 12 and 17 years old.
“Children who are most affected by the… sexual violence… are the children at the age of puberty. That’s the age you find from… 13 to 18 years old.” Humanitarian specialist working in Goma health zone
“Well, sometimes, we get children who are victims of sexual assault that are three years old, four years old, five years old, eight years old, it depends” Public health expert working in Goma health zone
Most child survivors were girls although some health care professionals reported rare cases of treating boys who experienced sexual violence, though the general feeling was that boys experience sexual violence, but they do not report it.
“Up until now, since we’ve started the patient care, since the atrocities of the war, we have never found a man. Even though men can get raped, but they do not present themselves [to us].” Nurse working in Kirotche health zone
In general, health care professionals interviewed for this study were unable to speak to specific ethnic or linguistic groups being targeted.
Gender
Most of the health care professionals interviewed reported that the majority of conflict-related sexual violence survivors treated in their facilities were women and girls who had been internally displaced. Gender intersected with other factors, including labor roles, age, displacement status, and economic status to create vulnerabilities to sexual violence. The most common vulnerabilities described by respondents include the lack of firewood and food which forced women and children to go to the fields outside of the camps to gather these resources due to gendered labor roles.
“…many are linked to the conflict because as you know, we are close to the displaced persons camps. Where the displaced people go to get firewood in the park. And there, they run into many armed groups who take them and rape them while they are conducting their activities in the park.” Nurse working in Goma health zone
While male survivors sought services at some facilities, not every health care worker interviewed had received male survivors. Most health care workers described seeing limited or sporadic cases of conflict-related sexual violence against men and boys. However, many health care workers emphasized that they are aware that there are many men who have experienced sexual violence and choose not to come forward due to fear of stigma from health care workers or their community.
“What’s true is that there are men who get raped. But unfortunately, when you see yourself as a man, there are times where you hide a lot of things because you start developing the idea to say, no, maybe they’ll make fun of me as soon as I’ll tell my story, and all that. But I’ve at least seen one dad before…. He had been raped and it was a dad who came to the consultation… But predominantly, men do not come to the consultation, but they are also raped.” Psychologist working in Minova health zone
“Sometimes, we don’t ask for their origin … You see, when someone is traumatized, and you start going deeper into their origin. They’ll tend to wonder: ‘He’s asking me about my origin, what does that mean? Does he not want to treat me anymore, or is there something wrong?’ So, we limit way more the questions that seem more closed and that would cause the cut off of the dialogue.”
Psychologist working in Minova health zone
Survivor Demographics
The survivors seen by the respondents came from a variety of ethnic and linguistic groups. Some of these ethnic groups include Bahavu, Banyarwanda, Bashi, Batembo, Hunde, and Nande. Survivors were identified as speaking Kihunde, Kinyarwanda, Kirundi, and Swahili. However, several health care workers explained that it was challenging to identify a predominant ethnicity of conflict-related sexual violence survivors as they saw survivors from many backgrounds at their facilities.
“Ethnicity, it’s really… we can’t really say that there’s one ethnicity that’s affected, but it’s everybody. Because those that are raped, there are the Bahunde, there are the Banyarwandas, there are the Batembos, there are Bahavus. And so, the one who falls into the trap is always raped. So, we can’t really say that the violence is characterizing or choosing an ethnicity.” A nurse working in Kirotche health zone
“…on a general level, really, all the communities that are there are affected in a proportional manner, if I may say it that way.” Physician working in Minova health zone
Health care workers also sometimes choose not to collect information on ethnicity or geographic origins of the patients to avoid retraumatizing or alienating the survivor. One health care worker explained:
“Sometimes, we don’t ask for their origin … You see, when someone is traumatized, and you start going deeper into their origin. They’ll tend to wonder: ‘He’s asking me about my origin, what does that mean? Does he not want to treat me anymore, or is there something wrong?’ So, we limit way more the questions that seem more closed and that would cause the cut off of the dialogue.” Psychologist working in Minova health zone
Perpetrator Characteristics
All health care professionals interviewed as part of this study reported treating survivors who experienced violence at the hands of multiple perpetrator groups, including governmental military forces, rebel, and militia groups.
Some survivors identified members of FARDC as perpetrators of rape; one health care worker shared a story of a rape:
“There’s a displaced person who was here at the camp. And then there were some soldiers who met her at her home. They entered there and took this victim by force. Afterwards, the victim arrived here with soldiers accompanying her here. And we took care of this case… They were soldiers from the [FA]RDC…Here, in the camp… [of] displaced persons… The assault took place during the night… So, the soldiers had weapons. They were intimidating the victim with the weapons. All three of the soldiers had raped this woman… [The soldiers spoke] …Swahili.” Nurse working in Minova health zone
Some survivors reported rapes perpetrated by Wazalendo groups. Meaning patriots in Swahili, Wazalendo are local militia groups generally affiliated with the DRC government.[52] Some survivors identified Wazalendo as speaking Swahili when reporting to health professionals.
“What we can say with this, there really are rape cases… There are either soldiers, or Wazalendos who intimidate them, and they do whatever they please with them.” Psychologist working in Minova health zone
Other health professionals reported treating survivors who experienced rape at the hands of Nyatura militias,
“They say that it’s the soldiers or it’s the Wazalendos, or it’s the Nyaturas.” Nurse working in Kirotche health zone
Rebels associated with the M23 were reported by multiple health care workers as perpetrators of multiple forms of sexual violence.
“It was three soldiers… well-armed… from armed groups. That’s when she said they were soldiers of the M23… the soldiers had gone to war. She was left on her own… She ran away just like that, she left.” Psychologist working in Minova health zone
Health care workers reported a greater level of diversity of perpetrators of conflict-related sexual violence against children compared to adults. Reported perpetrators included armed soldiers from several armed groups identified above and a limited number of health care workers identified peacekeeping forces, or associated entities as perpetrators of sexual violence. [53]. Clinicians identified others who took advantage of vulnerability and instability to commit these acts. These included teachers, family members, peers, and employers. One health care worker below described UN MONUSCO forces giving “favors” to families in exchange for being allowed to have sexual relations with their children.[54]
“Yes, we admitted at least two who were raped. They came with pregnancies resulting from rapes by their parents.” Nurse working in Goma health zone
“Our military, the UN, MONUSCO. So, the MONUSCO too, sometimes, take the children and give favors to their family so that they consent to relations with the children. All of these are cases of sexual exploitation and sexual abuse.” General physician working in Goma health zone
Despite these accounts that contained specific information identifying perpetrator groups, many survivors were not able to identify perpetrators beyond affirming that they were armed strangers who were either uniformed or tried to conceal their identities.
“Often, the victim has no knowledge and doesn’t manage to identify them. I can just describe to you a little bit how he was dressed. Was it a man in a uniform, was it a civilian? But often, because she’s the one who’s coming from the fields, you get told that they’re hooded men. Hooded, maybe they couldn’t identify. The others are men, they had faces, but they don’t get found. They can describe how he was dressed, his body shape a bit, but oftentimes, they are people the victim has not been able to truly identify” Nurse working in Minova health zone
“The survivors, because today you can’t know to identify the armed groups on the ground. With the multiplicity of armed groups, they all are in military clothing, they all carry weapons. Now identifying them, you can say they may be FARDC soldier, while they are soldiers from Wazalendo or Nyatura, as there are more than 20 armed groups in this entity where women are raped.” Nurse working in Kirotche health zone
While survivors were not always able to specifically identify perpetrators, when asked by health care workers, they were still able to identify certain characteristics. Most commonly, survivors were able to report the language that perpetrators spoke, including Kinyarwanda, Swahili, and Lingala.
“He said that they are soldiers who speak Kinyarwanda. He did not identify this type of soldiers, but he said they speak Kinyarwanda only.” Nurse working in Kirotche health zone
“So, in many cases, the victims are not able to really provide the profiles… But there are some others who respond that the perpetrators spoke either Lingala, or Kinyarwanda… In many cases, we cannot detect the perpetrator’s profiles.” Psychologist working in Minova health zone
A common pattern of perpetration is the use of hoods or masks to conceal the perpetrator’s identity from the survivor.
“No, they don’t know the tormentor… Many say that the tormentors are masked. They are usually masked, and they don’t see the perpetrator, they don’t even see the face. So, they see that they are men wearing military outfits, armed with either rifles or machetes, for instance, but they don’t see the face.” Nurse working in Goma health zone
As noted in the quotation above, the use of weapons is also frequently mentioned in the survivor’s accounts of their experiences. Masked or hooded perpetrators carry out the assault with rifles, guns, machetes, or other bladed weapons. The perpetrator(s) would then often threaten to kill the victim(s) if they do not submit themselves to the rape.
“The survivors arrive, they have been assaulted by an armed man. And when the weapon is pointed at the head of the survivor, the survivor lets herself be used.” Physician working in Minova health zone
Types of Sexual Violence
Multiple Perpetrators
All health care workers interviewed by PHR universally reported having treated multiple survivors who experienced conflict-related sexual violence[55] with rape[56] reported by all respondents. In particular, patients who had experienced multiple perpetrator rape.
“The cases that we receive a lot, are rapes committed by several people and often, they are armed people, so soldiers and the likes of them. But there are also cases of forced sexual acts, without consent. That is found here also, but most oftentimes, they are cases linked to rapes with multiples partners, if I can put it that way, or multiples aggressors.” General physician working in Minova health zone
Use of Foreign Objects
Health care workers often reported survivors presenting with complex physical injuries. One described several physical injuries resulting from penetration with sharp objects:
“Yes, there are injuries linked to sharp objects that can be used during the rape, as it is much more the case during conflicts, during war. There are those perpetrators who use sharp objects such as wood sticks. And from that, we get vaginal lesions, lesions on the perineum, and sometimes complete tear of the perineum. And really, it is the type of lesions that we receive most often.” General physician working in Minova health zone
Types of Sexual Violence against Children
Respondents reported frequently treating child survivors of conflict-related sexual violence to be mostly girls. Children who presented for health care after experiencing sexual violence commonly experienced vaginal rape. Cases of forced marriage, procuring or trafficking, harassment, and sexual assault were also mentioned.
“…When I talk about sexual violence, it’s much more about penetration. … Because there are children who arrive, you see that perhaps…” General physician working in Goma health zone
“Rape, there are others… There is harassment. There are cases of harassment. There are… We also have cases of forced marriage. There are cases of pimping. There are so many forms of sexual violence.” Humanitarian worker working in the Goma health zone
Settings of Sexual Violence
Geographic Location of Reported Attacks
Health care workers interviewed by PHR frequently collect information related to the location of the attacks from the survivors that they treat. Over 18 different locations were flagged by these health care workers as locations where survivors had experienced sexual violence (see Table 2). These include the following: Bitonga, Butondo, Bweremana, Kabase, Kalehe, Karuba, Kashenda, Kituku, Minova, Mubimbi, Mungunga, Ndosho, Ngungu, Numbi, Rusayo, and Soko Boudondo. Within these geographic locations, the site of perpetration is often referenced generally as “the forest” and “the fields” surrounding the displacement camps; these are the most common sites of perpetration mentioned by survivors:
| Table 2: Geographic locations identified by health care workers as sites of reported conflict-related sexual violence | |||
| North Kivu Attacks | North Kivu Origins | South Kivu Attacks | South Kivu Origins |
| Bitonga, Masisi | Kanya Bayonga, Rutshuru | Butondo, Kalehe | Buganga, Kalehe |
| Bulengo IDP Camp, Masisi Nyiragongo border | Karuba, Masisi | Bweremana, Kalehe | Bukavu, Kabare |
| Goma, Nyiragongo | Kiluki, Masisi | Market of Bweremana, Kalehe | Bushushu, Kalehe |
| Kabase (Bahunde chiefdom), Masisi | Health care zone of Kirotshe, Masisi | Market of Kashenda, Kalehe | Bweremana, Kalehe |
| Kanyaruchinya IDP Camp, Nyiragongo | Health care zone of Kitoyi, Masisi | Minova, Kalehe | Kalehe, Kalehe |
| Market of Kituku, Nyiragongo | Masisi, Masisi | Highlands of Minova, Kalehe | Minova, Kalehe |
| Lushagala IDP Camp, Nyiragongo | Mushaki, Masisi | Mubimbi IDP Camp, Kalehe | |
| Masisi, Masisi | Mushenge, Lubero | Numbi, Kalehe | |
| Mushaki, Masisi | Ngungu, Masisi | ||
| Ndosho, Nyiragongo | Rutshuru, Rutshuru | ||
| Rusayu IDP Camp, Nyiragongo | Shasha, Masisi | ||
| Rutshuru, Rutshuru | |||
Rape While Fleeing Violence
Health care workers reported that women often experienced conflict-related sexual violence while fleeing their home and encountering militias, rebels, the FARDC and other armed groups in road to displacement camps.
“Lately, most of the victims confess that the incident happened, mostly in the conflict areas. While they are trying to flee and some others, while they are heading to the field to look for food, they encounter this difficulty there. And others, in their home, because there are victims who stayed in the conflict zones. And when the malefactor run into them there, they sexually assault them.” Nurse working in Minova health zone
“And you see, that with this conflict of war, when they flee, they head towards Minova, but they always tend to return to go look for food in their original environment. That’s how they fall into the hands of these bandits. They rape them in the bush, even on the way, in the bush. It happens sometimes even that they bring them back in their camp and they finish up with them for that many days and leave them.” Nurse working in Kirotche health zone
“Lately, most of the victims confess that the incident happened, mostly in the conflict areas. While they are trying to flee and some others, while they are heading to the field to look for food, they encounter this difficulty there. And others, in their home, because there are victims who stayed in the conflict zones. And when the malefactor run into them there, they sexually assault them.”
Nurse working in Minova health zone
Rape while Seeking Food or Cooking Fuel
Health professionals interviewed for this study frequently shared that survivors reported rapes after leaving camps or their communities to look for food or firewood for cooking in insecure areas nearby. One health care worker spoke about the large number of survivors they see who report sexual violence while looking for firewood.
“Most of them tell us that they were in the bush in order to look for firewood. Especially firewood. Because there are times when we receive even 10 cases of firewood, firewood.” Nurse working in Goma health zone
“There is a case we received the day before yesterday, just arriving from Bitonga. She had gone towards the forest to look for firewood. Once she got there, she ran into unidentified soldiers. Then, those soldiers forced, they took by force and really, they hurt even the outside part and even the inside part of this survivor. We saw that it was really severe [damage/injuries].” Nurse working in Kirotche health zone
Not limited to firewood, survivors also shared with health care workers that they were raped while looking for food. A participant spoke of one survivor in particular who was raped while looking for cassava leaves to eat.
“…a woman who came, who told me she had gone to get food in a field, to pick cassava leaves. And then she was caught by someone in charge, an individual she didn’t know, and he imposed sexual intercourse on her. There, he raped her. When I examined her, I did not find physical traces, but I found that since it had been already two, three days, it was more infections that were developing.” Nurse working in Minova health zone
Survivors frequently reported sexual violence occurring within camps. One health care worker shared a pattern of sexual violence occurring at night and particularly during periods of rain.
“So, in the camps, it happens mostly at night. And when it rains, then it’s more serious because even twice, even three times during the night. Because it’s raining, there is no one to help and all that. It’s complicated in the camps.” Public health expert working in Goma health zone
“…it was raining. There’s a man who came sneaking into the little house, that is, thinking he wanted to take shelter there. But instead, he found the woman on her bed and jumped on top of her. While it was raining, the woman tried to scream, but the people around, as there was heavy rain, people around didn’t realize immediately.” Nurse working in Minova health zone
The lack of security in both communities and camps left survivors vulnerable to repeated experiences of sexual violence.
Rape While Deprived of Liberty
The majority of the health care workers interviewed also shared survivors experienced sexual violence in captivity. In one case, a survivor reported being held for five days and in another case a survivor reported being held in captivity for one month before escaping.
“…she had come from Minova to go look for food in their place of origin, in the high plateau. And as she was coming back, there was a hold-up by armed men who took her to their place of residence. She finished five days and during the five days, she suffered forced sexual intercourse, by five men per day and each according to his will. And when she was released, she found that she did not even have the strength to contain urines. So, she felt that she was already open. And when she came, we tried to run tests. Unfortunately for her, she had already contracted syphilis, that we took care of.” Nurse working in Kirotche health zone
Other forms of Gender-Based Violence
Health professionals interviewed for this study also identified cases of forced marriages happening within IDP camps.
“Forced marriages, there, we receive them starting from the… [prenatal consultation] … A young girl aged 15, she has already married in the camps. That, that’s already a forced marriage.” Public health expert working in Goma health zone
Settings of Sexual Violence Against Children
Often what left adults vulnerable to sexual violence left children at an even higher risk. Children were reportedly raped and experienced other forms of violence by members of armed groups and militants while fleeing their towns and villages on the way to IDP camps, and after having arrived at the camps. Like their adult counterparts, children were often attacked when gathering food or firewood for cooking in the forest or fields.
“The child had told me that she went to the field to get food. Then, arriving at the field, she ran into two soldiers. After, the soldier told her: I will have sexual intercourse with you. If you refuse, I will kill you. Then the child accepted. The soldiers had forced the act.” Nurse working in Kirotche health zone
There were also accounts of children who had been raped alongside their mother while in the fields outside of the IDP camps. In other accounts, rebels and other militants have attacked IDP camps and children have been raped in their tents.
“Currently, in the displaced persons camps, there’s everything. So even children are raped in the tents there. There are others who go to the field with their mothers, they are raped there.” Nurse working in Goma health zone
Children not only experienced sexual violence while fleeing violence, but also faced sexual violence in internally displaced persons camps. Respondents reported that perpetrators of sexual violence against children in camps sometimes included a child’s family members, including parents.
“Yes, we have received at least two who were raped. They had come with pregnancies resulting from rapes by their parents. One had come from Kalehe, another had come from Mungunga. They had come alone to request an abortion.” Nurse working in Goma health zone
Children also experienced sexual violence from their friends, peers, and classmates.
“For the children, the tormentors are often their older friends. They are sometimes the pupils, their classmates. Most of them admit that it is their friends, their classmates, who are the tormentors.” Nurse working in Minova health zone
Several respondents noted that children may take employment in private homes and that their employers perpetrated sexual violence against children by taking advantage of their vulnerabilities, notably absent parents and economic poverty to demand sex in exchange for employment or benefits.
“Yes, we are seeing children that are now being used in environments such as the Ngandas, or they’re being used in homes, restaurants. And there, we think they can be used as workers, but we don’t know what happens in those homes, and since they do not have any means, they can concede their sex. That is a problem already.” Nurse working in Kirotche health zone

“Well, consequences of sexual violence, first of all we have… There are many diseases. There are a lot of diseases linked to sexual violence. There are children who… Well, there are children who are victims of rape. There is also famine because the women are afraid to go get food outside.”
Psychologist working in Minova health zone
Consequences of the Sexual Violence on Survivors
The experiences of sexual violence described above left survivors with numerous physical and psychological consequences.
“Beaten up. Yes, there are even fractures that arrive, even with fractures. Even from machete or from bullet.” Nurse working in Goma health zone
Other physical consequences included sexually transmitted infections, unwanted pregnancies, amongst other physical injuries and conditions:
“Consequences, those who arrive after 72 hours, they have a lot of infections. We see a lot of STIs, sexually transmitted infections. There are unwanted pregnancies that can occur, and much more on a psychological level. They really have psychological disorders. There are even those who go all the way to developing mental disorders to the point of going to psychiatric centers. … There are those who arrive, but who have been sexually and physically assaulted, they arrive with broken bones, with paralysis, with a lot of stuff.” Physician working in Goma health zone
“Even with HIV, we have a lot of cases here that we screen who already carry the HIV due to [sexual] violence.” Nurse working in Goma health zone
Health care workers routinely reported seeing patients displaying severe psychological consequences of violence. Health professionals interviewed for this study routinely reported seeing patients with signs of post-traumatic stress disorder, isolation, shame, self-blame, and depression.
“The consequences are obvious. The cases we see in consultation develop several pathologies. …They develop isolation issues after experiencing these problems. There are precursors that already give us an idea that the patient is already developing a mental problem: isolation, guilt, shame, fear that the event will happen again. From a pathological point of view, there are now major pathologies that are developing: depression. Aside from depression, we also encounter cases that develop post-traumatic stress disorders. There are also cases that develop many other problems, anxiety disorders.” Psychologist working in Goma health zone
While some survivors had complex physical injuries after their assault, many survivors presented without any physical injuries that could be documented.
“The survivors get here; they have been assaulted by an armed man. And when the weapon is aimed at the survivor’s head, the survivor lets herself be manipulated. So, sometimes, for older people that have had sexual relations in the past, maybe with their husband, it’s a little bit difficult to have lesions. Because with the weapon there, when told undress, they undress, sleep, they sleep, spread your legs, straight away they do it. It’s like they were ready to do that thing. So, sometimes many women can arrive and out of ten women, to have just two people who show lesions.” Physician working in Goma health zone
Survivors experienced many consequences of sexual violence that have been outlined above including famine because of fear of returning to the fields outside of the camps and being raped again.
“Well, consequences of sexual violence, first of all we have… There are many diseases. There are a lot of diseases linked to sexual violence. There are children who… Well, there are children who are victims of rape. There is also famine because the women are afraid to go get food outside.” Psychologist working in Minova health zone
“…The impact of the conflict on children victims of sexual violence, in any case, the impact is too severe.You know, first of all, these children, apart from the fact that they may undergo physical traumas, organ [traumas], a nasty destruction of the genitals, they can develop, contract sexually transmitted diseases that endanger their lives, their future.”
Nurse working in Minova health zone
Impacts on Children
Children experienced complex patterns of violence with profound psychological and physical impacts. Physical effects included contracting sexually transmitted infections (notably syphilis), HIV, lesions on the vulva and vagina and other genital traumas.
“But in what happens in cases of minors who have never had sexual intercourse well before, there are so many lesions that can be observed. This is all that is done to a child under the age of 10, under 15, 10 or 12, like that. There are visible lesions, that can be seen in the vulva area. There are others that were traumatized, that were assaulted physically. They can arrive with wounds, bleedings.” Physician working in Goma health zone
“The impact of the conflict on children who are victims of sexual violence, in any case, the impact is too severe. You know, first of all, these children, aside from the fact that they undergo physical traumas, organ [traumas], a nasty destruction of the genitals, they can contract and develop sexually transmitted diseases that endanger their lives, their future.” Nurse working in Minova health zone
Pregnancy resulting from sexual violence was a particular concern for respondents who noted that since the resurgence of the conflict, there has been an increase in pregnancies in girls under age 18. Several health professionals reported treating child patients for unwanted pregnancies. Some participants reported girls being abandoned because they became pregnant following rape. Abortion access was, however, noted to be limited.
“A child who has been sexually abused without finding support, it’s a trauma that destroys their whole life. That destroys their whole life, that can even get to the point of defining their future. …The child thinks this is normal. We even get to… unwanted pregnancies, clandestine abortions, with everything it convenes.” Humanitarian worker working in Goma health zone
“Minors, they are accompanied by their parents. But this one time, a girl had just given birth in the hospital […] in case of a pregnancy resulting from rape, it becomes a headache for the hospital, because it is the hospital that covers this medical care and expenses… it’s as if the family has abandoned the young girl, because the pregnancy is a pregnancy resulting from rape. The perpetrator is not known […]. So, it’s the hospital that bears the weight on its back for the care of this child.” Public health expert working in Goma health zone
In addition to physical health effects, there were multiple psychological health consequences of sexual violence against children. Respondents discuss Post Traumatic Stress Disorder (PTSD), trauma, fears of abandonment, fear of being reattacked, fears of discussing the experience of violence, sadness, depression, anxiety, stress, isolation, distraction, inability to reason, low self-esteem, inability to express oneself, developmental delays, behavioral problems and changes among others.
“The impact on these children’s mental health is that these children seem to be abandoned to their sad fate because their mothers, sometimes, do not know the perpetrators of the rape[s]. These children now find themselves in situations where they are abandoned to their ill fate et sometimes they also develop mental illnesses.” Nurse working in Minova health zone
“Yes, there are definitely developmental delays. Because with the situation they’ve been through, there are some children who become absent-minded. There’s no concentration.” Psychologist working in Minova health zone
One participant described the interconnected and long-lasting impacts of sexual violence on child survivors’ physical, psychological and mental health.
“…The impact of the conflict on children victims of sexual violence, in any case, the impact is too severe. You know, first of all, these children, apart from the fact that they may undergo physical traumas, organ [traumas], a nasty destruction of the genitals, they can develop, contract sexually transmitted diseases that endanger their lives, their future. They can contract unwanted pregnancies. And with those unwanted pregnancies, they’re at risk of becoming disabled in their lives. They will no longer study. Especially since even studying is hard for displaced persons. When to all of this is added an unwanted pregnancy, the girl’s life becomes complicated. At the same time on the psychological level, some develop mental disorders, abnormal behaviors in the community, in life. And I believe that the impact, the consequences, there are numerous ones.” Nurse working in Minova health zone
These accounts speak to both the long-lasting mental health impacts and the stigma and social consequences child survivors may face. Finally, respondents discussed the potential impact of sexual violence on parents’ mental health.
“The concerns are that the parents even have difficulties digesting [processing] these cases. They find that the child is traumatized. But sometimes, the parent or the guardian is also traumatized at the same time as their child because their child was the victim of a rape case. And you find that there is… There’s guilt on the one hand. For example, if a parent has sent the child to fetch firewood and the child becomes a victim, the parent will guilt themselves too. Why did I send them?” Humanitarian worker working in Goma health zone
Delays in Accessing Care
Besides, multiple health care workers spoke of significant delays related to the time of survivors presenting at facilities for care. Some survivors did not present until six months after the assault, due to insecurity related to the conflict and challenges accessing care and social barriers such as fear, stigma, or lack of understanding of the resources available.
“You will see a case, a victim to whom the rape occurred six months ago, who is showing up at the hospital now. … And it’s afterwards that we discover cases like that and so, who stay within the community, unfortunately. And when they get to the hospital, often it’s late and there are not many interventions we can proceed to about it.” Physician working in Minova health zone
“Those that are in society or in the community, many do not seek support. And we received some cases recently who told us: I resigned myself for at least two weeks before looking for support or seeking care. …There are many cases like that, that are referred to us late, beyond 72 hours. And there, taking care of them is a big issue for us, whether it’s on a medical level or a psychological level.” Psychologist working in Goma health zone
Drivers of Conflict-related Sexual Violence
Health care workers interviewed by PHR identified numerous drivers of conflict-related sexual violence that left survivors vulnerable to sexual violence, including insecurity, poverty, and food scarcity. Insecurity took many forms including banditry, troop movements, and militia presence along roadways. Survivors frequently reported having no choice but to enter insecure areas when fleeing, and due to a lack of basic resources in IDP camps.
Insecure areas in and around IDP camps were identified by health care workers as a key factor increasing the risk of vulnerability to sexual violence.
“Yes, because for now, the majority of our patients come from displaced persons camps. Because over there, there is insecurity, especially at night, it’s a bit complicated. So, in the morning, if there is a case that exceeds the plateau at the camp level…” Public health expert working in Goma health zone
Some health care workers also identified insecurity within communities as drivers of sexual violence in conflict-affected areas of North and South Kivu. Insecurity in terms of banditry, troop movements, and militia presence along roadways led to experiences of sexual violence.
“Cases of rapes exist a lot because as you will notice, there are women that can go to the field and on the way, there are either soldiers or Wazalendos who intimidate them, and they do whatever they want with them. So, in short, we really have women raped here and there. …there is a mother who came lately, here, she said that no, I was raped, because on her plot, there is a road that leads to the mountain where the soldiers keep their bombs, their heavy weapons, there. And as soon as they passed by, they found the mother and took the mother, they went up with her, on the way she was raped.” Psychologist working in Minova health zone
Response to Conflict-Related Sexual Violence: Access and Barriers to Care
Forensic documentation
Forensic documentation services are being provided to survivors by some local health care workers, but most facilities included in this study do not routinely collect forensic medical evidence. Multiple health care workers interviewed pointed to the need for further training and mentorship to support improved forensic documentation at their facility.
“We collect them on the basis of a medical certificate that we have, but the certificate of forensic evidence, we will maybe need accompaniment or training so we can reassure ourselves that really, we do it without failures… Yes, as I’ve said, we don’t have training on filling forensic documents, but also sometimes we face difficulties to fill some of the tools, but with the means we have on board, we try to do what we can.” Humanitarian worker in Goma health zone
Another health care worker described the lack of materials for collecting forensic evidence, including dignity drapes, medical certificates, supplies to collect forensic samples, in addition to the lack of training as a key barrier to the collection of forensic evidence.
“Yes, sometimes we face difficulties in collecting forensic evidence due to lack of equipment for sampling this evidence, but also due to lack of training. We are not informed on the ways to collect this evidence.” A nurse working in Minova health zone
“Consent forms, general information, all that. There aren’t any. There aren’t any.” Nurse working in Kirotche health zone
Even at facilities where the collection of forensic evidence was taking place, challenges related to the collection and analysis of samples due to lack of resources remained. Storage of forensic evidence posed problems for many health care workers interviewed for this study as facilities lacked secure places to store evidence, such as clothing, paperwork, and other important materials and supplies necessary for the forensic evidence collection process.
“You know, the survivors that arrive to you with clothes but already torn up, dirty, shredded. They would need to keep, conserve these clothes that they wear for evidence, but also to be given new clothes, for instance. They would need first of all to be accompanied, even maybe materially a bit, for a time so that she feels considered. But often, she comes… Us, we will only stop at the medication aspect. We only give treatment.” Nurse working in Minova health zone
“Document? I can say yes, because on the consultation form. There is the part where we talk about evidence. Keeping them, we don’t really have an appropriate place to keep them. … First, their collection poses a problem because we don’t have all the means, everything that is necessary to collect this evidence, but also their conservation.” Nurse working in Minova health zone
“Often, there are shortages of medication. Even PEP kits, sometimes, we can lack other means, logistical means.”
A sexual and gender-based violence nurse working in Minova health zone
Lack of Resources
Health care workers almost universally pointed to a lack of general resources in a number of areas that made comprehensive care and treatment of survivors of sexual violence more difficult. Supplies, including medicine, post-exposure prophylaxis (PEP) kits for HIV prevention, and forensic evidence collection supplies (discussed above) were frequently cited as missing. In particular, PEP kits were identified as sometimes missing.
“We’ve observed that if there is no assistance in PEP kits and other essential medicines, really, the population has to suffer from this bad behavior.” Nurse working in Kirotche health zone
“Often, there are shortages of medication. Even PEP kits, sometimes, we can lack other means, logistical means.” A sexual and gender-based violence nurse working in Minova health zone
Furthermore, one facility reported missing HIV testing kits for routine testing and treatment.
“Yes, well, difficulties in relation to medical care, for now, it does not pose a problem. But sometimes, we’re missing tests for HIV. When we need to do the tests and we do not have any, it is a difficulty. That is in relation to medical care.” Humanitarian specialist working in Goma health zone
In addition to the lack of funds for key supplies and materials, resource challenges also had an impact on the kinds of services available. One health care worker described how some facilities continue providing free care and support – despite the lack of resources for programming – even at great cost to the facility, however it was unclear how long facilities can continue to do so without additional funds.
“Fortunately, lately, since the war started, here, the care, we provide care to the displaced persons and all other categories for free without even support. That is also a difficulty we are facing, because with the structure not being supported, we do not know what to do. At the same time our brothers who came from Masisi and Rutshuru and elsewhere, they need care. They are unable, in a state of vulnerability where they cannot pay for care. Us, we sacrifice the care ourselves to tell them they do not pay today.” Nurse working in Minova health zone
Unwanted Pregnancy, Access to Abortion Care and Emergency Contraception
Pregnancy was noted as common amongst survivors. Health care workers reported multiple challenges in caring for survivors with children resulting from unwanted pregnancies, as well as facing malnutrition, housing barriers, lack of psychosocial support, and limited access to pre and antenatal care.
“During the consultation, the midwives, the nurses notice that the mother is crying. So, they wonder why. And while trying to dig deeper, they observe that the mother is crying because of the burden of this child. And that in truth, at home, she has nothing to eat. And no one is helping her to take care of that child. That’s when the nurse notices the child is the result of a rape. … The child is already six months old. He’s already six months old. And the need of the mother was what? To separate from this child because he is a burden now. She can’t take it anymore. There is nothing to give him, there is no food. Even housing, the mother relates that the child spends the nights with the mother under the stars, meaning next to the shops, in the street. So, she wanted this child to have a taker, someone who needs to adopt him at least, because she can’t stay with that child anymore… Psychologically, it had disturbed her.” Psychologist working in Goma health zone
Another health care worker pointed to the complex challenges mothers who have children born of rape face in their communities.
“They are almost discredited and abandoned. They are not acknowledged by their family. They are people that are always neglected. On the economic level, they have no activity because she was raped when she was a minor or here, she was even an adult woman of the household, but who was raped and was rejected by the husband. She remains alone trying to find ways to feed this child.” Nurse working in Minova health zone working
In the face of high levels of unwanted pregnancies and social stigma facing unwed mothers, health care workers reported some instances where survivors asked to terminate the pregnancy or expressed desire to no longer be pregnant. They reported that access to abortion care for survivors of sexual violence varied from site-to-site with services being offered at some locations and other locations did not have adequate supply of emergency contraception due to the lack of PE kits or for facilities with a religious affiliation they did not offer abortion care. At other health institutions where abortion access was unavailable, survivors may be referred to other places where they could access this service.
“If it happens that the survivor suggests an intervention, on our end, we make a referral to where there is a package in relation to care. That’s what we do. You know, religious faith, it’s a little complicated compared to other structures. So, we redirect, make a referral to where the package is available.” Public health expert working in Goma health zone
At some facilities, survivors were sometimes given counseling to discourage them from seeking an abortion if they expressed a desire to terminate the pregnancy. One health care worker described an example of this practice.
“… We put in place psychoeducation to show her that… We guided her, we can’t make the decision for her, but we guided her on how she could bring this child into the world. There is time, we even apply an acceptance therapy so she can settle with that. … we discourage them from aborting.” Psychologist working in Minova health zone
Impact of the Crisis on Health Care Workers and Human Resource Constraints
Health care workers frequently reported that the conflict’s scale and gravity has taken a toll on them. They described how they were overwhelmed with the number of patients they see.
“Sometimes, we are affected when we’re overwhelmed. We see cases that really overwhelm [us]. Because there are cases of sexual violence for which you start wondering: are they humans, are they animals. Sometimes, it suffuses, and it really affects the person’s mood.” Public health expert working in Goma health zone
One health care worker described how the volume of survivors they saw had a great impact on their own wellbeing and suggested mental health programming to help health care workers navigate how they are impacted by the crisis.
“Yes, as a health care worker, really, I would like to add something. It is related to the psychological state of us also, staff, caregivers, because it affects us too, when you see the cases really increasing in high numbers like that, it affects us. It affects us a lot…” General physician working in Minova health zone
In addition to mental health care and support, health care workers often pointed to human resource challenges that affect their ability to provide patient care. Some health care workers pointed to lack of pay as a factor that is disincentivizing health care workers who support survivors.
“Yes, on the funding side, there is an impact. Because the human resources are available, the medicines are available, but there is no motivation for the staff who takes care of these victims.” Nurse working in Minova health zone
Pay was not the only factor impacting the ability of health care workers to treat survivors. The health care workers indicated that lack of clinical training on survivor care and forensic documentation is a key human resource constraint.
“Well, we have human resources, but who also lack training[s], because everyone, in this context should go through training…. We have personnel who should help to receive and know many cases or to have many cases who were raped and stay within the community, but who are not trained.” Nurse working in Kirotche health zone
Good Practices in Service Provision
Despite the immense challenges identified by health care workers – including lack of resources and a surge of cases – clinicians and health facilities have found collaborative and innovative ways to provide support and services to survivors. One emerging good practice to tackle the stigma and mental health challenges for survivors has been the development of safe spaces. One clinician shared the initiative their facility has taken to establish a safe space for women who have experienced sexual violence to meet and discuss their experiences:
“So, for the women, women didn’t have a place where they could go to discuss, to talk about their stuff. … So, that’s why our project thought of creating a space where women can come, talk about what’s happening to them and what they do, and feel safe. So, the safe space is where there is safety. They can talk about their stuff here and there’s not going to be any infiltrators or things that can leak out. That’s it. So, they feel good when they come here to discuss their matters.” Psychologist working in Minova health zone
Several clinicians also referenced the strong referral pathways to support services within their facilities and with other facilities and organizations. These referral pathways have made it possible for clinicians to send their patients to trained and specialized professionals to address their unique needs resulting from the conflict. This has allowed for more comprehensive care for survivors to address their needs – both physical and psychological.
“For the psychological state, thankfully, we organize it before the care, we must go through counselling always. We have the APS who are trained but also the organizations that help us in the care, they have APS too, they have psychologists. This is how we try to put the victims back in their own frame. But their psychological situation is not always good because they incriminate the fact that if the war wasn’t happening, they would not fall into these pictures of violence. So, they are not well at all, despite the fact that they are still in houses, in foster families, in schools. They are still in the entities, and they don’t know when they will be able to return to their original environment, with this war that does not want to end.” Nurse working in Kirotche health zone
And despite the growing needs for increased training and resources for forensic documentation, several facilities are establishing strong practices and policies for secure collection and documentation of medical-legal evidence. While there are still challenges to address, clinicians discussed the use of tools, such as the forensic medical certificate, that have helped them more comprehensively document forensic medical evidence. Another clinician spoke about using technology to support forensic medical documentation of sexual violence, as an innovative approach they use to document forensic evidence medical evidence of sexual violence.
“…We do a collection correctly because we have elements for collection. We have our forensic certificate. We have… the… software… that helps us collecting forensic evidence. …we have our documents for the collection, so we still do it anyway.” Physician working in Goma health zone

Analysis
Clinicians interviewed for this study report that violence has increased dramatically in North Kivu and South Kivu since 2022. This has resulted in a surge of cases of conflict-related sexual violence in a region that has experienced over 30 years of these violations. Clinicians frequently report a growing trend of receiving patients who have experienced multiple forms of conflict-related sexual violence, including multiple perpetrator rape, rape with foreign objects, which has resulted in a host of physical and psychological impacts, including sexually transmitted infections, unwanted pregnancy, incontinence, isolation, and post-traumatic stress disorder in addition to other long term psychological impacts.
Despite the “massive influx of cases”[57] of sexual violence seen by clinicians interviewed by PHR, the study’s findings also point to a potentially large number of survivors who have experienced sexual violence but who have not accessed care, support, or medicolegal documentation services. Clinicians frequently reported that the survivors who presented at health facilities were typically in need of care for acute medical needs, such as prenatal care, pregnancy termination, HIV testing and treatment, mental health and psychosocial support for complex trauma. The fact that most clinicians reported survivors presenting at facilities with acute injuries combined with the intense stigma faced by survivors suggests that there may be many more survivors who could not access care or did not access care due to the lack of physical injuries following sexual violence. This implies that there may be a potentially large number of survivors who have not reported their experiences of sexual violence, have not sought medical care, or been able to access post-rape care or services.
While no one actor was identified as the sole perpetrator of the violence, clinicians interviewed by PHR identified multiple armed groups that used sexual violence to fuel fear, intimidation and exercise control amongst affected communities. Survivors reported conflict-related sexual violence as being committed by Swahili, Lingala and Kinyarwanda speaking perpetrators. Furthermore, clinicians also identified instances where the UN, MONUSCO forces, or their associated civilian agents committed sexual exploitation and abuse against children.[58] In addition to UN actors, clinicians interviewed by PHR also identified others, including teachers, family members, peers, and employers, who took advantage of vulnerability and instability to commit sexual violence against children. One respondent below described UN or MONUSCO forces giving “favors” to families in exchange for being allowed to have sexual relations with their children. These accounts are consistent with other reports, including the recent report that eight MONUSCO peacekeepers were accused of sexual misconduct in October 2023.[59] There were 224 documented reports of sexual exploitation and abuse by MONUSCO forces between 2010 and 2021.[60]
Additionally, armed actors took advantage of the vulnerability created by protracted fighting to commit sexual violence with impunity. Most notably, this study noted no difference in patterns of perpetration of the crimes across groups nor did the data show patterns of how specific groups targeted affected populations which points to a need for additional research. That being said, multiple drivers of conflict-related sexual violence, including insecurity in communities, on roadways, in and around camps, and economic insecurity placed survivors in situations where they were particularly vulnerable to violence. Clinicians almost universally reported that survivors experienced sexual violence while searching for food or firewood. This report shows that there are no safe spaces for civilians to go to as they face sexual violence in their communities, along the roadways as they seek safety, and in internally displaced person camps. The gendered vulnerabilities associated with gathering firewood are well-documented as women and girls are often exposed to sexual and gender-based violence when gathering food and firewood.[61] [62] In DRC, Médecins Sans Frontières has reported that the majority of survivors describe sexual violence occurring “while searching for food or firewood outside of the displacement camps.”[63] While sexual violence occurs at the hands of a variety of actors, the root factors that drive conflict-related sexual violence include the security of roadways and communities, food insecurity , and the security of displaced persons camps.
DRC has the world’s largest population of food insecure people with 6.5 million people experiencing food insecurity in Ituri, North Kivu, and South Kivu. Furthermore, the lack of services to support citizens experiencing insecurity and displacement due to conflict with necessary humanitarian aid such as food, cooking fuel, health services and other resources, creates a self-perpetuating cycle of vulnerability to sexual violence which we see in the number of respondents who shared stories of patients who had experienced sexual violence at multiple times.
This study draws important attention to the sexual violence experienced by children in this conflict. Clinicians reported treating children of all ages who have experienced rape, forced marriage, and forced pregnancy. The drivers of sexual violence against children in this conflict were similar to those of adults but were heightened by children’s specific vulnerabilities based on their age and gender. As well, the range of perpetrators shared by clinicians for cases of sexual violence involving children, indicates that in some instances the insecurity caused by conflict was seen as an opportunity for acquaintances and others to commit acts of violence against children. Clinicians interviewed for this study almost universally reported providing post-rape care to child survivors who experienced complex patterns of violence and presented with compounded physical and mental health impacts of the violence, including sexually transmitted infections, unwanted pregnancies, long-lasting trauma, and physical injuries, including on survivors’ genitals. Clinicians reported using emerging good practices for engaging with children, notably child-friendly spaces, but resources to support more child-focused programming to ensure children have access to tailored care and psychosocial support services to address the immediate and long-term impacts of the violence were still seen as lacking.
The study also provides insight into the profound needs related to medical care and services related to post-rape care and support for survivors of sexual violence. Many clinicians reported outages – ranging from sporadic to frequent – of key medical supplies that are key to patient care, such as HIV testing kits, PEP kits, and key medicines. These supply chain challenges are coupled with severe human resource constraints which leave health professionals without the training, staffing, and pay to manage such an acute influx of survivors. As of the date of publication, the United Nations Office for Coordination of Humanitarian Affairs is reporting a significant gap in the amount of funds needed for the humanitarian response in DRC versus the amount of funds allocated for the response underscoring the gap in resources needed to support survivors, prevent conflict-related sexual violence, and ensure millions of people can access the lifesaving support that they need.[64]
In particular, this study finds that forensic documentation of sexual violence is only happening at some – but not all – facilities where survivors seek care, pointing to challenges in documentation and a need for more investment in training and resources to facilitate medicolegal evaluations and evidence collection. Forensic documentation services are an essential part of post-rape care and are part of the United Nations Joint Global Programme on Essential Services for Women and Girls Subject to Violence, a partnership by UN Women, United Nations Population Fund (UNFPA), WHO, United Nations Development Fund (UNDP) and The United Nations Office on Drugs and Crime’s (UNODC) Essential Services package for women and girls subject to violence. To ensure that crucial forensic documentation services are routinely offered to survivors, training and funding are required to ensure clinicians are able to collect, document, preserve, and transfer key evidence. A forensic medical certificate of sexual assault – a standard documentation tool for clinicians to use to systematically document forensic medical evidence of sexual violence – was nationally recognized in the DRC in 2022. Additional support is needed to ensure that all professionals are trained in its use and have the requisite supplies to properly collect, document, store, and transfer forensic medical evidence. Moreover, some clinicians interviewed were not trained on the specificities of conducting medicolegal investigations with pediatric and adolescent populations- highlighting both a need for additional training for clinicians and the possibility that some children may not have access to appropriate forensic documentation, due to distance and lack of knowledge of the availability of those services.
In addition to the needs of survivors and the health system, support for clinicians who are front-line first responders engaging with survivors must be central to all responses to the conflict. Often working with little to no pay, clinicians report experiencing vicarious trauma from working with survivors of sexual violence who have experienced complex trauma and brutal injuries. To manage this exposure to trauma, clinicians requested psychosocial support and training on coping with exposure to trauma for themselves.
While access to abortion care is legal in the DRC, this study shows that these services are not always available to survivors who express a desire to terminate an unwanted pregnancy. A variety of factors contributed to the inability of survivors to avoid pregnancy or access abortion care, including a lack of emergency contraception at the facility or the referral of women expressing a desire for abortion care to counselling. These factors meant that pregnant survivors of conflict-related sexual violence who wish to terminate their pregnancy are not always able to access abortion care or pregnancy termination despite DRC’s obligations under the 2008 ratification of the Maputo Protocol and the 2018 Public Health Law.[65] The need for access to safe abortion for survivors of conflict-related sexual violence in DRC is great. The lack of services and supplies has a profound impact on women; the DRC has one of the highest maternal mortality rates in the world[66] and it is estimated at least 10 percent of maternal deaths each year are due to complications from unsafe abortions and 74 percent of Congolese women aged from 15 to 49 have an unmet need for contraception. As of September 2023, the United Nations Population Fund estimated that there were at least 220,000 pregnant and displaced women in this conflict who lack secure access to health care.[67] 2.2 million pregnant and breastfeeding mothers suffered from acute malnutrition in 2023 in Ituri, North Kivu and South Kivu provinces.[68]
Challenges in pursuing political solutions have prolonged the growing violence in the DRC. The Nairobi and Luanda processes provide opportunities to advocate for sustainable and non-militarized solutions to the humanitarian crisis.[69] Increased funding for the Humanitarian Response Plan for the DRC is also essential to reducing the risk of further violence for civilians and IDPs in North Kivu. As of September 2024, the Humanitarian Response Plan for the DRC was only 37 percent funded, at US$964.1M million.[70]
Legal Analysis
PHR’s research confirms that conflict-related sexual violence is perpetrated by a range of actors, including the FARDC, M23, which UN experts recently identified as being in the control and acting at the direction of Rwanda, and other Congolese and foreign rebel and militia groups. Our findings establish widespread and severe conflict-related sexual violence – including rape and sexual slavery – and barriers in access to health care and accountability, indicating violations of IHRL, as well as IHL.
This evidence of violations of international law gives rise to immediate obligations for the DRC and other state actors – including Rwanda, Burundi, and Uganda who the UN has identified as playing a role in this crisis – to prevent further atrocities, ensure documentation and investigation of harms, enable accountability and justice, and provide health care including sexual and reproductive health care to survivors. All armed groups must cease the use of sexual violence. To do so, they must issue clear directives prohibiting its use and remove and pursue accountability against members who have engaged in such acts.
| Table 3: Status and Date of Human Rights Article Accession(a), Succession(d), Ratification (r) by Country | ||||
| DRC | Rwanda | Uganda | Burundi | |
| International Convention on the Elimination of all Forms of Racial Discrimination (1965) | 21 April 1976 a | 16 April 1975 a | 21 November 1980 a | 27 Oct 1977 |
| International Covenant on Economic, Social and Cultural Rights (1966) | 1 November 1976 a | 16 April 1975 a | 21 January 1987 a | 9 May 1990 a |
| International Covenant on Civil and Political Rights (1966) | 1 November 1976 a | 16 April 1975 a | 21 June 1995 a | 9 May 1990 a |
| Convention on the Elimination of All Forms of Discrimination against Women (1979) | 17 October 1986 | 2 March 1981 | 22 July 1985 | 8 January 1992 |
| Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment (1984) | 18 March 1996 a | 15 December 2008 a | 3 November 1986 a | 18 February 1993 a |
| Convention on the Rights of the Child (1989) | 21 September 1990 | 24 January 1991 | 17 August 1990 | 19 October 1990 |
| Convention on the Rights of Persons with Disabilities (2006) | 30 September 2015 a | 15 December 2008 a | 25 September 2008 | 22 May 2014 |
| The Maputo Protocol | 9 June 2008 r | 29 December 2003 r | 18 December 2003 r | X |
| The Rome Statute | 11 April 2002 | X | 14 June 2002 | Withdrew 27 Oct 2017 |
| The Genocide Convention | 31 May 1962 d | 16 April 1975 a | 14 November 1995 a | 6 January 1997 a |
Prohibition on Sexual Violence in War, Perpetrator and Command Responsibility, and Obligation to Protect IDPs
Conflict-related sexual violence is a violation of IHL[71], international criminal law[72], and IHRL[73]. In non-international armed conflicts such as DRC, all parties, including state and non-state armed groups, are required to prevent and address sexual violence in accordance with their obligations under IHL, including Common Article 3, Additional Protocol II to the 1949 Geneva Conventions, and relevant Security Council resolutions. Sexual violence in war is prohibited by the requirement of ‘humane treatment’, and by the prohibitions of ‘violence to life and person’, including ‘cruel treatment and torture’ and ‘outrages upon personal dignity’[74]. Serious violations of IHL may constitute war crimes.
Under IHL, states may prosecute individuals for serious violations of the Geneva Conventions.[75] International criminal law also recognizes that commanders of forces led by both state and non-state actors may be held criminally responsible for war crimes by their forces if they knew or should have known about such crimes and failed to prevent them or punish those responsible.[76] All military leaders, whether affiliated with a state or not, have the obligation to send clear directives to their members and subordinates that sexual violence is a violation of the laws of war and unacceptable, and can incur liability individually for ordering, failing to prevent, or failing to ensure accountability for sexual violence. All states involved in the conflict in DRC have the obligation to prevent and prosecute sexual violence by their own state forces as well as non-state actors acting under their control. Further, the DRC authorities have the obligation to pursue accountability even by other parties for all acts of conflict-related sexual violence. Finally, beyond states holding individuals accountable, a state may also be held responsible for the acts of non-state actors in certain circumstances, including where a state has exercised control over the non-state actor, such as where the non-state actor is in fact acting under its discretion.[77]
In addition to IHL, international and regional human rights law requires states parties -including the DRC and other states supporting rebel groups including M23 – to prevent, investigate, prosecute, punish, and provide remedy – including reparations – for sexual and gender-based violence in general, including in conflict[78]. Sexual violence violates several fundamental rights, including the rights to life, health, privacy, torture, and freedom from gender-based discrimination[79]. The DRC, Rwanda, Uganda, and Burundi have signed and ratified numerous human rights treaties (see Table 3) that prohibit sexual and gender-based violence, including the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW).[80] The UN Committee on the Elimination of Discrimination against Women (CEDAW Committee) has clarified in General Recommendations 19, 30, and 35 that CEDAW prohibits gender-based violence [81] including in international and non-international conflict and post-conflict periods[82]. States parties must prevent and redress conflict-related sexual violence, including violence perpetrated by non-state actors[83]. Similarly, the Protocol to the African Charter on the Rights of Women (the Maputo Protocol) establishes that states parties must, “in accordance with the obligations incumbent upon them under IHL, protect civilians including women, irrespective of the population to which they belong, in the event of armed conflict”[84]. Further, the Maputo Protocol requires states parties to protect internally displaced women and girls from “all forms of violence, rape and other forms of sexual exploitation, and to ensure that such acts are considered war crimes, genocide and/or crimes against humanity and that their perpetrators are brought to justice before a competent criminal jurisdiction.”[85]
The obligation to prevent sexual violence, including in conflict, requires addressing risk factors for sexual violence including insecurity, lack of food, and lack of cooking fuel. In particular, States have obligations under both IHL and IHRL to protect civilian populations and IDPs in particular, including specifically from violations of sexual and reproductive autonomy.[86] Furthermore, the African Union Convention for the Protection and Assistance of Internally Displaced Persons in Africa (Kampala Convention)[87], to which the DRC is a party, reinforces that the primary responsibility for supporting and protecting IDPs lies with the state. States must ensure comprehensive protection measures that include preventing sexual violence, providing essential services, and creating a secure environment for IDPs. IDPs are entitled to protection like all other civilians and must not be the object of attack provided they are not directly and actively taking part in hostilities.[88]
Places where IDPs are sheltered are considered protected civilian objects so long as IDP camps must be secured by national and local authorities in accordance with their primary obligation to protect civilians under IHL and in a manner that strictly adheres to international human rights law.[89] IHL specifically establishes that the life, dignity, and humane treatment of IDPs must be respected, requiring protection of their physical and mental well-being as well as freedom from rape and other sexual violence.[90] IDPs are also entitled to enjoy satisfactory conditions of shelter, hygiene, health, safety and nutrition.[91] Similarly, IHRL recognizes that displaced women and girls in particular face risks of human rights violations including sexual violence during flight and in displacement and calls upon states parties to ensure protection of displaced persons’ human rights by ensuring basic services and humanitarian assistance including in “all situations of massive influx of refugee and displaced populations.”[92]
Obligations to ensure survivors’ access to health care and reproductive autonomy
IHRL recognizes that women in conflict-affected areas face heightened risks of sexual violence, sexually transmitted infections, and unplanned pregnancy due to conflict-related sexual violence as well as disruptions in access to essential services. Even during conflict, states parties are obligated to provide basic health services and information, including mental health care and sexual and reproductive health care such as maternal health care, abortion care, STI treatment, and contraceptive services.[93]
Further, IHL requires all parties to a conflict to respect the protection, health, and assistance needs of women affected by armed conflict and establishes special protections for medical personnel and facilities to ensure the functioning of health care throughout a conflict.[94] Civilians in conflict areas have the right to receive humanitarian aid, including medical and other supplies essential to survival[95]. IHL allocates primary responsibility for meeting civilian needs to the state or party that controls the territory in which the civilians are located,[96] which in this case is the DRC.
The UN Security Council has passed several resolutions in the past 15 years relating to women and armed conflict.[97] Specifically, with regard to sexual and reproductive health rights in conflict settings, the Security Council has urged “United Nations entities and donors to provide non-discriminatory and comprehensive health services, including sexual and reproductive health” to survivors of sexual violence.[98]
Obligation to ensure effective documentation, accountability, and justice
States also have an obligation to provide victims of human rights violations, including specifically sexual violence, with an effective remedy in satisfaction of their rights to truth, justice, and reparation[99]. This obligation includes ensuring effective prosecution, punishment, and remedy for sexual violence committed by both state and non-state actors.[100] Concerning documentation and accountability for conflict-related sexual violence, states parties are obligated to include “training and the adoption, implementation and monitoring of legal provisions, administrative regulations and codes of conduct, and for investigating, prosecuting and applying appropriate legal or disciplinary sanctions, as well as providing reparation, in all cases of gender-based violence against women, including those constituting international crimes.”[101] Where existing national mechanisms lack the capacity to undertake independent impartial investigations and prosecutions, the international community should act to promote justice with input from affected local communities. The CEDAW Committee has stated that states must safeguard refugees and IDPs from sexual and gender-based violence, including child and forced marriage, provide them with immediate access to medical services, and create accountability mechanisms for sexual and gender-based violence in all displacement settings.[102]
The CEDAW Committee establishes that states parties’ measures to prevent sexual violence should “provide mandatory, recurrent and effective capacity-building, education and training for members of the judiciary, lawyers and law enforcement officers, including forensic medical personnel, legislators and health-care professionals.”[103] Further, the Committee calls on states parties to address conflict-related gender-based violence by adopting gender-sensitive investigative protocols, and taking steps to “develop and disseminate standard operating procedures and referral pathways to link security actors with clinicians on gender-based violence, including one-stop shops offering medical, legal and psychosocial services for sexual violence survivors, multipurpose community centers that link immediate assistance to economic and social empowerment and reintegration, and mobile clinic.”[104]
National Legal Context
The DRC national law also prohibits sexual violence and commits to accountability and justice for survivors. For example, the revised Constitution of 2011 commits to the elimination of sexual violence (Article 15).[105] This provision establishes the fight against sexual violence as a cross-cutting matter for the entire administration. Paragraph 2 establishes sexual violence as a serious crime if it has a specific intent.[106]
Further, Congolese legislation defines sexual violence as a serious crime which, in some instances, may constitute a war crime, a crime against humanity, and/or a crime of genocide[107]. In addition, the law commits to the provision of appropriate protection measures for victims and witnesses, including reparation and support mechanisms.[108] Under the penal code, sexual violence is a crime and punishable by 5 to 20 years imprisonment.[109] To strengthen the protection of children, it adopted a law on child protection in 2009. The DRC also specifically prohibits sexual offenses against children. Under the code of criminal procedure, the DRC government also commits to ensure timely adjudication, victims’ protection during the proceedings through closed sessions, and other supportive measures. [110]
In 2013, the Law on the Organization and Jurisdiction of the Judiciary was discussed, which, among other things, gives jurisdiction to the civil courts to try crimes against peace and security, bringing these offences before courts that are likely to offer more than guarantee a fair trial[111]. But also, to allow for better implementation of the Rome Statute, three harmonization laws were adopted in 2015 to amend and supplement the Military Criminal Code (15/023), the Criminal Code (15/022) and the Code of Criminal Procedure (15/024)[112].
Moreover, in 2020, the DRC revised and validated the National Strategy to Combat Gender-Based Violence and the Action Plan to Combat Gender-Based Violence in 2020, expanding the definition of gender-based violence to include domestic violence and gender-based violence in humanitarian contexts.[113] The revised national strategy is the reference framework for all actions related to prevention, victim care, and the fight against impunity for perpetrators of gender-based violence. It includes 124 activities to be carried out over five years, structured around seven main components, such as gender-based violence prevention, women’s empowerment, education, security and protection, justice, and data collection for monitoring and evaluation of interventions. While the action plan that accompanies this strategy for the period 2021-2025 aims to concretely implement the activities identified in the strategy. This action plan includes specific measures to improve holistic care for victims, strengthen justice mechanisms, and promote collaboration between different actors, including civil society organizations, government agencies, and international partners. These initiatives aim not only to reduce gender-based violence but also to provide adequate support to survivors and strengthen protection systems to prevent such violence in the future.
The DRC adopted Law No. 22/065 in 2022 which establishes the fundamental principles relating to the protection and reparation of victims of conflict-related sexual violence and victims of crimes against the peace and security of humanity[114]. This law is a major step forward in enshrining the rights of victims of serious crimes, fighting impunity and supporting them, including victims of conflict-related sexual violence. It has the merit of clarifying the concept of victim, adding administrative reparations alongside judicial reparations, setting up a Fund for the Benefit of Victims (FONAREV), among others. However, this measure has not yet resulted in reparations for many survivors.[115]
Conclusions and Recommendations
The findings of this report are a clarion call to the government of the DRC, other parties to the conflict, and regional and international actors to take urgent action to halt sexual violence as a tactic of war and to increase security and guarantee access to food and cooking fuel in IDP camps to prevent such violence. As funding for humanitarian aid and political will to negotiate diplomatic solutions are channeled to other crises, clinicians on the frontlines in the DRC report seeing “a massive influx” of survivors who have faced repeated acts of sexual violence during attacks and while displaced, including multiple perpetrator rape and rape with foreign objects. This violence has led to serious physical and psychological impacts, including sexually transmitted infections, unwanted pregnancy, incontinence, isolation, and post-traumatic stress disorder in addition to other long-term psychological harm. Yet, survivors also face significant barriers in accessing the health care they require to heal, as well as the materials and support necessary to have the evidence necessary to pursue accountability documented. Across North and South Kivu, clinicians have underscored the critical need for materials and training to support survivors’ healing and access to justice, including post-rape care, forensic documentation of sexual violence, and comprehensive health care for survivors including mental health and sexual and reproductive health care.
The sexual violence and resulting suffering experienced by civilians in eastern Congo indicate widespread violations of international law that merit monitoring and investigation. Stemming this crisis requires coordinated action by local, national, regional, and international actors. In particular, as MONUSCO continues to draw down its presence in eastern DRC, efforts must be redoubled to ensure that civilians do not face increased sexual violence and that survivors can pursue accountability and justice. Given these findings, PHR makes the following recommendations:
All parties to the conflict:
- Fully comply with IHL and IHRL in all aspects of operations throughout the conflict.
- Ensure that local armed forces and police forces, as well as various armed groups involved in the hostilities, do not engage in sexual violence, including by issuing clear directives prohibiting such violence, investigating and removing from service known perpetrators, and referring the perpetrators of these crimes to the appropriate courts to combat impunity.
- Implement the priority actions contained in regional diplomatic efforts, including the Luanda Process and the EAC-led Nairobi Process with a view to promote de-escalation and create the conditions for lasting peace in DRC, the repatriation of all foreign armed groups and foreigners, and compliance by local armed groups with the Disarmament, Demobilization, Community Recovery and Stabilization programme.[116]
The government of DRC:
- Take all measures to prevent sexual violence and establish conditions to enable IDPs to return to their living environments, including multisectoral coordinated care for survivors, emergency humanitarian aid and community recovery.
- Immediately improve access to food and cooking fuel inside of camps to prevent sexual violence against IDPs that occurs outside of the camps.
- Strengthen security in and around routes where displaced populations are fleeing and within the IDP camps to prevent sexual violence.
- Investigate, remove from service, and prosecute actors responsible for violations of IHL and IHRL including Congolese military and political figures, through the judicial services of the DRC.
- Ensure survivors’ access to justice and reparation for conflict-related sexual violence, including by:
- Supporting survivors who wish to report conflict-related sexual violence,
- Carry out geographic mapping of where violations have occurred to ensure coherent, effective, and efficient holistic response,
- Prioritize the development of a policy for the National Fund for the Reparation of Victims to make the identification of survivors who are eligible for reparations more effective and secure, including the digitalization of medicolegal documentation, and
- Building upon the national consultations held throughout the country, the DRC should adopt a binding legal text to support the implementation of transitional justice mechanisms which have thus far remained inoperative in their entirety
- Ensure accessible, available, acceptable, and quality health care for survivors of sexual violence, including post-rape care and prophylaxis, sexual and reproductive health care including stigma-free abortion care, mental health care, and child- and adolescent-friendly care.
- Take all measures to cooperate with regional and international legislative bodies to seek accountability and justice for human rights violations.
United Nations and members of the international diplomatic community:
- Regional leaders should exert influence on all states involved in the conflict to promote peace and support a robust African Union led peace support operation, should a ceasefire be negotiated.
Support efforts to ensure adherence with international humanitarian, human rights, and criminal law, including by exercising diplomatic pressure on all parties to de-escalate tensions, cease engagement in conflict-related sexual violence, and pursue diplomatic solutions.
- As committed by DRC in the June 2024 Security Council session,[117] refrain from authorizing the withdrawal of MONUSCO in North Kivu until progress is made to de-escalate the fighting and instability and when violence has come down meaningfully.
- Ensure robust monitoring of the situation in South Kivu where MONUSCO withdrawal has occurred, including rates of conflict-related sexual violence in border areas between North and South Kivu.
- Mobilize additional resources urgently to bolster the work of UN agencies, as well as non-governmental development, humanitarian, and peace organizations which support state services in their sovereign missions, funds, and programs in preparation for MONUSCO’s departure.
- Fully fund the 2024 DRC Humanitarian Response Plan, including to prevent sexual violence by strengthening provision of basic necessities (food, cooking fuel, and others) in IDP camps and by supporting survivors’ healing and access to justice through materials and training for post-rape care, forensic documentation of sexual violence, and comprehensive health care for survivors including mental health and sexual and reproductive health care.
- Increase international human rights cooperation and support to the government of DRC to promote stronger documentation and evidence-gathering of grave human rights abuses, with a special focus on conflict-related sexual violence and medicolegal documentation and care; to take measures to address risk factors for sexual violence such as lack of food and cooking fuel; and to ensure survivors’ access to reparations and multisectoral coordinated care as guaranteed in national law.
International Criminal Court (ICC) Office of the Prosecutor (OTP):
- In line with the ICC OTP memorandum of understanding with the DRC, the OTP should work with the government to:
- Continue to support efforts for accountability for past acts of conflict-related sexual violence to send a clear message that such violations will not be tolerated
- Provide support to the DRC government not only for forensic documentation relating to mass graves but also for ongoing cases of conflict-related sexual violence
- Investigate and prosecute perpetrators responsible for conflict-related sexual violence in violation of international law and ensure justice for survivors.
Acknowledgements
This report was researched and co-written by a team of Democratic Republic of the Congo (DRC) and United States-based PHR staff experts, with expertise on conflict-related sexual violence, public health, international human rights law, and research methodologies, including Thomas McHale, SM, PHR director of public health and Payal Shah, JD, director of legal, advocacy, and research, and additional co-authors who remain anonymous due to the severe and ongoing security risks in the eastern DRC.
PHR staff who contributed to the review of the report are: Saman Zia-Zarifi, JD, LLM, executive director; Karen Naimer, JD, LLM, MA, director of programs; Michele Heisler, MD, MPA, medical director; Payal Shah, JD, director of research, legal and advocacy; and Michael Payne, deputy director of advocacy; and Christian DeVos, JD, PhD, former director of research and investigations.
External review was provided by Ranit Mishori, MD, MHS, MSc, FAAFP, member of PHR advisory council; Adam Richards, MD, PhD, MPH, PHR board member and senior technical advisor at Community Partners International and Patrick Bigabwa, gynecologist in Panzi Hospital.
The research team would like to recognize the dedication and resilience of health care workers in the Democratic Republic of the Congo who have provided care and support for thousands of survivors of conflict-related sexual violence and whose experiences and stories are reflected in this report.
Citations and Endnotes
[1] “Why Congo’s M23 Crisis Lingers On,” Global Observatory, May 30, 2023, https://theglobalobservatory.org/2023/05/why-congos-m23-crisis-lingers-on/.
[2] “UN Peacekeepers Begin Withdrawal from DRC.” Voice of America, September 3, 2024,
https://www.voaafrica.com/a/un-peacekeepers-begin-withdrawal-from-drc/7505753.html; “Military Muscle Rather Than Mediation Prevails in DRC,” Institute for Security Studies, September 1, 2024, https://issafrica.org/iss-today/military-muscle-rather-than-mediation-prevails-in-drc.
[3] “Implementation of the Peace, Security and Cooperation Framework for the Democratic Republic of the Congo and the Region,” United Nations Security Council, April, 1, 2024, https://documents.un.org/doc/undoc/gen/n24/082/53/pdf/n2408253.pdf.
[4] “Attacks Against Healthcare in the Democratic Republic of the Congo,” International Rescue Committee, April 2024, https://www.rescue.org/sites/default/files/2024-04/ERSP%20UCB%20RIAH%20IRC%20-%20ATTACKS%20AGAINST%20HEALTHCARE%20DRC.pdf.
[5] “WHO Director-General declares mpox outbreak a public health emergency of international concern,” WHO, August 14, 2024, https://www.who.int/news/item/14-08-2024-who-director-general-declares-mpox-outbreak-a-public-health-emergency-of-international-concern.
[6] “Democratic Republic of the Congo,” OCHA, https://www.unocha.org/democratic-republic-congo
[7] Kambere Kavulikirwa, Olivier, “Intersecting Realities: Exploring the Nexus between Armed Conflicts in Eastern Democratic Republic of the Congo and Global Health,” Science Direct, https://doi.org/10.1016/j.onehlt.2024.100849.
[8] Council on Foreign Relations, “Violence in the Democratic Republic of Congo,” Global Conflict Tracker, Updated June 20, 2024, https://www.cfr.org/global-conflict-tracker/conflict/violence-democratic-republic-congo.
[9] Council on Foreign Relations, “Violence in the Democratic Republic of Congo,” Global Conflict Tracker, Updated June 20, 2024, https://www.cfr.org/global-conflict-tracker/conflict/violence-democratic-republic-congo.
[10] Council on Foreign Relations, “Violence in the Democratic Republic of Congo,” Global Conflict Tracker, Updated June 20, 2024, https://www.cfr.org/global-conflict-tracker/conflict/violence-democratic-republic-congo.
[11] Michaud, Catherine M., and Christopher J.L. Murray, “Resources for Health Research and Development in 2001: A Global Analysis.” The Lancet 368, no. 9534 (2006): 1077-1087, https://doi.org/10.1016/S0140-6736(06)67923-3; Simms, Chris, “Africa Needs the G8 to Do Better,” BMJ 336, no. 7638 (2008): 235, https://doi.org/10.1136/bmj.39458.591806.59.
[12] United States Holocaust Memorial Museum, “Democratic Republic of the Congo: 1996-Present,” Confront Genocide, https://www.ushmm.org/genocide-prevention/countries/democratic-republic-of-the-congo/1996-present.
[13] “Health Sector in DRC Crumbles Amidst Conflict, Negatively Impacting Survivors of Sexual Assault,” CARE , https://www.care.org/news-and-stories/press-releases/health-sector-in-drc-crumbles-amidst-conflict-negatively-impacting-survivors-of-sexual-assault/; Council on Foreign Relations, “Violence in the Democratic Republic of Congo,” Global Conflict Tracker, https://www.cfr.org/global-conflict-tracker/conflict/violence-democratic-republic-congo; Council on Foreign Relations. “DRC-Rwanda Talks Underway, but Lasting Peace Remains Elusive,” Africa in Transition (blog), https://www.cfr.org/blog/drc-rwanda-talks-underway-lasting-peace-remains-elusive; “The Nairobi Process,” East African Community, Accessed September 4, 2024, https://www.eac.int/nairobiprocess; “In Hindsight: The Escalating Conflict in Eastern DRC and UN Support of Regional Forces,” Security Council Report, April 2024, https://www.securitycouncilreport.org/monthly-forecast/2024-04/in-hindsight-the-escalating-conflict-in-eastern-drc-and-un-support-of-regional-forces.php; “Bold African Union Role Needed to Stabilise East DRC,” ISS Today, https://issafrica.org/iss-today/bold-african-union-role-needed-to-stabilise-east-drc; “Welcoming the Ceasefire in Eastern Democratic Republic of the Congo,” U.S. Department of State, https://www.state.gov/welcoming-the-ceasefire-in-eastern-democratic-republic-of-the-congo/.
[14] “Congo Peace Means a Halt to Brutal Illegal Mining,” United States Institute of Peace, published March 7, 2024, https://www.usip.org/publications/2024/03/congo-peace-means-halt-brutal-illegal-mining; “Blood Minerals: What Are the Hidden Costs of the EU-Rwanda Supply Deal?” Al Jazeera, published May 2, 2024, https://www.aljazeera.com/features/2024/5/2/blood-minerals-what-are-the-hidden-costs-of-the-eu-rwanda-supply-deal; United Nations Security Council. “Report of the Secretary-General on the Situation in the Democratic Republic of the Congo,” S/2024/432, June 4, 2024, https://n2411880.pdf (un.org); “Democratic Republic of the Congo (report),” Human Rights Watch, March 2001. https://www.hrw.org/reports/2001/drc/drc0301-03.htm; “Burundi,” Impact, https://impacttransform.org/en/countries/burundi/
[15] “Report of the Secretary-General on the Situation in the Democratic Republic of the Congo,” United Nations Security Council, S/2024/432, June 4, 2024, https://documents.un.org/doc/undoc/gen/n24/118/80/pdf/n2411880.pdf.
[16] “DR Congo: Army Units Aided Abusive Armed Groups,” Human Rights Watch, October 18, 2022, https://www.hrw.org/news/2022/10/18/dr-congo-army-units-aided-abusive-armed-groups.
[17] “DRC: Women Rebels Fight Back Against M23,” Al Jazeera, August 14, 2024, https://www.aljazeera.com/features/2024/8/14/drc-congo-women-rebels-m23; “In Eastern Congo, The Regional War is Already Here,” International Crisis Group, https://www.crisisgroup.org/africa/great-lakes/democratic-republic-congo/dans-lest-du-congo-la-guerre-regionale-est-deja-la; “Military Muscle Rather Than Mediation Prevails in DRC,” Institute for Security Studies, Accessed September 4, 2024, https://issafrica.org/iss-today/military-muscle-rather-than-mediation-prevails-in-drc.
Report of the Secretary-General on the Situation in the Democratic Republic of the Congo, S/2024/432, United Nations Security Council, June 4, 2024, https://documents.un.org/doc/undoc/gen/n24/118/80/pdf/n2411880.pdf.
[18] “In Eastern Congo, The Regional War is Already Here,” International Crisis Group International Crisis Group, Published July 16, 2024, https://www.crisisgroup.org/africa/great-lakes/democratic-republic-congo/dans-lest-du-congo-la-guerre-regionale-est-deja-la.
[19] “UN Peacekeepers Begin Withdrawal from DRC,” Voice of America. September 3, 2024, https://www.voaafrica.com/a/un-peacekeepers-begin-withdrawal-from-drc/7505753.html.
[20] “Military Muscle Rather Than Mediation Prevails in DRC,” Institute for Security Studies, September 1, 2024, https://issafrica.org/iss-today/military-muscle-rather-than-mediation-prevails-in-drc.
[21] Kumar, Rajesh, Sandeep Sharma, and Arun Gupta, “Advances in Molecular Diagnostics for Emerging Infectious Diseases,” Scientific Reports 14, no. 1 (2024): 65412, https://doi.org/10.1038/s41598-024-65412-7.
[22] Luma, Hubert, et al. “A Comprehensive Review of the Impact of COVID-19 on Health Systems and Health Care Workers in Sub-Saharan Africa,” International Journal of Environmental Research and Public Health 17, no. 21 (2020): 7597022. https://doi.org/10.3390/ijerph17217594; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7597022/;
“Health Systems Strengthening: WHO’s Approach to Health System Strengthening,” World Health Organization, 2016. https://iris.who.int/bitstream/handle/10665/250330/9789241511407-?sequence=1.
[23] “Attacks Against Healthcare in the Democratic Republic of the Congo,” International Rescue Committee, April 2024, https://www.rescue.org/sites/default/files/2024-04/ERSP%20UCB%20RIAH%20IRC%20-%20ATTACKS%20AGAINST%20HEALTHCARE%20DRC.pdf.
[24] “Attacks Against Healthcare in the Democratic Republic of the Congo,” International Rescue Committee, April 2024, https://www.rescue.org/sites/default/files/2024-04/ERSP%20UCB%20RIAH%20IRC%20-%20ATTACKS%20AGAINST%20HEALTHCARE%20DRC.pdf.
[25] “Disease Outbreak News: Democratic Republic of the Congo,” World Health Organization, October 25, 2023, https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON493; “Disease Outbreak News: Democratic Republic of the Congo,” World Health Organization, August 10, 2023. https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON441; “Yellow Fever – West and Central Africa,” World Health Organization, https://www.who.int/emergencies/disease-outbreak-news/item/yellow-fever—west-and-central-africa.
[26] “UNICEF Calls for Urgent Action to Respond to Alarming Levels of Increasing Sexual Violence,” UNICEF Press Release. September 3, 2024, https://www.unicef.org/press-releases/unicef-calls-urgent-action-respond-alarming-levels-increasing-sexual-violence-0#:~:text=Reports%20of%20gender%2Dbased%20violence,2022%20in%20North%20Kivu%20alone.
[27] “Essential Services Package for Women and Girls Subject to Violence: Module 1,” United Nations Population Fund (UNFPA), https://www.unfpa.org/resources/essential-services-package-women-and-girls-subject-violence-module-1#:~:text=The%20Essential%20Services%20Package%20is,services%2C%20police%20and%20justice%20sectors.
[28] “Ensuring Women’s Protection Amid Rising Conflict in Eastern DRC, Refugees International,” https://www.refugeesinternational.org/reports-briefs/ensuring-womens-protection-amid-rising-conflict-in-eastern-drc/.
[29] “Gender-Based Violence Cases Surge in Conflict Zones, UN Reports,” United Nations News, July 25, 2024, https://news.un.org/en/story/2024/07/1151846#:~:text=Gender%2Dbased%20violence-,Ms.,increasing%20by%2040%20per%20cent.
[30] “Care in the Midst of Conflict: Heal Africa in Eastern Democratic Republic of the Congo,” Physicians for Human Rights, Accessed at https://phr.org/our-work/resources/care-in-the-midst-of-conflict-heal-africa-in-eastern-democratic-republic-of-the-congo/.
[31] Baker, Sarah, et al., “Addressing the Health Needs of Conflict-Affected Populations: Evidence from Eastern Democratic Republic of the Congo,” BMJ Global Health 6, no. 10 (2024): e006631. https://doi.org/10.1136/bmjgh-2024-006631; “Ensuring Women’s Protection Amid Rising Conflict in Eastern DRC,” Refugees International, https://www.refugeesinternational.org/reports-briefs/ensuring-womens-protection-amid-rising-conflict-in-eastern-drc/.
[32] “Ensuring Women’s Protection Amid Rising Conflict in Eastern DRC,” Refugees International, Published April 2024, https://www.refugeesinternational.org/reports-briefs/ensuring-womens-protection-amid-rising-conflict-in-eastern-drc/.
[33] “Implementation of the Peace, Security and Cooperation Framework for the Democratic Republic of the Congo and the Region,” United Nations Security Council, April, 1, 2024, https://documents.un.org/doc/undoc/gen/n24/082/53/pdf/n2408253.pdf.
[34] “Democratic Republic of the Congo,” OCHA, accessed 5 April, 2024, https://www.unocha.org/democratic-republiccongo; “Humanitarian Response Plan Democratic Republic of the Congo 2023,” OCHA Financial Tracking Service, https://fts.unocha.org/plans/1113/summary.
[35] “Why Sexual Violence is Rising in Goma’s Displacement Camps,” Doctors Without Borders, September 18, 2023, https://www.doctorswithoutborders.org/latest/why-sexual-violence-rise-gomas-displacement-camps.
[36] “Support for Refugee Camps in North Kivu,” Panzi Foundation, https://panzifoundation.org/support-for-refugee-camps-in-north-kivu/.
[37] “Innovative E-Health Tool Scales in the Democratic Republic of Congo: Medicapt Launches HEAL Africa in Goma, DRC,” Relief Web, June 7, 2022, https://reliefweb.int/report/democratic-republic-congo/innovative-e-health-tool-scales-democratic-republic-congo-medicapt-launches-heal-africa-goma-drc.
[38] “Care in the Midst of Conflict: Heal Africa in Eastern Democratic Republic of the Congo,”Physicians for Human Rights, https://phr.org/our-work/resources/care-in-the-midst-of-conflict-heal-africa-in-eastern-democratic-republic-of-the-congo/
[39] “Visual Diary: Caring for Child Survivors of Sexual Violence in Eastern Democratic Republic of Congo,”
Physicians for Human Rights, July 19, 2024, https://phr.org/our-work/resources/visual-diary-caring-for-child-survivors-of-sexual-violence-in-eastern-drc/
[40] “Democratic Republic of the Congo 2023,”Amnesty International, https://www.amnesty.org/en/location/africa/east-africa-the-horn-and-great-lakes/democratic-republic-of-the-congo/report-democratic-republic-of-the-congo/.
[41] “Democratic Republic of the Congo 2023,”Amnesty International, https://www.amnesty.org/en/location/africa/east-africa-the-horn-and-great-lakes/democratic-republic-of-the-congo/report-democratic-republic-of-the-congo/; This was the DRCs second referral to the International Criminal Court – the first was made in 2004, https://www.amnesty.org/en/location/africa/east-africa-the-horn-and-great-lakes/democratic-republic-of-the-congo/report-democratic-republic-of-the-congo/; The International Criminal Court Office of the Prosecutor has now signed an Memorandum of Understanding with the DRC government to deliverable concrete deliverables through a framework of complementarity. domestic efforts through cooperation/complementarity, https://www.icc-cpi.int/news/prosecutor-international-criminal-court-karim-aa-khan-kc-concludes-his-first-visit-democratic.
[42] Democratic Republic of the Congo. Law n°22/065 in date of the 26th of December 2022 setting the foundational principles related to protection and reparations for victims of conflict-related and for victims of crimes against peace and security of humanity. Published December 26, 2022, https://leganet.cd.
[43] “Democratic Republic of the Congo,” Global Survivors Fund, https://www.globalsurvivorsfund.org/our-work/democratic-republic-of-the-congo/.
[44] “Minimal Norms for Prevention and Response to Gender-Based Violence in Emergency Situations,”United Nations Population Fund, November 2015, https://www.unfpa.org/sites/default/files/pub-pdf/16-092_Minimum_Standards_Report_FRENCH_proof.FINAL__1.pdf.
[45] “Eastern DRC at Breaking Point as Security, Humanitarian Crises Worsen,” Al Jazeera, March 29, 2024,
[46] Morse, Janice M, “The Significance of Saturation,” Qualitative Health Research 5, No. 2 (1995): 147-149. https://doi.org/10.1177/104973239500500201.
[47] “The Global Code of Conduct for Gathering and Using Information about Systematic and Conflict-Related Sexual Violence,” Murad Code, June 2020, https://www.muradcode.com/murad-code.
[48] “The Global Code of Conduct for Gathering and Using Information about Systematic and Conflict-Related Sexual Violence,” Murad Code, June 2020, https://www.muradcode.com/murad-code.
[49] “Sexual Violence, Trauma, and Neglect: Observations of Health Care Providers Treating Rohingya Survivors in Refugee Camps in Bangladesh,” Physicians for Human Rights, October 22, 2020, https://phr.org/our-work/resources/sexual-violence-trauma-and-neglect-observations-of-health-care-providers-treating-rohingya-survivors-in-refugee-camps-in-bangladesh/?utm_term=hero.
[50] Dedoose Version 9.2.12, cloud application for managing, analyzing, and presenting qualitative and mixed method research data (2024). Los Angeles, CA: SocioCultural Research Consultants, LLC, www.dedoose.com.
[51] “What Is Survival Sex?”, Changing Lives, December 2023, https://www.changing-lives.org.uk/insights/what-is-survival-sex.
[52] “The Wazalendo Patriots at War in Eastern DRC,” Le Monde, December 19, 2023, https://www.lemonde.fr/en/international/article/2023/12/19/the-wazalendo-patriots-at-war-in-eastern-drc_6356363_4.html.
[53] Rohwerder, Briony, “The Impact of Conflict on Health Care Provision and Access in the Democratic Republic of the Congo,” Conflict and Health 15 (2021): Article 14, https://doi.org/10.1186/s13031-021-00414-0.
[54] “UN Suspends Some Peacekeepers in Congo, Denounces Sexual Abuse,” Reuters, October 12, 2023, https://www.reuters.com/world/africa/un-suspends-some-peacekeepers-congo-denounces-sexual-abuse-2023-10-12/.
[55] Physicians for Human Rights uses the definition used by the United Nations to define conflict related sexual violence as “rape, sexual slavery, forced prostitution, forced pregnancy, forced abortion, enforced sterilization, forced marriage and any other form of sexual violence of comparable gravity perpetrated against women, men, girls or boys that is directly or indirectly linked to a conflict. That link may be evident in the profile of the perpetrator, who is often affiliated with S/2019/280 2/35 19-04552 a State or non-State armed group, which includes terrorist entities; the profile of the victim, who is frequently an actual or perceived member of a political, ethnic or religious minority group or targeted on the basis of actual or perceived sexual orientation or gender identity; the climate of impunity, which is generally associated with State collapse, cross-border consequences such as displacement or trafficking, and/or violations of a ceasefire agreement. The term also encompasses trafficking in persons for the purpose of sexual violence or exploitation, when committed in situations of conflict.” S/2019/280
[56] The International Criminal Court Elements of Crimes defines rape as: “The perpetrator invaded the body of a person by conduct resulting in penetration, however slight, of any part of the body of the victim or of the perpetrator with a sexual organ, or of the anal or genital opening of the victim with any object or any other part of the body” and “the invasion was committed by force, or by threat of force or coercion, such as that caused by fear of violence, duress, detention, psychological oppression or abuse of power, against such person or another person, or by taking advantage of a coercive environment, or the invasion was committed against a person incapable of giving genuine consent.”
[57] A quote from a psychologist in the Goma health zone working with survivors of CRSV since 2021
[58] Rohwerder, Briony, “The Impact of Conflict on Health Care Provision and Access in the Democratic Republic of the Congo,” Conflict and Health 15 (2021): Article 14, https://doi.org/10.1186/s13031-021-00414-0.
[59] “UN Urges Action to Address Sexual Violence and Exploitation in Conflict Zones,” United Nations News, October 10, 2023, https://news.un.org/en/story/2023/10/1142247.
[60] “UN Suspends Some Peacekeepers in Congo, Denounces Sexual Abuse,” Reuters, October 12, 2023, https://www.reuters.com/world/africa/un-suspends-some-peacekeepers-congo-denounces-sexual-abuse-2023-10-12/.
[61] “Gender and Clean Cooking: A Summary of Key Issues,”Clean Cooking Alliance, July 2021, https://cleancooking.org/wp-content/uploads/2021/07/CCA-gender-sheet-ENGLISH.pdf.
[62] Mulumba, D. (2011), “The Gendered Politics of Firewood in Kiryandongo Refugee Settlement in Uganda,” African Geographical Review, 30(1), 33–46. https://doi.org/10.1080/19376812.2011.10539134
[63] “DRC: Alarming Numbers of Sexual Violence Victims in Camps Around Goma,” Médecins Sans Frontières, https://www.msf.org/drc-alarming-numbers-sexual-violence-victims-camps-around-goma.
[64] “Democratic Republic of the Congo,” United Nations Office for the Coordination of Humanitarian Affairs, https://www.unocha.org/democratic-republic-congo.
[65] “Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa (Maputo Protocol),” African Union, adopted July 11, 2003, entered into force November 25, 2005.
Law n° 18/035 in date of the 13th of December 2018 setting the foundational principals related to the organization of Public Health.
[66] “Gender Data: Democratic Republic of the Congo,”World Bank, https://genderdata.worldbank.org/en/economies/congo-dem-rep.
[67] “Beating the Odds: Resilience, Hope, and Safe Births with UNFPA’s Mobile Clinic in the Democratic Republic of the Congo,” United Nations Population Fund, https://www.unfpa.org/news/beating-odds-resilience-hope-and-safe-births-unfpa-mobile-clinic-democratic-republic-congo.
[68] “WFP Delivers Nutrition Assistance to People Affected by Conflict in Eastern DRC,” ReliefWeb, https://reliefweb.int/report/democratic-republic-congo/wfp-delivers-nutrition-assistance-people-cut-conflict-eastern-drc.
[69] Remadji Hoinathy, “Eastern DRC: Peace Processes Miss the Mark,” Institute for Security Studies, https://issafrica.org/iss-today/eastern-drc-peace-processes-miss-the-mark; East African Community (EAC). “The EAC-Led Nairobi Process on Restoration of Peace and Security in Eastern DRC,” East African Community https://www.eac.int/nairobiprocess.
[70] “UN Warns of Escalating Humanitarian Crisis in Eastern DRC as Conflict Intensifies,” United Nations News, July 4, 2024. https://news.un.org/en/story/2024/07/1151701; “Democratic Republic of the Congo,” UNOCHA, 2024, https://www.unocha.org/democratic-republic-congo.
[71] Fourth Geneva Convention, article 27 (2). Article 76 of Protocol I extend this protection of protected persons to all women. Protocol I, article 76; Protocol II, article 4 (2) (a), (e), and (f).
[72] Statute of the International Criminal Court (1998), articles 7(1)(g); 8(2)(b)(xxii); 8(2)(e)(vi)
[73] United Nations General Assembly Rape as a grave, systematic and widespread human rights violation, a crime and a manifestation of gender-based violence against women and girls, and its prevention G21/089/99, https://documents.un.org/doc/undoc/gen/g21/089/99/pdf/g2108999.pdf; Office of the High Commissioner for Human Rights. General Comment No. 30 on Women in Conflict Prevention, Conflict, and Post-Conflict Situations. CEDAW/C/GC/30. https://www.ohchr.org/sites/default/files/Documents/HRBodies/CEDAW/GComments/CEDAW.C.CG.30.pdf.
[74] Article 3 common to the Geneva Conventions (CA3); ICRC, Commentary on GCI, 2016, CA3, paras. 696, 699, 701.
[75] Geneva Conventions Rule 158 Prosecution of War Crimes Rule 158. States must investigate war crimes allegedly committed by their nationals or armed forces, or on their territory, and, if appropriate, prosecute the suspects. They must also investigate other war crimes over which they have jurisdiction and, if appropriate, prosecute the suspects.
[76] “Command Responsibility and Failure to Act,” International Committee of the Red Cross, April 2014, https://www.icrc.org/sites/default/files/external/doc/en/assets/files/2014/command-responsibility-icrc-eng.pdf.
[77] “Draft Articles on Responsibility of States for Internationally Wrongful Acts, with Commentaries, International Law Commission, October 18, 2013, https://www.ohchr.org/sites/default/files/Documents/HRBodies/CEDAW/GComments/CEDAW.C.CG.30.pdf.
[78] United Nations General Assembly. “Convention on the Elimination of All Forms of Discrimination against Women (A/RES/34/180) Adopted 18 December 1979; Committee on the Elimination of Discrimination against Women; Rome Statute of the International Criminal Court Done at Rome on 17 July 1998, in force on 1 July 2002, United Nations, Treaty Series, vol. 2187, No. 38544, Depositary: Secretary-General of the United Nations, http://treaties.un.org; “Common Article 3 of the Geneva Conventions, 1949,”; Protocol Additional to the Geneva Conventions of 12 August 1949, and Relating to the Protection of Victims of International Armed Conflicts (Protocol 1); Protocol Additional to the Geneva Conventions of 12 August 1949, and Relating to the Protection of Victims of Non-International Armed Conflicts (Protocol II); Geneva Convention Relative to the Protection of Civilian Persons in Time of War of 12 August 1949;
[79] United Nations Declaration on the Elimination of Violence Against Women (1993); See, example, Declaration on the Elimination of Violence Against Women; CEDAW Committee, General Recommendation No. 35 on gender-based violence against women, updating general recommendation No. 19, para. 15, U.N. Doc. CEDAW/C/GC/35 (2017); https://documents.un.org/doc/undoc/gen/g21/089/99/pdf/g2108999.pdf para. 20.
[80] “Sexual and other forms of gender-based violence are prohibited as violations of autonomy, sex and gender discrimination, and as forms of torture,” See UN General Assembly, Convention on the Elimination of All Forms of Discrimination Against Women, December 18, 1979, United Nations, Treaty Series, vol. 1249, p. 13, http://www.un.org/womenwatch/daw/cedaw/cedaw.htm, Article 1; ICCPR, articles. 2 (1) and 26; UN General Assembly, Declaration on the Elimination of Violence against Women, article 4.
https://www.ohchr.org/en/countries/burundi, Status of Ratifications, CEDAW, 07 Feb 1992
[81] As clarified by the Committee on the Elimination of Discrimination against Women (CEDAW Committee) in General Recommendations 19, 30, and 35; “General Recommendation No. 19: Violence against Women,” Committee on the Elimination of Discrimination against Women, https://www.refworld.org/legal/resolution/cedaw/1992/en/96542; “General Recommendation No. 30 on Women in Conflict Prevention, Conflict, and Post-Conflict Situations,” Committee on the Elimination of Discrimination against Women,” https://www.refworld.org/legal/general/cedaw/2013/en/53711; “General Recommendation No. 35 (2017) on Gender-Based Violence against Women, Updating General Recommendation No. 19 (1992),” Committee on the Elimination of Discrimination against Women, https://www.ohchr.org/en/documents/general-comments-and-recommendations/general-recommendation-no-35-2017-gender-based.
[82] United Nations General Assembly, supra note 7
[83] Committee on the Elimination of Discrimination against Women (CEDAW Committee). General Recommendation No. 35 on Gender-Based Violence Against Women, Updating General Recommendation No. 19. CEDAW/C/GC/35, para. 24(b). https://www.ohchr.org/sites/default/files/Documents/HRBodies/CEDAW/GComments/CEDAW.C.CG.35.pdf.
[84] “Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa. Article 11(2),” African Union, 2003, https://au.int/en/treaties/protocol-african-charter-human-and-peoples-rights-rights-women-africa.
[85] “Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa. Article 11(3),” African Union, 2003, https://au.int/en/treaties/protocol-african-charter-human-and-peoples-rights-rights-women-africa.
[86] “Guiding Principles on Internal Displacement, second edition, OCHA/IDP/2004/01, New York,” United Nations, 2004, https://www.unhcr.org/protection/idps/43ce1cff2/guiding-principles-internal-displacement.html. In 1998 the UN Commission on Human Rights adopted a resolution taking note of the Guiding Principles on Internal Displacement, which are not legally binding but contain numerous rules that are part of existing international human rights law (IHRL) and IHL. Furthermore, the Guiding Principles have enjoyed wide support from the international community, and many states have incorporated them into their domestic legal systems.
[87] “African Union Convention for the Protection and Assistance of Internally Displaced Persons in Africa (Kampala Convention),” African Union, Adopted October 23, 2009. Entered into force December 6, 2012.
[88] Geneva Convention (IV) Relative to the Protection of Civilian Persons in Time of War, Articles 3, 4, and 27, International Committee of the Red Cross, August 12, 1949, https://ihl-databases.icrc.org/en/ihl-treaties/geneva-convention-iv; Additional Protocol I to the Geneva Conventions of 12 August 1949, and Relating to the Protection of Victims of International Armed Conflicts. Articles 51 and 75, International Committee of the Red Cross, June 8, 1977, Accessed September 4, 2024. https://ihl-databases.icrc.org/en/ihl-treaties/additional-protocol-i; Additional Protocol II to the Geneva Conventions of 12 August 1949 and Relating to the Protection of Victims of Non-International Armed Conflicts. Articles 4 and 5, International Committee of the Red Cross, June 8, 1977, Accessed September 4, 2024, https://ihl-databases.icrc.org/en/ihl-treaties/additional-protocol-ii; Customary International Humanitarian Law. Rules 1 and 7, International Committee of the Red Cross, https://ihl-databases.icrc.org/en/customary-ihl/v1/rule1; https://ihl-databases.icrc.org/en/customary-ihl/v1/rule7.
[89] Additional Protocol II to the Geneva Conventions of 12 August 1949 and Relating to the Protection of Victims of Non-International Armed Conflicts. Articles 4 and 5, International Committee of the Red Cross, June 8, 1977. Accessed September 4, 2024. https://ihl-databases.icrc.org/en/ihl-treaties/additional-protocol-ii; Customary International Humanitarian Law. Rules 1 and 7, International Committee of the Red Cross, https://ihl-databases.icrc.org/en/customary-ihl/v1/rule1; Customary International Humanitarian Law, Rules 1, 7, 14, 15, and 22, International Committee of the Red Cross, https://ihl-databases.icrc.org/en/customary-ihl/v1/rule1; https://ihl-databases.icrc.org/en/customary-ihl/v1/rule7; https://ihl-databases.icrc.org/en/customary-ihl/v1/rule1; https://ihl-databases.icrc.org/en/customary-ihl/v1/rule7; https://ihl-databases.icrc.org/en/customary-ihl/v1/rule14; https://ihl-databases.icrc.org/en/customary-ihl/v1/rule15; https://ihl-databases.icrc.org/en/customary-ihl/v1/rule22.
[90] “Geneva Convention (IV) Relative to the Protection of Civilian Persons in Time of War, Articles 3, 4, and 27,” International Committee of the Red Cross, August 12, 1949, https://ihl-databases.icrc.org/en/ihl-treaties/geneva-convention-iv; “Additional Protocol I to the Geneva Conventions of 12 August 1949, and Relating to the Protection of Victims of International Armed Conflicts, Articles 51 and 75,” International Committee of the Red Cross, June 8, 1977, Accessed September 4, 2024, https://ihl-databases.icrc.org/en/ihl-treaties/additional-protocol-i; “Additional Protocol II to the Geneva Conventions of 12 August 1949, and Relating to the Protection of Victims of Non-International Armed Conflicts, Article 4,” International Committee of the Red Cross, June 8, 1977, Accessed September 4, 2024. https://ihl-databases.icrc.org/en/ihl-treaties/additional-protocol-ii; “Customary International Humanitarian Law, Rules 87, 89, and 93,” International Committee of the Red Cross, https://ihl-databases.icrc.org/en/customary-ihl/v1/rule87;
https://ihl-databases.icrc.org/en/customary-ihl/v1/rule89; https://ihl-databases.icrc.org/en/customary-ihl/v1/rule93;
[90] “Geneva Convention (IV) Relative to the Protection of Civilian Persons in Time of War, Article 49(3),” August 12, 1949, International Committee of the Red Cross, https://ihl-databases.icrc.org/en/ihl-treaties/geneva-convention-iv; “Geneva Conventions of 12 August 1949, Common Article III,” International Committee of the Red Cross, August 12, 1949, https://ihl-databases.icrc.org/en/ihl-treaties/geneva-convention-i-iv; “Additional Protocol II to the Geneva Conventions of 12 August 1949, and Relating to the Protection of Victims of Non-International Armed Conflicts, Article 17(1),” International Committee of the Red Cross, June 8, 1977, https://ihl-databases.icrc.org/en/ihl-treaties/additional-protocol-ii; “Customary International Humanitarian Law, Rule 131,” International Committee of the Red Cross, https://ihl-databases.icrc.org/en/customary-ihl/v1/rule131.
[92] General Recommendation No. 30 on Women in Conflict Prevention, Conflict and Post-Conflict Situations. Para. 57. October 18, 2013, https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/Download.aspx?symbolno=CEDAW%2fC%2fGC%2f30&Lang=en.
[93] Committee on the Elimination of Discrimination against Women. General Comment 30, paragraphs 50(c)-(d)
The CEDAW Committee has stated that the failure to provide services that only women require to meet their reproductive health needs is a form of discrimination and has emphasized that state obligations under the Convention “are non-derogable and continue to apply during conflict situations.” CEDAW Committee, General Recommendation No. 24: Article 12 of the Convention (Women and Health), paras. 17, 26, U.N. Doc. A/54/38/Rev. 1 (1999) [hereinafter CEDAW Committee, Gen. Recommendation No. 24]; CEDAW Committee, Concluding Observations: Central African Republic, para. 13, U.N. Doc. CEDAW/C/CAF/CO/1-5 (2014). See also CEDAW Committee, Gen. Recommendation No. 28, para. 11; CEDAW Committee, Gen. Recommendation No. 30. 4. For women and girls affected by conflict, the CEDAW Committee has called on state parties to [e]nsure that sexual and reproductive health care includes access to sexual and reproductive health and rights information; psychosocial support; family planning services, including emergency contraception; maternal health services, including antenatal care, skilled delivery services, prevention of vertical transmission and emergency obstetric care; safe abortion services; post-abortion care; prevention and treatment of HIV/AIDS and other sexually transmitted infections, including post-exposure prophylaxis; and care to treat injuries such as fistula arising from sexual violence, complications of delivery or other reproductive health complications, among others. CEDAW Committee, Gen. Recommendation No. 30, para. 52(c).
[94] See, e.g., William H. Boothby and Michael N. Schmitt, The Law of Targeting (Oxford: Oxford University Press, 2013), 233.
[95] See Fourth Geneva Convention, Articles 16–18, 21–23, 38, 50, 89, 91 and 127 (ibid., §§ 76–80); Additional Protocol I, Article 70(1) (adopted by consensus) (ibid., § 81) and Article 76(2) (adopted by consensus) (ibid., § 82).
[96] “Guiding Principles on Internal Displacement,” See principles 3 and 25 of UNOCHA, 1998, https://www.unhcr.org/43ce1cff2.pdf.
[97] UN Security Council Resolutions: Normative Frameworks, https://peacemaker.un.org/wps/normative-frameworks/un-security-council-resolutions.
[98] United Nations Security Council. Resolution 2106, para. 19. U.N. Doc. S/RES/2106. June 24, 2013, https://undocs.org/S/RES/2106(2013).
[99] “About Transitional Justice and Human Rights,”Office of the United Nations High Commissioner for Human Rights (OHCHR), https://www.ohchr.org/en/transitional-justice/about-transitional-justice-and-human-rights#:~:text=Transitional%20justice%20is%20rooted%20in,truth%2C%20justice%2C%20and%20reparation;
United Nations. Draft Articles on Responsibility of States for Internationally Wrongful Acts, with Commentaries. 2001, Accessed https://www.un.org/law/ilc/texts/state_responsibility/responsibility_articles.pdf; General Recommendation No. 35 on Gender-Based Violence against Women, Updating General Recommendation No. 19. Para. 2. November 14, 2017. https://documents.un.org/doc/undoc/gen/n17/231/54/pdf/n1723154.pdf.
[100] CEDAW Committee. General Recommendation No. 35 on Gender-Based Violence against Women, Updating General Recommendation No. 19. Para. 2, November 14, 2017. https://www.ohchr.org/en/documents/general-comment-or-recommendation/general-recommendation-no-35-gender-based-violence.
[101] CEDAW Committee, General Recommendation No. 35 on Gender-Based Violence against Women, Updating General Recommendation No. 19. Para. 23. November 14, 2017, Accessed September 4, 2024, https://www.ohchr.org/en/documents/general-comment-or-recommendation/general-recommendation-no-35-gender-based-violence.
[102] CEDAW Committee, General Recommendation No. 30 on Women in Conflict Prevention, Conflict and Post-Conflict Situations, Para. 57, October 18, 2013, https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/Download.aspx?symbolno=CEDAW%2fC%2fGC%2f30&Lang=en.
[103] CEDAW Committee, General Recommendation No. 35 on Gender-Based Violence against Women, Updating General Recommendation No. 19. Para. 30(e). November 14, 201, https://www.ohchr.org/en/documents/general-comment-or-recommendation/general-recommendation-no-35-gender-based-violence.
[104] CEDAW Committee. General Recommendation No. 30 on Women in Conflict Prevention, Conflict and Post-Conflict Situations. Para. 35(f). October 18, 2013. https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/Download.aspx?symbolno=CEDAW%2fC%2fGC%2f30&Lang=en.
[105] Congo (Democratic Republic of the) 2005 (rev. 2011) Article 15
[106] Congo (Democratic Republic of the) 2005 (rev. 2011)
[107] Congolese Penal Code Official Journal Special issue 30th of November 2004
Code of Criminal Procedure, 1959, Democratic Republic of the Congo, Decree in date of the 6th of August 1959
Congo (Democratic Republic of the) 2005 (rev. 2011)
[108] The Democratic Republic of Congo – Act No. 22/065 of 26 December 2022
[109] Congolese Penal Code Official Journal Special issue 30th of November 2004
Code of Criminal Procedure, 1959, Democratic Republic of the Congo, Decree in date of the 6th of August 1959
[110] Congolese Penal Code Official Journal Special issue 30th of November 2004
Code of Criminal Procedure, 1959, Democratic Republic of the Congo, Decree in date of the 6th of August 1959
“Democratic Republic of the Congo,” the U.S. Department of State, 2023,
[111] “Magistrates Discuss Dual Jurisdiction of Military and Civilian Courts for International Crimes in DRC,” International Center for Transitional Justice (ICTJ), October 9, 2015, https://www.ictj.org/news/drc-magistrates-discuss-dual-jurisdiction-military-civilian-courts-international-crimes.
[112] Law n° 06/018 in date of the 20th of July 2006 modifying and adding to the «sentence». Decree in date of the 30th of January 1940 regarding the Congolese Code of Criminal Procedure.
[112] Law n° 06/019 in date of the 20th of July 2006 modifying and adding to the «sentence». Decree in date of the 30th of January 1940 regarding the Congolese Code of Criminal Procedure.
Organic Law n°13/011-B in date of 11 April 2013, regarding the organization, functioning and competencies of jurisdictions of the legal Order.
[113] “DRC Takes a Step Towards Zero Tolerance Against Gender-Based Violence,” UN Women Africa, September 1, 2020, https://africa.unwomen.org/en/news-and-events/stories/2020/09/drc-takes-a-step-towards-zero-toleranceagainst-gender-basedviolence#:~:text=This%20revision%20aims%20to%20eliminate,of%20GBV%2C%20including%20domestic%20violence.
[114] Human Rights Committee
Information received from the Democratic Republic of the Congo on follow-up to the concluding observations on its fourth periodic report *[Date received: 4 September 2023]
[115] “Amnesty International Report 2022/23: The State of the World’s Human Rights,” Amnesty International, accessed April 5, 2024, https://www.amnesty.org/en/location/africa/east-africa-the-horn-and-great-lakes/democraticrepublic-of-the-congo/report-democratic-republic-of-the-congo/.
[116] “DRC: MONUSCO Supports New Demobilization Program for Ex-Combatants,” United Nations Peacekeeping, April 1, 2024, https://peacekeeping.un.org/en/drc-monusco-supports-new-demobilization-program-ex-combatants.
[117] “Military Group’s Expansion in Democratic Republic of Congo ‘Carries Very Real Risk of Provoking Wider Regional Conflict’, Mission Head Tells Security Council, Press Release: SC/15760,”United Nations, Meetings Coverage and Press Release, July 8, 2024, https://press.un.org/en/2024/sc15760.doc.htm.
Cover Photo: Women and children are at risk of experiencing sexual violence while searching for food or firewood outside of the Bulengo Internally Displaced Persons (IDP) camp near Goma, DRC in 2024. Photo: Alexis Huguet/AFP via Getty Images