
Executive Summary
In March 2011, the Arab Spring movement spread to Syria when civilians across the country began peacefully demonstrating against the government of President Bashar al-Assad. Although the Syrian government tried to signal to the international community that it was responding to the demands of peaceful demonstrators, in reality, it violently cracked down on peaceful protesters.[1] Security forces began brutally suppressing protests and detaining health care workers who treated injured protesters, effectively criminalizing health care. Most of the health care workers detained by the government were forcibly disappeared – they were never charged, and their fate remains unknown; some were released, and an unknown number have died in detention. Enforced disappearance is a crime with multiple victims: in addition to the physical and psychological suffering of the detainees, their families and community are all forced to live with mental anguish and uncertainty about their loved ones’ fate, without access to their remains for proper burial and memorial when they are deceased.
In this report, Physicians for Human Rights (PHR) examines patterns in the Syrian government’s forced disappearance, detention, and abuse of health care workers during the early years of the Syrian uprising. The findings are based on a new data set of 1,685 detentions that occurred in 2011 and 2012, which PHR compiled using data sets provided by the Open Society Justice Initiative, the Syrian Network for Human Rights, and the Violations Documentation Center. The PHR research team systematically reviewed the original data sets to standardize the format, create new variables using information from notes sections, and deduplicate repeated cases. In addition to several examples from previous PHR interviews with physicians detained for providing health care, this report includes a case study of a medical team that operated in Aleppo in 2012. Many of the team’s members were detained by the Syrian government and several were killed while in detention. This newly compiled data and PHR’s analysis illuminate the government’s massive violent crackdown on dissent and its persecution of health care workers who responded to the injured during the initial years of the Syrian crisis.
From the earliest days of the Syrian uprising, the Syrian government targeted health care workers with detention, abuse, and torture for providing medical assistance to those who opposed the regime.
The report reveals that a health care worker’s profession and the reason they were detained appear to have had a significant impact on the outcome of their detention. PHR’s analysis yielded two main findings: health care workers detained for providing medical care experienced worse outcomes than health care workers detained for their political activities, and among detained health care workers, physicians overall experienced better outcomes than non-physicians.
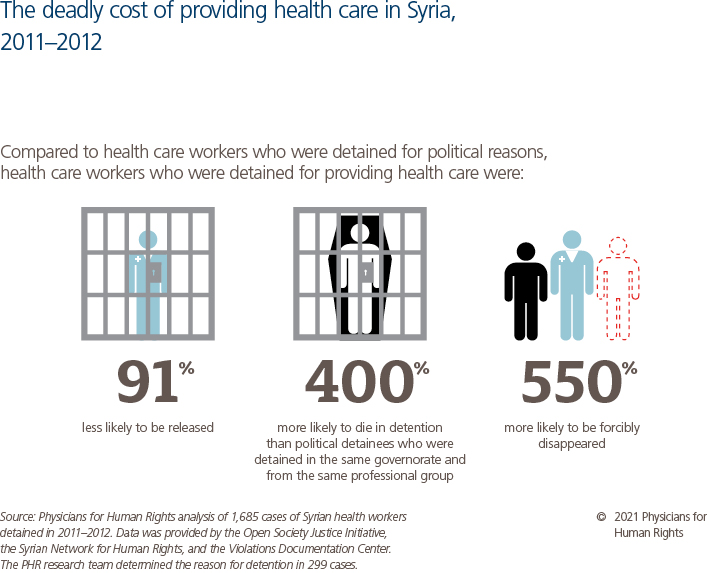
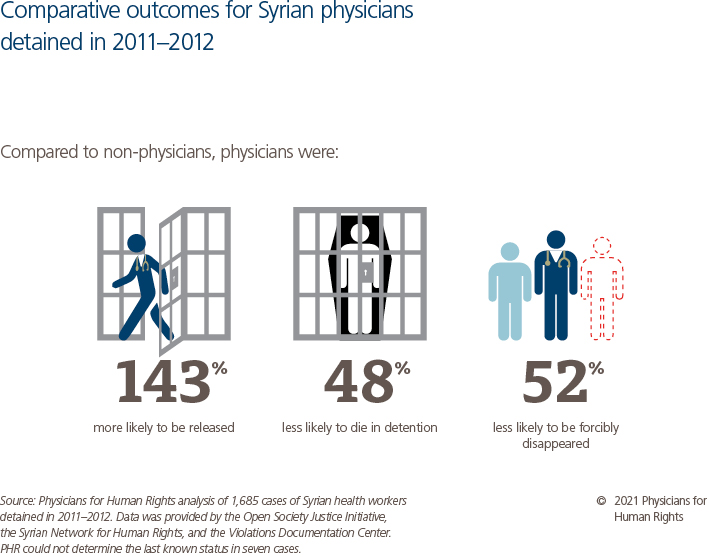
If the Syrian government detained a health care worker for providing medical care to an injured protester, the odds of release for that person were 91 percent lower and the odds of being forcibly disappeared were 550 percent higher compared to the fate of health care workers detained for political reasons. If two health care workers from similar professions were detained in the same place for different reasons, the data show that the one detained for providing health care would have 400 percent higher odds of dying in detention than the person detained for a political reason. Further, while most health care workers experienced poor outcomes, either dying or being forcibly disappeared, the odds that a physician would be released were 143 percent higher than for non-physicians. Physicians were also 52 percent less likely to be forcibly disappeared and 48 percent less likely to die in detention compared to non-physicians. There are many potential explanations for why and how these factors influenced detention outcomes, which this report explores.
Most of the health care workers detained by the government were forcibly disappeared – they were never charged, and their fate remains unknown; some were released, and an unknown number have died in detention.
PHR’s analysis shows that, from the earliest days of the Syrian uprising, the Syrian government targeted health care workers with detention, abuse, and torture for providing medical assistance to those who opposed the regime. The United Nations has estimated that the Syrian government arbitrarily detained or forcibly disappeared at least 100,000 people, among them thousands of health care workers, in contravention of domestic laws, human rights law, and international humanitarian law. As the Syrian conflict moves towards a potential phase of negotiation, it is imperative that the voices of the survivors and missing persons’ families be heard and that they be told the truth about their loved ones’ disappearance. In addition to the need for truth, Syrians deserve justice and accountability for the mass forced disappearance of opponents to the Syrian regime and those who provided care to the sick and wounded according to their ethical and moral duties.
In February 2021, a coalition of five Syrian organizations representing survivors, their families, and family members of the missing drafted a vision of its goals called the “Truth and Justice Charter.” In it, they have called for the United Nations to address the needs of survivors and their families. PHR urges the international community to heed their call, in order to lay the foundation for a future peace.
Key Recommendations:
To the Syrian Government and Affiliated Forces, and All Parties to the Conflict:
Immediately and unconditionally release all arbitrarily or unlawfully detained health care workers from official and unofficial detention sites.
To the UN Special Envoy for Syria:
Ensure that discussions of human rights and international humanitarian law violations, including arbitrary detention, torture, enforced disappearances, and attacks on health, are prominent within the political process.
To UN Member States:
Coordinate efforts and endorse the Truth and Justice Charter and ensure that survivor-led short- and long-term plans for peace and accountability are the main drivers of decision making.

Introduction
The Syrian conflict has been characterized by a systematic assault on health care facilities by the Syrian government and its Russian allies, with the intent of preventing non-government-controlled areas from receiving medical care. From the earliest days of the conflict, the government arrested, unlawfully detained, and forcibly disappeared health care workers, including nurses, doctors, and medical volunteers, among many others.[2]
Although the government does not acknowledge a forced disappearance, let alone provide information to the family of the disappeared, colleagues, communities, and family members have maintained records of the circumstances of their loved one’s disappearance. The United Nations (UN) estimates that at least 100,000 Syrian civilians have been forcibly disappeared in the past decade[3] and tens of thousands of Syrians have died in detention after being forcibly disappeared.[4] Health care workers make up an important subset of those forcibly disappeared because, in addition to depriving them of their liberty, the government deprives their communities of the health care they can provide.
This report addresses the detention of health care workers by the Syrian government in the early years of the Syrian uprising. Specifically, it examines outcomes among health care workers – including physicians, pharmacists, nurses, students, and others – who were detained by state security and intelligence forces for providing health care to protesters. The report analyzes 1,685 detentions of 1,644 health care workers (some were detained multiple times) that occurred between 2011 and 2012 and were recorded and maintained by civil society organizations. The records are specific to health care workers who were detained, forcibly disappeared, released, or died while in detention. Through a combination of research, interviews, and descriptive notes from data sets, the report also highlights the experiences of health care workers who were detained.
Any negotiated settlement to the conflict in Syria must address as a central element the issue of Syrians who have been disappeared. Without a clear and sustainable survivor-driven solution for the families of the missing, it is unlikely that any negotiations will result in lasting peace.
A coalition of the families of the Syrian missing has consolidated its demands in the “Truth and Justice Charter,”[5] which lays out policy priorities. Physicians for Human Rights (PHR) recognizes the need for information and closure among the families of the disappeared, including access to the remains of the deceased and the ability to settle legal affairs. It also acknowledges the long-term need for the Syrian government to be held accountable in justice processes for these gross human rights violations. This report will contribute to the discussion of the ongoing grave situation of the many health care workers and others who remain missing in Syria. PHR insists that any negotiated settlement to the conflict in Syria must address as a central element the issue of Syrians who have been disappeared. Without a clear and sustainable survivor-driven solution for the families of the missing, it is unlikely that any negotiations will result in lasting peace.

Background
In March 2011, peaceful protests calling for economic and political reforms broke out across Syria. Unarmed protesters were quickly met with violence and repression by the Syrian government’s security forces, including military units, government-backed militias, and intelligence agencies. As the protest movement grew across the country, the government responded with increasing force and began to systematically target health care workers and others suspected of treating injured protesters.[6] Syrian health care workers willing to treat protesters were unable to provide this care in government-controlled public health facilities without the risk of detention. Therefore, they developed a network of underground “field hospitals” to provide basic trauma care and surgery for civilians injured during protests.[7] These health care workers also created a referral system to help injured protesters avoid detection and arrest. Beginning in March 2011, it was common for state security agents to be present in public – and some private – health facilities, particularly after demonstrations. In all public hospitals, a 24/7 security unit tracked all admissions to emergency departments in order to arrest injured demonstrators and the health care workers treating them. In response, individual health care workers coordinated with private and charity-run health facilities – where security forces were less likely to be present – to facilitate safe access to health care for injured demonstrators. However, if security agents were present in the facility, or if the private hospital manager believed there was a high risk that a security agent would enter, he would usually refuse to accept the transfer.[8]
Syrian health care workers willing to treat protesters were unable to provide this care in government-controlled public health facilities without the risk of detention. Therefore, they developed a network of underground “field hospitals” to provide basic trauma care and surgery for civilians injured during protests.
In retaliation for this medical response that Syrian health care workers provided to the large number of injured protesters, the Syrian government began detaining hundreds of health care personnel working in and supporting the field hospitals and referral network. They were held in facilities where security officials subjected them to horrific conditions and abuses, including torture. Many died, and thousands simply disappeared into the system, their whereabouts unknown to this day. Those whose families had personal connections or wealth often learned of their whereabouts or gained their freedom only after paying hefty bribes.[9] As the country erupted into open conflict in 2012, the government began a coordinated campaign to destroy access to health care by systematically attacking health facilities and health care workers.[10] The Syrian government has long benefited from its political alliance with the Russian Federation, which has provided military support, including Russian airstrikes on medical facilities.[11]
Physicians for Human Rights (PHR) has documented the detention of health care workers in Syria throughout the conflict, in which multiple parties have committed human rights violations and war crimes, including enforced disappearances, torture, sieges, bombing of civilian infrastructure, and widespread and systematic attacks on hospitals and clinics. By December of 2011, the Office of the High Commissioner for Human Rights estimated that 4,000 Syrians had been killed in the context of the uprising. To date, however, the detention and disappearance of health care workers in the initial stages of the conflict, between 2011 and 2012, have not been rigorously examined.
A more detailed assessment of the use of Syria’s detention regime to persecute health care workers is critical to understanding the initial stages of the government’s systematic campaign to undermine access to health care. From March to December 2011, the Syrian government directly controlled most of the country, including all major cities and public health facilities. The government heightened its control of health facilities by increasing the state security and intelligence force presence in them. The military and civil police forces and the four intelligence agencies,[12] or mukhabarat, all monitored emergency room admissions and reported on or detained any patients with injuries that could have occurred at a protest.[13] Security forces also detained any health care provider who failed to report an injured protester prior to providing care. During this period, health care workers throughout Syria became increasingly vulnerable to state violence as Syrian security forces began systematically detaining medical personnel across the country.
The Syrian government detains health care workers because it alleges that the treatment and lifesaving care they provide to its opponents, whom they classify as “terrorists,” constitutes material support for terrorism.[14] Criminalizing health care in this way disregards the protection of care to the sick and wounded in international humanitarian law. Significantly, between March 2011 and July 2012, there was little to no armed opposition, hence no such “justification” for the detention of health care workers. Moreover, President Bashar al-Assad’s repeal of Syria’s emergency law in April 2011, which had for decades given the government the power to arbitrarily detain and arrest perceived opponents, was followed by legislation legalizing peaceful protests.[15] It was not until July 2012 that the government passed the counterterrorism law that codified its unjust practices to criminalize protests and the provision of humanitarian aid, among other activities.[16] In this context, the Syrian government’s actions during this critical first phase of the conflict, prior to the development of an armed opposition, illustrate a clear strategy to intentionally deprive its perceived opponents of access to health care as a means of punishment.
To document this harsh strategy in a sample of health care workers who were detained, PHR examined: 1) characteristics of a large data set of health care workers detained between January 2011 and December 2012; 2) characteristics and outcomes of their detention; and 3) associations between type of health care worker (professional background), reason for detention (medical vs. political), and the detainee’s last known status.
Methodology
The findings in this report are based on secondary analysis of a data set describing 1,685 detentions of Syrian health care workers from 2011 to 2012, in-depth interviews with four members of a medical team operating in Aleppo, and a desk review of open-source documentation of information sources used for creating the timeline and verifying accounts presented in the case study. Physicians for Human Rights’ (PHR) Ethics Review Board (ERB) provided guidance and approved this study based on regulations outlined in Title 45 CFR Part 46, which are used by academic institutional review boards in the United States. All PHR’s research and investigations involving human subjects are conducted in accordance with the Declaration of Helsinki 2000, a statement of ethical principles for medical research involving human subjects, including research on identifiable human material and data.
PHR Data Set
The report is primarily based on a data set containing 1,685 community-generated records of the detention of health care workers from January 2011 to December 2012. Groups of Syrian activists, including health care workers, students, lawyers, and journalists, worked with Local Coordination Committees in different governorates across the country to collect the original data.[17] Those who collected the information followed a system in which as many data points as possible were collected, including: name, profession, data of birth, location of residence, location of arrest or disappearance, and descriptive notes, including other additional information describing the detention event compiled by the activists and added to the database whenever possible. The descriptive notes varied in quality, consistent with the information available at the time the record was produced. The original data was then submitted to civil society organizations that served as central collection sites. The assembled data was subsequently shared with regional and international human rights organizations in order to establish a record of detentions over the last decade. PHR’s research team, composed of experts fluent in Arabic and English and knowledgeable about the Syrian context, compiled the PHR data set (“data set”) by merging, cleaning, and recoding three independent data sets provided to PHR by the Open Society Justice Initiative (OSJI), the Syrian Network for Human Rights (SNHR), and the Violations Documentation Center (VDC).[18]
Cleaning the Data
In order to merge the data sets, the PHR research team systematically reviewed the data and formatted it into a uniform structure across all three data sets. Team members then categorized qualitative data from the descriptive notes section into different variables, including the governorate in which the arbitrary arrest or disappearance occurred,[19] profession, and reason for detention. The professions of the detainees were grouped into six broad categories: physicians; holders of university-level health science degrees (dentists, pharmacists, and veterinarians); holders of institute-level health science degrees (nurses and technicians); health science students; non-health background; and unknown.[20]
To categorize the reason for a health care worker’s detention, the team systematically searched the descriptive notes about the detention event contained in each data set (where available) for keywords to distinguish between those health care workers detained for their political actions, such as attending a demonstration, and those detained for providing health care to people the government viewed as opponents. In 1,386 detention cases (82 percent), there was insufficient information to determine the reason for detention, so the field was left blank. Some individuals were officially detained, and many others were forcibly disappeared. Forcible disappearance is defined as the secret abduction or imprisonment of a person by a state or political organization, or by a third party with the authorization, support, or acquiescence of a state or political organization, followed by a refusal to acknowledge the person’s fate and whereabouts, with the intent of placing the victim outside the protection of the law.[21]
To distinguish between these two types of detainees, the team searched the notes for references to a legal proceeding. Detainees who received a court sentence or were reportedly held in civilian central prisons were categorized as “officially detained” instead of “forcibly disappeared.” Dates of detention, release, and death were standardized using the month-day-year format. The duration of detention was then calculated by subtracting the date of release or death from the date of detention.[22] Age at detention was calculated by subtracting date of detention from the date of birth.
Ranking and Merging the Sources
The research team ranked the quality of the three data sets according to their comprehensiveness and when they were last updated. The SNHR data set – the largest, most complete, and most recently updated of the three – was ranked highest, followed by the data sets VDC and OSJI provided, in that order. Inconsistencies between the data sets were resolved by deferring to the highest-ranked data set. In cases where entries in the VDC and OSJI data sets matched but differed from the SNHR data set, PHR used the data supported by the majority. When any data set recorded a detainee’s last known status as “released” or “died,” this status was used in place of “forcibly disappeared,” regardless of which data set provided the information. To avoid the duplication of cases, the team de-duplicated records from the merged data set in which the names were the same or substantially similar and matched in three of the following five variables: date of detention, date of release or death, governorate of detention, governorate of origin, and profession.
To obtain the total number of health care workers included in the data set, the team then reviewed all cases with matching names to determine whether the same person was detained multiple times. The team associated multiple detentions with a single person if the names matched, the dates of detention did not overlap, the last known status for every earlier detention was “released,” and there were no conflicting entries for age, gender, profession, or governorate of origin. The team accepted Damascus and Rural Damascus as the same governorate of origin only when reviewing these cases due to shifting administrative boundaries. The team also reviewed the notes sections of each case for any additional identifying information or references to other detentions.[23]
Quantitative Data Analyses
The process of merging, cleaning, and recategorizing the data was completed using Microsoft Excel.[24] The same software was also used to perform and document the de-duplication of cases. The research team then uploaded the PHR data set to Stata, where a Do File and a log were created to document steps in the data analysis.[25] First, all categorical variables were encoded to convert strings (data values that can include letters) into numeric variables. Date of detention and date of release were encoded in Stata and the duration of detention variable was created and calculated in days. String variables were then deleted, and encoded variables were labeled and sorted.
The research team also used Stata to clean the data set by changing the “last known status” for seven cases to “unknown” due to each case having a last known status of “forcibly disappeared” with dates indicating either release or death. Ages below 18 years (two cases) and negative durations of detention (15 cases) were replaced by missing values.
PHR researchers examined the relationships between characteristics of detainees, including their profession, reason for detention, and last known status using STATA. The team examined bivariate associations between detainees’ last known status and their province of detention, profession, and reason for detention in chi-square analyses using an alpha of .05 for statistical significance. Both age and duration of detention were tested for normality. As neither variable was normally distributed, the median was used for reporting. To run logistical regressions and calculate the odds ratios for different outcomes, dummy variables were created for each possible value of the “last known status” and “profession” variables.
Finally, different logistical regressions were run to estimate the odds ratios of each detention outcome using multiple independent variables, including the profession, the reason for detention, and the province of detention for adjustment. The team used an alpha of .05 for statistical significance.
Interviews
In order to elucidate the risks health care workers took, the importance of the services they performed, and the consequences of their detainment by the Syrian government, the PHR team conducted a case study of detentions in the city of Aleppo. The case study relies heavily on interviews a PHR researcher with both country and health expertise conducted between August and October 2021. The PHR researcher interviewed four health care workers who were members of a health team operating in Aleppo in 2012 and who personally experienced detention, had firsthand knowledge of the detention and killing of other health care workers in Aleppo, or both. PHR’s researcher, a native speaker of both Syrian Arabic and English, conducted interviews remotely via Zoom in the language requested by interviewees. The researcher obtained oral informed consent to record the interviews. Primary data was transcribed and analyzed to extract key themes relating to detention of health care workers in Aleppo and the recordings were used to create transcripts of interviews. All personally identifiable information was removed to maintain interviewee confidentiality and safety. Recordings were stored in a secure folder after transcription. After the analysis was completed, the transcripts were stored on a secure PHR server, and the recordings were destroyed as described in the ERB human subjects research protocol. To cross-check dates and corroborate key details, the team consulted a contemporaneous written account of the events covered in the case study.[26] Any inconsistencies were shared with the interviewees for their review.
Desk Review
PHR’s team conducted open-source research to supplement the information from the dataset and the interviews. This desk review focused on the role of health care workers in the development of the Syrian uprising and their detention for providing care to protesters. In addition to PHR’s past interviews with detained health care workers, researchers consulted Google Scholar, Nexis Uni, and ProQuest academic databases, as well as open-source media web searches. Results included articles and reports in English and Arabic published by media outlets, human rights organizations, and UN agency reports from 2011 and later.
Limitations
The findings of this report must be interpreted in the context of eight main limitations. First, due to the Syrian government’s refusal to acknowledge its practice of arbitrary detention and enforced disappearances, it is difficult to independently verify the data sets. Second, because there is often greater awareness of when a person is detained compared to when they are released, the number of health care workers coded as “released” in the data set may be undercounted. Some health care workers may avoid identifying themselves as former detainees to organizations compiling records for multiple reasons, including threats by authorities and the social stigma of having been detained by the state and potentially being subjected to sexual violence or other abuse. For example, upon review of the combined dataset, a PHR researcher with extensive knowledge of the health sector in Aleppo noted that roughly one-tenth of health care workers in Aleppo with the last known status of “forcibly disappeared” had in fact been released (n=10). Third, the Syrian government does not report many of the deaths recorded in the data set. Instead, colleagues and family members often identified the bodies of detained health care workers based on the time when they were discovered at hospitals or appeared in leaked photographs of facilities run by security forces. Because the government provides no information about either detention or death, the number of deaths recorded in the data set is likely an undercount as well and represents the broader limitation of documenting deaths in the Syrian context. Fourth, dates for when health care workers died reflect when family members or colleagues learned of the death. In several cases, an unknown amount of time, ranging from days to years, may have passed between a health care worker’s death and when it was reported. Fifth, female health care workers comprise only 2 percent of the data set. While the overall population of detained health care providers is predominantly male, the social stigma associated with being detained is especially strong for women and likely contributes to an underrepresentation of women within the data set. Sixth, the data sets do not provide information about legal processes related to the release or death of detainees. Seventh, for the case study, the interviewees were asked to recollect traumatic events from a decade before, which may have led to memory bias. While the team sought to use multiple sources of data and cross-check the information provided, it is impossible to independently verify these personal, and often traumatic, accounts, especially concerning the experiences of health care workers who were killed. Lastly, the case study reflects the experiences of a group of health care workers in Aleppo and cannot be used to generalize the experiences of all health care workers in Aleppo or across Syria. Despite these limitations, this study presents a clear glimpse into the Syrian government’s use of detention to penalize health care workers and to reduce the amount of health care services available in the early stages of the Syrian uprising and provides a strong foundation for future study.
Results
Characteristics of Detainees
A total of 2,756 detention cases were merged from the three data sets, resulting in 1,685 unique detention events.[27] Of these, 77 events (4.6 percent) were attributed to 36 people who were detained multiple times.[28] In total, the Physicians for Human Rights (PHR) data set comprises 1,644 health care workers, including 1,607 male health care workers (97.7 percent) and 37 female health care workers (2.3 percent).[29] The research team determined age at detention for 233 cases. The median age was 32 years, with a minimum of 18 and maximum of 76. The team found no correlation between age and last known status.
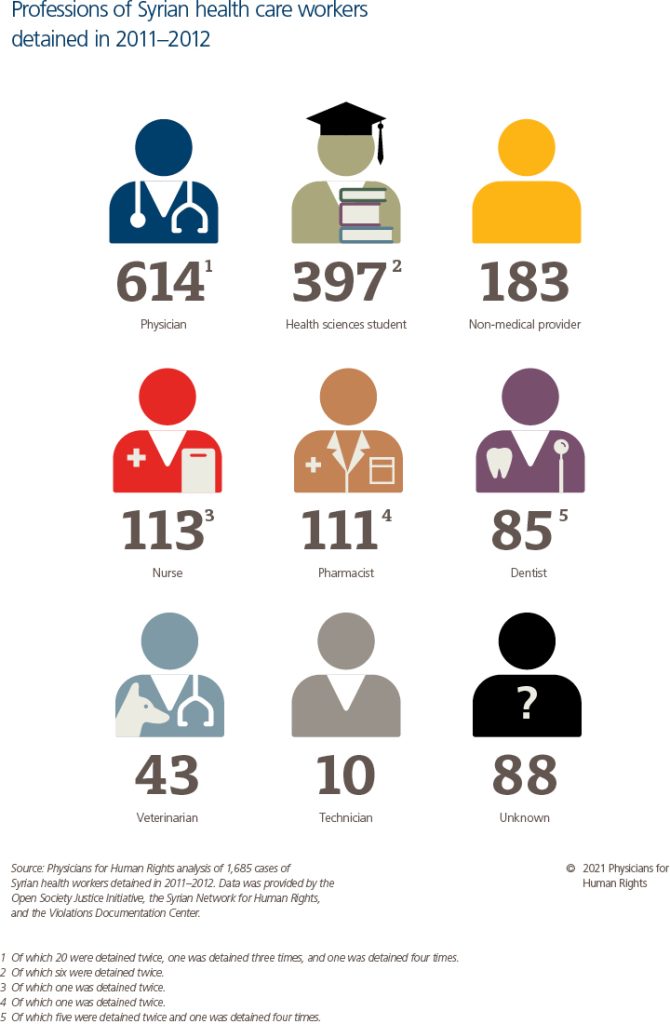
By profession, the PHR data set includes:
- 614 physicians (110 surgeons, 75 non-surgeon physicians, and 429 physicians whose specialty is unknown)
- 397 health sciences students
- 239 health care workers with degrees from medical universities (111 pharmacists, 85 dentists, and 43 veterinarians)
- 123 health care workers with degrees from health institutes (113 nurses and 10 technicians)
- 183 health care workers with non-health backgrounds
- 88 health care workers whose professions are unknown
The PHR research team determined the governorate of origin for 1,602 cases (95 percent) and the governorate of detention for 774 cases (46 percent).
Characteristics of Detention
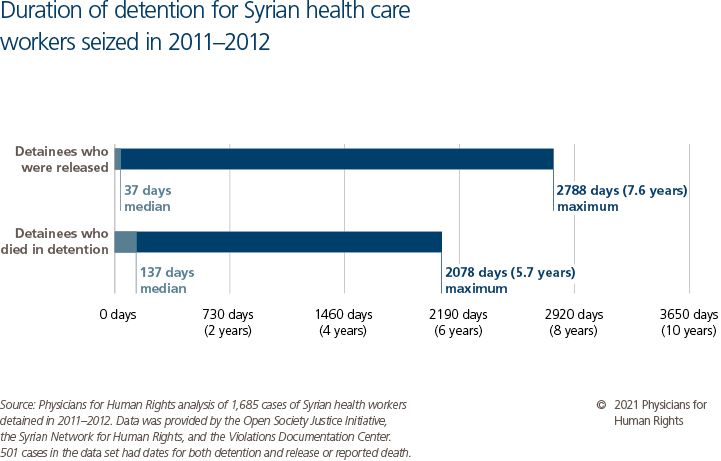
Only 31 cases (2 percent) in the PHR data set lack a date of detention. Of the released detainees, 443 cases (94 percent) had dates for both detention and release. The median length of detention was 37 days, with a maximum of 2,778 days (7.6 years). For detainees who were reported to have died while in detention, 58 cases (97 percent) included both date of detention and date of reported death. The median length of time that elapsed between a health care worker’s detention and reported death was 137 days (about 4.5 months), with a maximum of 2,078 days (5.7 years).
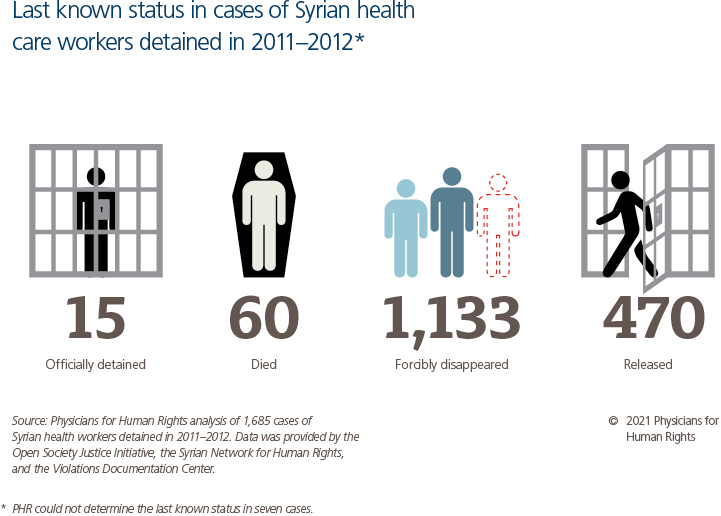
The possible classifications for the last known status variables include “released,” “died,” “detained,” “forcibly disappeared,” and “unknown.” The last known status for the majority of detentions in the PHR data set – 1,133 cases (67.5 percent) – was “forcibly disappeared,” meaning the government deprived the detainees of their liberty without a legal proceeding or official recognition that the disappearance had taken place. In fact, there was information suggesting a legal proceeding had occurred, leading to a designation of “officially detained,” in only 15 cases (1 percent). Of the remaining 31.5 percent of detentions, the team found 470 cases (28 percent) where a health care worker was released after being detained, and 60 cases where people (3.5 percent) died in detention. Of those who died, 15 (25 percent) were physicians, 18 (30 percent) were health care workers from non-health backgrounds, and 13 (22 percent) were health sciences students. Many detainees reportedly died during torture, were intentionally killed, or died from lack of medical care.[30] In at least one case, the notes indicated that the Syrian government reported the cause of death for a detainee as suicide, but a fellow detainee later reported that the person had been tortured to death. Detention events with a last known status of “unknown” (0.4 percent) were not included in any analysis using last known status.
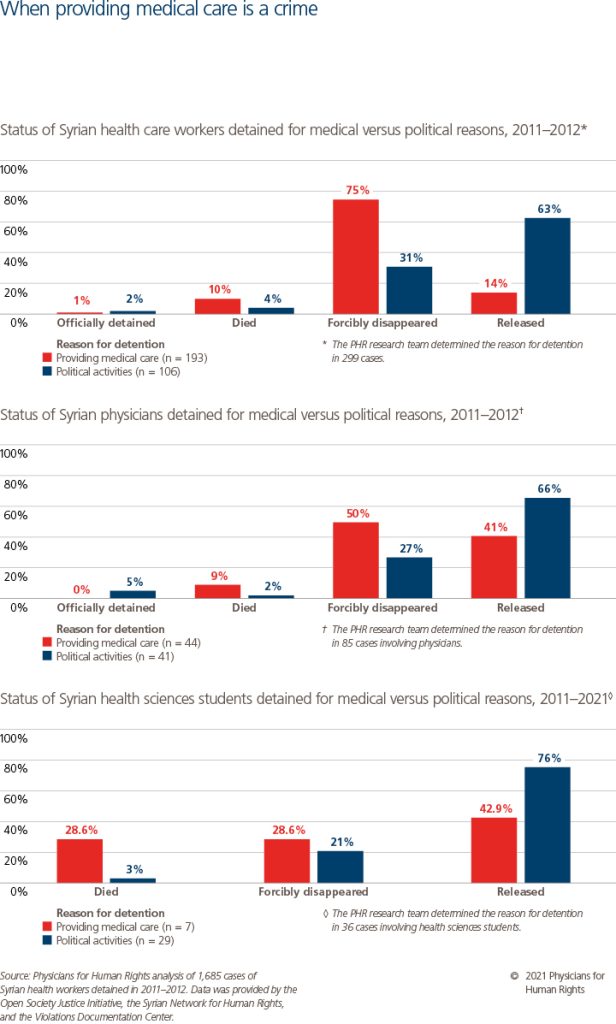
The PHR research team determined the reason for detention in 299 cases (18 percent). In 193 cases (64.5 percent), health care workers were detained for providing health care, including by working in a field hospital, transferring patients to medical facilities, offering medical treatment to protesters, or carrying medical equipment. In the remaining 106 cases (35.5 percent), the health care workers were detained due to their involvement in political activities, including participating in protests, engaging in peaceful acts of civil disobedience, and joining opposition parties. Of the health care workers who were detained for providing health care, 75 percent were forcibly disappeared, 10 percent died in detention, and only 14 percent were released. In comparison, among the health care workers detained for their political activities, only 31 percent were forcibly disappeared, 4 percent died, and the majority (63 percent) were released.
Associations Between Profession, Reason for Detention, and Last Known Status[31]
In bivariate analyses, there was a statistically significant correlation between reason for detention and last known status (P <.001). Overall, health care workers who were detained for providing medical care had 91 percent lower odds of being released than those who were detained for political reasons. These individuals were also 550 percent more likely to be forcibly disappeared compared to health care workers detained for political reasons. Within the same governorate and professional group, detainees who had provided medical care were 400 percent (P = .015) more likely to die in detention than detainees who were detained for political activities.
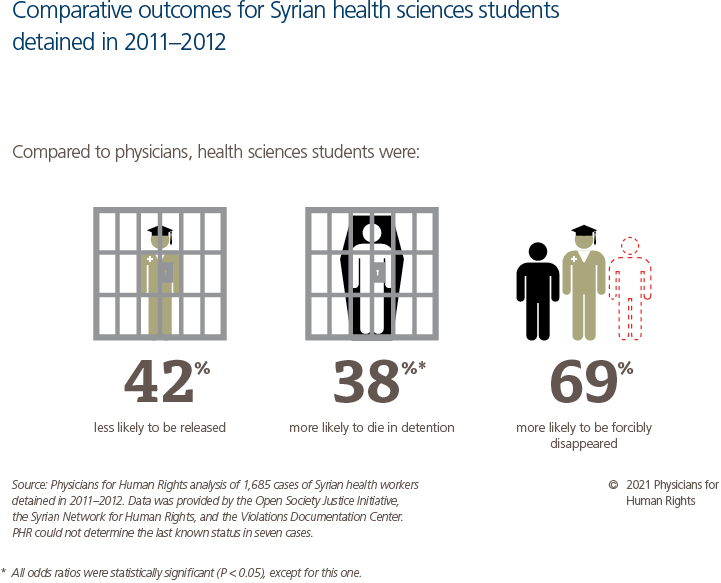
There was also a statistically significant correlation between detained health care workers’ professional group and their last known status (P < .001). The findings were particularly pronounced when comparing physicians and non-physicians. The odds that a physician would be released were 143 percent greater compared to a non-physician. Physicians were also 52 percent less likely to be forcibly disappeared and 48 percent less likely to die in detention compared to non-physicians (P = .03).
Each of the other four professional health care worker groups – detainees with university-level health science degrees (dentists, pharmacists, and veterinarians), institute-level health science degrees (nurses and technicians), health sciences students, and those with a non-health background – had higher odds of being forcibly disappeared and lower odds of being released compared to their physician peers. For enforced disappearance, dentists, pharmacists, and veterinarians had 66 percent higher odds (P = .001), nurses and technicians had 166 percent higher odds, health sciences students had 69 percent higher odds, and people with non-health backgrounds had 229 percent higher odds of being forcibly disappeared compared to physicians. These same groups had between 41 and 90 percent lower odds of being released compared to physicians (P ≤ .001). People with non-health backgrounds were also 353 percent more likely to die in detention than physician detainees. It is important to note, however, that most physicians in the PHR data set experienced poor outcomes. Only 255 physicians (40 percent) were released, while 359 (56 percent) were forcibly disappeared and 15 (2 percent) died in detention.
Discussion of Findings
Physicians for Human Rights’ (PHR) analysis yielded two main findings from the data on detention during this period: health care workers detained for providing medical care experienced worse outcomes than health care workers detained for political reasons, and among detained health care workers, physicians overall experienced better outcomes than non-physicians.
Reason for Detention and Outcomes: Health Care vs. Political Activity
As only 18 percent of cases in the data set had notes indicating the reason for detention, any interpretations of the differences in outcomes between medical and political detainees are tentative. With that caveat, the finding that health care workers who were detained because they had provided health care experienced worse outcomes then those detained for political reasons is striking. This finding could be interpreted as suggesting that government officials running the detention and interrogation system regarded providing medical aid to injured protesters as a more serious crime than participating in protests. This may be a result of the government assuming that health care workers detained for providing aid may have helped multiple protesters, thereby multiplying the perceived crime. Regardless of the reason, this finding reinforces the idea that the Syrian government decided to criminalize and harshly punish the provision of health care to protesters.
The finding that health care workers detained for providing health care had worse outcomes may also help explain the disparity in outcomes between physicians and non-physicians. Due to a relative lack of skills and experience, health sciences students and health care workers with non-health backgrounds may have been more active in providing basic first aid in the field compared to trained physicians. If these non-physicians were caught with medical supplies or while treating a protester at the scene of a protest, they would have had little room for disputing an accusation of providing health care. Physicians, on the other hand, would have greater deniability or could claim ignorance if detained on suspicion of treating protesters in a hospital. This may have influenced how interrogators and jailers perceived the severity of the crime, which could have affected both the treatment of health care workers in detention as well as the size of the bribes they were able to pay to secure their release. This would consequently help explain why physicians, with their greater economic means, appear to have been released more frequently than non-physicians.
Only three health care workers in the data set experienced detention more than twice, two of whom were detained four times. One of them was a dentist, and the other two were physicians. None of them were ever detained for providing health care, although the reason for detention was not known in every case. These three health care workers may have benefited from some unknown factor that allowed them to repeatedly exit the detention system alive. However, it is also possible that because none of them were detained for providing health care, and two were physicians who may have benefited from having wider professional networks and more economic resources, these health care workers were among the groups most likely to avoid poor outcomes.
Class and Status
Given that physicians represent the largest group of health care workers who were detained in our data set, the finding that physicians experienced better outcomes relative to other health care workers may seem paradoxical. These better outcomes, however, may be explained in part by the cultural and economic capital Syrian physicians enjoyed, particularly in the earliest years of the conflict. Specifically, their status as physicians may have provided access to a larger network of connections and to monetary resources that may have allowed them to navigate the detention process more successfully than non-physician detainees.[32]
When a person has been detained in Syria, there is strong evidence that social connections or “wasta” play a crucial role in the family learning the location of the detention site, the security service detaining their family member, and the alleged reason for detention.[33] Physicians in Syria, because of their role in the community, may have enjoyed larger professional networks that are capable of advocating on their behalf than non-physicians. These connections may have allowed family members and colleagues to locate where the detainee was in custody and communicate with the branch of the responsible security apparatus. Detainees whose families and colleagues lacked the necessary connections to access this information may have been at higher risk of disappearing into the Syrian government’s secretive detention system.
Once a detainee is located, the process of negotiating that person’s release may require a substantial amount of money. Systematic corruption within the detention system in Syria has created a significant source of revenue for government officials in positions to extort families and solicit bribes in exchange for securing the release of detainees.[34] Former detainees have reported that bribes were necessary for release and at times critical to avoiding death in detention. Physicians have historically received the highest salaries of all health care workers and may come from families with more economic resources.[35] Consequently, the families of physician detainees included in the PHR data set may have been better able to afford the price of survival.
Although the data set does not include information about detainees’ experience of cruel and inhuman conditions or torture, there is ample information that torture is common in Syrian detention facilities.[36] For example, the UN Commission of inquiry on Syria found that between March 2011 and November 2015, the Syrian government’s detainees were beaten and tortured to death or had inhuman living conditions inflicted on them, including serious over-crowding, lack of food, unclean drinking water, and lack of medical care.[37] This is also consistent with PHR’s previous research on the torture of health care workers detained by the government.[38]
Post-2014 Release Trend
Another important observation from the data set is that only six (1.3 percent) of the 470 cases of release occurred after 2014. Many reasons may account for this, including the mass forced displacement of millions of Syrians, both internally and abroad, Syria’s economic decline, and a possible shifting of government policy away from release of those detained for providing health services. The economic crisis in particular may have decreased the ability of many previously well-resourced families to afford bribes and may have disrupted personal networks. The punishment for providing health care may also have increased in severity as peaceful protests gradually gave way to armed opposition.
A Timeline of Events in Syria, 2011-2012
January to March
Health workers detained: 16
In March, government forces detain a medical student in Damascus for his participation in demonstrations. He is taken to Adra Central Prison and released the following month.
April to June
Detained health workers: 118
In May, government forces detain a physician in Damascus for his participation in protests against the regime. he remains in detention for almost a year.
July to September
Detained health workers: 208
In July, a hospital administrator in Idlib is detained by government forces for treating the wounded. He is forcibly disappeared by the regime.
October to December
Detained health workers: 135
In October, government forces detain a laboratory technicians in Hama. He is forcibly disappeared by the regime.
January to March
Detained health workers: 146
In March, government forces detain a nurse at the National Hospital in Hama. Only in November will his family learn that he was tortured to death while in detention.
April to June
Detained health workers: 139
In June, Air Froce security forces detain a physician in Aleppo and take him to the infamous Sednaya Military Prison in Damascus. He will be released nearly four years later, having lost more than 120 pounds.
July to September
Detained health workers: 208
In July, government forces enter a clinic in rural Damascus and detain a dentist. He is forcibly disappeared by the regime.
October to December
Health workers detained: 141
In November, government forces arrest a veterinarian in Latakia while he is on his way to work. He is forcibly disappeared by the regime.

“Protesters who were injured by the security and secret police could have been detained, tortured, or killed, had they sought normal medical care.”
Dr. Karim, a surgeon and member of the Noor al-Hayat medical team[39]
Aleppo’s Noor al-Hayat Medical Team
Killed for Treating Demonstrators
In the early days of the Syrian uprising, when the government of President Bashar al-Assad was violently suppressing peaceful demonstrations, 13 health care workers in Aleppo formed the Noor al-Hayat medical team to provide care to injured protesters. The group included two doctors, three dentists, a pharmacist, five medical students, and two non-health sciences university students. Before the uprising, each of them had enjoyed a peaceful life and a promising future. Within a year of Noor al-Hayat forming, half of the members had been detained and tortured, and four of them had lost their lives.
How the Noor al-Hayat Team Was Established
Throughout 2011 and 2012, Syrian security forces inflicted frequent and serious injuries on protesters peacefully demonstrating against the government. Wounded protesters were branded as criminals and “enemies of the state” and were threatened with detention and death if they attempted to seek care at public hospitals. “Security agents would come to the hospital, questioning and interrogating the injured,” said Dr. Bassam, a dentist. Because of these risks, in January of 2012, Dr. Mansur, a pulmonologist, established the Noor al-Hayat team to provide lifesaving medical care to anyone injured during peaceful demonstrations in the city of Aleppo. The team provided first aid at protest sites, performed emergency medical procedures in field settings – including private homes and other structures – and coordinated admissions to private hospitals when demonstrators required surgery. Since the Syrian government did not maintain a constant presence in all of Aleppo’s private hospitals, protesters seeking care in those hospitals were at lower risk of being found by security forces and detained.
How the Noor al-Hayat Team Carried Out its Work
When a demonstration began, the Noor al-Hayat team deployed to the area, ready to provide care. As protesters were injured, team members administered basic first aid using pre-prepared medical kits. Each kit contained several oropharyngeal tubes (used to maintain an open airway), a compression bandage, two tetanus injections, intravenous fluids (used to treat blood loss), and painkillers. The medical students were the team’s frontline health care providers, who attended demonstrations to treat emergency cases and identify victims with serious injuries. Dr. Karim, a surgeon, explained his role: “I was responsible for the field management, meaning I would refer cases to the appropriate hospital and reach an agreement with other doctors to treat the injured protesters.”
Treatment in any hospital – even a private one – was never completely safe, but other options were limited. Patients injured during protests would claim to have been attacked by “terrorist groups” to avoid being labeled as protesters and detained. However, some families decided it was too risky and preferred treatment at a field medical point – despite knowing they had minimal to no equipment and very low hygienic standards – to avoid the risk of their family member being detained at a hospital. “I remember a young, injured protester whose situation was critical,” Dr. Karim recalled. “His family refused [to admit him to a hospital], saying ‘The regime knows he is one of the protesters. They will kill him.’” Dr. Karim added that when a patient had surgery, the team would try to get him discharged as quickly as possible because “the police would come to check and see where he came from and how he was injured.” At one point, Dr. Karim recalled how security agents at a hospital tried to arrest a 16-year-old boy with a spinal cord injury. Dr. Karim and his wife joined a sit-in at the hospital to prevent the injured boy’s arrest. While the boy was ultimately not detained, Dr. Karim partially credited the success to someone leveraging their social connections to obtain “the help of someone with a critical role in Parliament.”

Detention, Torture, and Death
Dr. Mansur was an outspoken critic of the Syrian government. He posted on social media using his own name and actively encouraged the protest movement in Aleppo. He was detained by the government multiple times and died five months into his third detention in June 2012. During that time, he sent several messages to his family through detainees who had been released. He told his family he was being severely tortured. He asked them to pay bribes to set him free. When his family finally received his body, it was unidentifiable. He had lost more than 100 lbs in detention and his brother, a dentist, could only identify Dr. Mansur by a tooth that he had replaced.
On June 17, 2012, three student members of Noor al-Hayat – Abdullah, Hassan, and Ibrahim – were returning home at 1:00 a.m. after helping treat injured demonstrators. They were carrying a medical kit with them in the truck they rode in, identifying them as health care workers. Samir, a fellow Noor al-Hayat medical student member, recalled that they had planned to meet at the al-Razi hospital for training that evening. Samir last spoke to the group around 10:00 p.m., when they told him that they were attending to another patient and would not make it to the hospital that night. The next morning, Hassan’s family called the team and told them that Hassan never arrived home.
The team later learned that Abdullah had called a friend and told him that they were being stopped at a security checkpoint in the al-Hamdaniya neighborhood. Abdullah’s friend said that he immediately went to the area and saw the three students in the back of a security vehicle. When Hassan’s family realized that he was missing, they called his cell phone repeatedly. A person identifying himself as a government official answered Hassan’s phone and told them that their son had been detained. Samir remembers that they were air force security branch officers. The officers told Hassan’s parents, “You did not know [how] to educate your child, we will do that for you.” Hassan’s parents feared the worst because the accusation against him was of providing medical services. Immediately after the three students were detained, the remaining Noor al-Hayat members halted their work, removed all the medical equipment from the field hospitals, and avoided returning to their homes.
Samir recalled that six days after the students were initially detained, Ibrahim’s family received a call from their son’s phone. An official on the other end of the line directed them to a car that contained the burnt bodies of the students. Samir, who had worked in forensic medicine, accompanied Hassan’s brother to identify his body. “There were signs of beating and torture by flogging on his back,” Samir recalled. “We could identify Hassan because his body was not completely burned…. The worst part was that he was handcuffed and shackled so tight that you could see bone. He had a gunshot wound behind the left ear.”
Abdullah’s father and Ibrahim’s brother tried to identify the bodies of their loved ones, but their injuries had left them unrecognizable. Eventually, Ibrahim was identified by one of his shoes and Abdullah by his belt buckle. Later, graphic photos and videos appeared on the internet showing that Abdullah, Hassan, and Ibrahim had been burned with their hands tied behind their backs.[40] The brutal killing of the Noor al-Hayat team fueled a surge of protests in Aleppo.
“There were signs of beating and torture by flogging on his back…. We could identify Hassan because his body was not completely burned.”
Samir
Tortured but Released: Jamal and Rahim’s Story
After the burnt corpses of the three student volunteers were found, the remaining members of the Noor al-Hayat team resumed their work. However, the risks associated with their efforts had not decreased. Rahim described how he and his friend Jamal were detained after security forces caught them in possession of medical equipment. It was in August 2012, during Ramadan: “We had gone to get some food for Iftar [to break the fast], as well as to get some medical equipment … near the al-Bassel roundabout in New Aleppo,” Rahim recalled. Three agents from the nearby Military Security Directorate branch stopped them after their car had been reported for suspicious activity. When the security agents discovered the medical kit, they brought the students to the military security branch, located next to the roundabout.
At the branch office, Jamal and Rahim tried to claim they were volunteers with a government-approved organization, but the military security officers did not believe them. “I said goodbye to Jamal, and I thought we were definitely dead,” remembered Rahim. “We had a similar kit to the one Abdullah, Hassan, and Ibrahim had, and it is obvious we [were] from the same team.”
The cells were small, crowded rooms, with no furniture or mattresses. Rahim explained that they put detainees in a group cell measuring 5 x 6 meters (16.4 x 19.7 feet) with “40 or 50 people. I mean, if you wanted to lay down, you could not lay down on your back, you would have to be on your side and you [could] not extend your legs.” There were no toilets in the cells, and detainees were only allowed to use the bathroom twice every 24 hours. “They would allow you to use the toilet only until they counted to 10.”
“I said goodbye to Jamal, and I thought we were definitely dead.”
Rahim
Rahim recounted that, during interrogation, he was verbally abused and tortured. He described how his interrogators blindfolded and bound him, then hit him from all sides. He remembers them saying, “So, you’re treating the terrorists?” They tried to scare Rahim and Jamal by telling them that the other had pleaded guilty and told everything. “Me and Jamal were agreed that if we were caught, never to tell the truth whatever [happened], so we knew they were lying.”
Jamal and Rahim were held for 17 days. Neither believed that they would get out alive, thinking instead that they would be tortured to death. However, on the outside, Jamal’s relatives were using their connections to find out what had happened to the men and negotiate their release. In the end, Jamal’s family sold a house to afford the massive bribe that government officials demanded in exchange for facilitating the release of Jamal and Rahim. When the pair left the detention center, the security officials who had detained them told them to deny that they had ever been detained and never to discuss what was done to them.
Supporting Information from Previous PHR Documentation
The findings from PHR’s dataset regarding Syrian authorities’ criminalization of medical care are consistent with PHR’s longstanding research on the Syrian government’s attacks on health care facilities and providers.
In previous interviews that PHR conducted with health care workers who were detained between 2011 and 2012, interviewees recounted Syrian authorities telling them that they were detained for being doctors or for providing health care.[41] Interrogators accused many of the interviewees who worked in or helped establish field hospitals of providing medical treatment to “terrorists,” and/or of working to overthrow the Syrian government.
In October 2011, Air Force Intelligence agents arrested Dr. Ahmad, a surgeon, while he was operating on a patient with a thigh injury in Hama governorate. Dr. Ahmad subsequently learned during his interrogation that the authorities suspected the patient of being a “terrorist.” Dr. Ahmad’s act of providing medical care was the only justification given for his detainment. “My only crime was that I was a doctor,” he said.
Dr. Hadi, a pediatrician in Daraa, described being detained for possessing medical supplies at a checkpoint. “On August 9, 2012, in the late afternoon, I was stopped at a military checkpoint on the main highway between Daraa and Damascus,” Hadi recalled. “It was a 9th Armored Division checkpoint…. On that day, I was with a driver, and we were transporting a quantity of medical supplies – saline, antibiotics, gauze, medical plaster, etc. – to a field hospital in Daraa.” That same evening, an interrogator at the base accused Dr. Hadi of intending to equip a field hospital that treated protesters. Syrian authorities detained him without legal justification for nearly six months, during which he was repeatedly interrogated and tortured before he was finally released after paying a bribe to a judge.
In August 2011, Dr. Youssef was arrested as he was treating a patient in a hospital in the Qalamoun region, north of Rural Damascus governorate. Security forces took him to the al-Khatib State Security Branch, where interrogators repeatedly asked him about the medical point network he had helped to establish and demanded he identify the network’s members. His interrogators told him that they detained him for supporting “terrorists” and working against the regime.
Legal and Policy Analysis
Brief Legal Overview
While an in-depth legal analysis lies outside the scope of this report, this section addresses the overall legal implications of the data presented in this project and germane policy initiatives.
The permanent, nation-wide state of emergency declared in Syria in 1963 resulted in the emergence of a parallel judicial system. In this system, people perceived as threatening by the Syrian government were sent to both official and unofficial detention sites after trials in “exceptional courts,” including military courts and the Supreme State Security Court.[42] Some observers praised the Syrian government for suspending the emergency law on April 21, 2011.[43] Physicians for Human Rights’ (PHR) analysis demonstrates that this praise was misplaced. Significantly, in the months after the lifting of the emergency law, and before the December 1, 2011 United Nations (UN) determination that civil war was occurring in Syria, the government subjected health care workers,[44] among many thousands of others, to arbitrary detention and enforced disappearances in violation of its obligations under domestic law, international treaties, and customary international law. PHR’s qualitative research, including “My Only Crime Was That I Was a Doctor” and multiple other credible sources, suggest a high likelihood that torture and extrajudicial killing of health care workers occurred while they were in detention.[45] These practices were legitimized the following year when Syria’s counterterrorism laws were signed into legislation on July 2, 2012.[46] The definition of terrorism in these laws is so broad as to include any opposition to the Syrian government, including the provision of first aid or other medical care to individuals the government deems its opponents.[47] These laws have effectively recreated the exceptional court system by establishing a Counterterrorism Court.
Relevant Legal Framework
This report shows that health care workers were arbitrarily detained and forcibly disappeared during peaceful protests in the first eight months of the conflict, prior to the UN’s recognition of civil war in Syria. Its analysis finds poorer outcomes for health care workers charged with providing medical care than those engaged in political protest, which is corroborated by the interrogator’s statements reported in the case study and in earlier PHR interviews with health care workers across Syria. PHR finds that the Syrian government targeted health care workers with detention, abuse, and torture for providing medical assistance. The allegations merit a robust investigation of multiple violations of domestic laws, human rights law, and international humanitarian law.
Domestic Rule of Law Provisions
The Syrian Constitution (2012) provides theoretical protections against arbitrary detention as well as torture. Articles 51-53 of the Constitution articulate rule of law principles, including the presumption of innocence in trials, the right to counsel, the right to fair trial, the prohibition of torture and cruel treatment, and the prohibition of false imprisonment.[48] The Syrian Penal Code and the Code of Criminal Procedures provide for similar procedural protections.[49]
International Humanitarian Law (IHL)
This report focuses on the arbitrary detention and abuse of health care workers by the Syrian government in the first phase of the popular uprising. There is no consensus on when the non-international armed conflict in Syria – required for the application of international humanitarian law (IHL) – was established. For the purpose of this legal analysis, after the UN determination of civil war in Syria in December 2011, the conflict can be characterized as primarily a non-international armed conflict in which obligations arise under both international treaty and customary law.[50] The Geneva Conventions of 1949, which Syria ratified in 1953, are at the heart of IHL. They contain provisions related to protecting civilians, regulating detention, and safeguarding medical personnel. Common Article 3 of the Geneva Conventions applies to all parties to the conflict in Syria and contains specific stipulations on the equal and humane treatment of persons taking no active part in hostilities, including the passing of sentences and the carrying out of executions without previous judgment by a “regularly constituted court.”[51] In addition to the IHL obligations arising under treaty law, the Syrian government and other parties to the conflict in Syria are bound by customary international law (CIL) in conflicts, which provides protections against the arbitrary deprivation of liberty, enforced disappearances, torture and other cruel and inhuman punishment, and murder.[52] Significantly, CIL protects medical personnel engaged exclusively in medical duties, and prohibits the punishment of a person for performing medical duties as demanded by medical ethics.[53] By attacking medical workers in this context, the Syrian government has committed war crimes.
International Human Rights Law
Syria is party to multiple international treaties prohibiting arbitrary detention, abuse, and torture. It has ratified the International Covenant on Civil and Political Rights, which provides in relevant part the prohibition of torture (Art. 7) and arbitrary arrest or detention (Art. 9); the humane treatment of detainees (Art. 10); and the provision of fair trials (Art. 14).[54] The right to free speech (Art. 19) protects the choices of health care workers to participate in protests as well as to provide care to injured protesters. As discussed above, there is high likelihood that health care workers subjected to arbitrary detention and enforced disappearance have also experienced torture. Syria has ratified the Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment that requires States parties to actively prevent acts of torture in territories under their jurisdiction, allowing for no derogation under any circumstances, including in a state of war, internal instability, or public emergency.[55]
Syria has also ratified the International Covenant on Economic, Social and Cultural Rights (ICESCR), which provides in Article 12 the right to physical and mental health.[56] By systematically detaining health care workers, the Syrian government has not only decreased the census of available providers, it has also created a chilling effect on the provision of health care, no matter how basic, to unarmed protesters.
The UN defines arbitrary detention as depriving persons of their liberty in a way characterized by “elements of inappropriateness, injustice, lack of predictability and due process of law,”[57] which applies before, during, and after trial, as well as in the absence of a trial (administrative detention). As with arbitrary detention, enforced disappearances involve depriving a person of liberty against their will and without due process. An enforced disappearance has the added element of state involvement – either through direct action or by acquiescence – coupled with the state’s concealment of the fate of the disappeared person or refusal to acknowledge that the enforced disappearance occurred.[58]
In 2015, the United Nations, “on the basis of the general consensus of contemporary thought,” adopted the Standard Minimum Rules for the Treatment of Prisoners (the “Mandela Rules”). These rules establish good practices for the treatment of prisoners and the management of penal institutions.[59] Although they are not legally binding, they lay out international agreement on good principles and practice for the treatment of prisoners, and as such can be persuasive. The Mandela Rules provide that prison administrations must allow detainee contact with families, access to medical care, and sufficient water and food, in addition to preventing torture, ill-treatment, and sexual violence.[60]
Although Syria is not a party to the Rome Statute of the International Criminal Court, a referral to the court is possible through a range of mechanisms. Article 7 of the Rome Statute provides that when committed as part of “a widespread and systematic attack directed against any civilian population,” imprisonment or other deprivation of physical liberty, torture, and enforced disappearance may be considered crimes against humanity.[61]
Recognition of Truth as a Right
Critically for this report, the right to the truth relating to enforced disappearances or missing persons is recognized in a number of international legal instruments. Article 32 of Protocol I to the Geneva Conventions establishes “the right of families to know the fate of their [disappeared] relative.”[62] Although Syria has not signed the 2006 International Convention for the Protection of All Persons from Enforced Disappearance, it has ratified the ICESCR. The Economic and Social Council treaty body charged with monitoring compliance of signatories to the ICESCR has reaffirmed the “inalienable right to know the truth” regarding human rights violations, including enforced disappearances, and the truth regarding the fate and whereabouts of the disappeared persons, noting it is an absolute right, not subject to any limitation or derogation.[63] The UN Working Group on Enforced or Involuntary Disappearances has further elaborated on this principle by finding a right to know about the progress and results of an investigation, the circumstances of the disappearances, and the identity of the perpetrators.[64]
The Syrian government has carried out a policy of forcibly disappearing health care workers for the past decade, in violation of its international legal obligations, including under international humanitarian law, international human rights law, and its own domestic human rights protections. Enforced disappearances punish critics of the government but also create uncertainty and fear in a population as a way to discourage further opposition. As detailed above, the system into which so many Syrians have disappeared is subject to corruption and misinformation. Syria’s domestic and international legal obligations to the families of the missing and to detainees themselves must be addressed.
Policy Approach: Humanitarian Response and Justice
The UN Commission of Inquiry on Syria, noting that forced disappearances directly harm both detainees and families, has observed that the harms “represent a national trauma that will affect Syrian society for decades to come.”[65] Research has demonstrated that the disappearance and death in detention of significant others is associated with an increased risk of a range of serious psychological disorders.[66] Representatives of the families of detainees killed in detention or still missing have spoken publicly about the pain they have experienced. As the sister of a detainee who died in detention explained, “Neither I nor my mother can regain our previous lives, as long as the one who killed him still kills others and does not feel the guilt for what he did, nor how he injured and destroyed our lives.”[67] The mother of a detainee who was forcibly disappeared and is still missing explained that each of the missing “is a human soul with a full life to live. We’re not talking about numbers. We’re talking about humans, about our sons, about our loved ones.”[68]
Two main initiatives discussed below to address survivors’ needs – for information, closure, services, support, and ultimately for justice – include the Truth and Justice Charter movement and legal approaches using the principle of universal jurisdiction.
Survivor-led Justice Initiatives
In February 2021, a coalition of five Syrian organizations drafted a statement of goals called the “Truth and Justice Charter.”[69] These organizations represent survivors, their families, and family members of the missing who were subjected to arbitrary detention, enforced disappearance, torture, and serious ill-treatment in detention.[70] The Charter states,
“We differentiate between short-term justice and long-term justice. In the short term, there are immediate measures that must be taken to put a halt to ongoing violations and alleviate the suffering of survivors, victims, and their families. In the medium- to longer-term, we have additional demands to ensure comprehensive justice and non-repetition of the crimes we have suffered and continue to suffer from.”
The organizations have called for the UN to create a mechanism to follow a “strictly humanitarian approach” to address immediate needs.[71] However, it would also liaise with UN entities collecting information for future justice processes, including the Commission of Inquiry and the International, Impartial and Independent Mechanism to support their respective mandates.
Universal Jurisdiction Cases
Lawyers seeking justice for victims of grave crimes in Syria have pursued cases against perpetrators residing in the eight countries that have adopted “universal jurisdiction” legislation.[72] Universal jurisdiction allows a national court to prosecute individuals for serious crimes against international law — such as crimes against humanity, war crimes, genocide, and torture – on the principle that these crimes harm the international community itself, including the country in which the case has been filed. While universal jurisdiction offers a path forward for those seeking accountability for survivors and families of the missing, significant funding and capacity challenges remain.
Conclusion
Physicians for Human Rights’ (PHR) analysis suggests that from the earliest days of the uprising, even before the conflict began, the Syrian government embarked on a systematic and widespread campaign to detain anyone who provided medical assistance to protesters. In most cases, these health care workers were not lawfully arrested, charged, or given a fair trial. Instead, they were taken from their homes and places of work, seized while treating patients or traveling through checkpoints, and held in detention facilities where torture was rampant; many died or have not been heard from again. The pervasive illegality and opacity of the detention system appears to have acted as a breeding ground for corruption. Detainees who could leverage social connections and afford to bribe officials, as confirmed through numerous interviews, could secure their release. Those without social and financial capital faced intractable barriers, walls that were raised even higher if they were accused of providing health care.
The harm detailed in this report extends far beyond 2012, and even beyond the detainees themselves. What this report does not adequately show are the physical, mental, emotional, and social challenges that detainees can face even if they are released, especially after surviving torture, sexual violence, and other horrific abuse; nor does it cover the harm inflicted upon the families of the missing, who, every day, endure the pain of not knowing if their loved ones are being tortured in a detention site or lying in a mass grave.
A decade after the Syrian government began intensifying its practice of forcibly disappearing civilians, including health care workers, the conflict in Syria has entered a tenuous period of negotiation, with the potential for a fragile peace. However, justice and accountability remain elusive. As fighting continues unabated in some areas, the government of Syria, under the auspices of the Astana process aimed at achieving a ceasefire and agreement on humanitarian issues,[73] has entered into piecemeal negotiations to reclaim territory. In addition, some countries are encouraging the return of Syrians who fled their homeland. The Russian Federation, which has actively provided military support to the government of Syria since 2015, serves as a guarantor of its peace negotiations. PHR urges that the voices of the missing persons’ families be heard in the context of any negotiations going forward. While the nature of enforced disappearance makes it impossible to appreciate the full scale of violation and trauma, the UN has estimated that at least 100,000 people have been arbitrarily detained or forcibly disappeared. It is imperative for families to learn the truth about their loved ones’ disappearance, and, where possible, to retrieve their bodies. In addition to the need for truth, there is a longer-term need for justice and for accountability for the mass forced disappearance of opponents to the regime and those who provided care to the sick and wounded according to their ethical and moral imperatives. Health care workers are vital to the public health of their communities, but respect for the lives of all detainees and the need for truth and justice for the survivors must be recognized in both the short and the long term.
Recommendations
The status of detainees in Syria has been deemed fundamental to any political negotiation between the parties to the conflict, but with limited results.[74] The Syrian government is now seeking to normalize diplomatic relations with the international community, particularly its neighboring states. This creates a critical opportunity for the international community to explore new methods to pressure all parties to the conflict to negotiate for the release of detainees and to demand transparency from the Syrian government about the status of those who have died in detention. Physicians for Human Rights makes the following recommendations:
To the Syrian Government and Affiliated Forces, and All Parties to the Conflict:
- Immediately and unconditionally release all arbitrarily or unlawfully detained individuals from official and unofficial detention sites;
- When facilitating the release of all arbitrarily detained people, special attention should be given to the most vulnerable, including children, women, the elderly, and the disabled;
- In response to the Truth and Justice Charter, create a national-level channel for Syrians to report and seek information about their missing and disappeared loved ones;
- Take immediate and systemic measures to prevent the torture and ill-treatment of detainees and ensure that allegations of abuse are investigated, and abusers held accountable;
- Disclose the locations of all official and unofficial detention sites and provide comprehensive lists of all those held in those sites;
- Share information with families on the location and status of detained and abducted relatives. When applicable, notify families of the circumstances of death and the location of burial sites;
- Establish and abide by a timetable for the release of detainees and information about the missing;
- Grant impartial and independent entities access to all prisons and detention sites, regardless of the entities’ official status;
- Improve detention conditions in compliance with international standards, including through ensuring detainee contact with families, access to medical care, and sufficient water and food, as well as preventing torture, ill-treatment, and sexual violence. This is especially critical in the context of the COVID-19 pandemic; and
- Respect health services and protect medical personnel, patients, facilities, and transport from attack or interference.
To the Russian Federation: (As the main supporter of the Syrian government and a party to the conflict in Syria)
- Use influence to press the Syrian government to implement the above-listed recommendations, focusing on the unconditional release of those arbitrarily detained, disclosing information to families on the fate and whereabouts of detained relatives, and granting access by international monitors to detention sites; and
- Support UN Security Council (UNSC) measures to accelerate the release of the arbitrarily detained, including medical personnel, in accordance with resolutions 2139 and 2254.
To the United Nations Security Council:
- Address non-implementation of prior UN Security Council resolutions by adopting a stand-alone resolution on the situation of detainees and missing persons, setting out in detail the steps that the government of Syria is required to take under international law;
- Enforce accountability by referring the situation in Syria to the Prosecutor of the International Criminal Court;
- Adopt targeted sanctions against persons, agencies, and groups credibly suspected of being responsible for or complicit in conduct leading to arbitrary arrests, custodial deaths, torture, and enforced disappearances;
- Encourage all parties to the conflict to abide by UNSC resolutions 2139, 2254, 2268, and 2474 and draw specific attention to the targeting of medical personnel; and
- Continue to reinforce the work of the International, Impartial and Independent Mechanism to Assist in the Investigation and Prosecution of Persons Responsible for the Most Serious Crimes under International Law committed in the Syrian Arab Republic since March 2011, and the Independent International Commission of Inquiry on the Syrian Arab Republic, which are charged respectively with collecting and storing information about and investigating alleged violations of international human rights law.
To the UN Special Envoy for Syria:
- Ensure that discussions of human rights and international humanitarian law violations, including arbitrary detention, enforced disappearances, torture, extrajudicial killings, and attacks on health, are prominent within the political process; and
- Re-insert the issue of detainees, abductees, and the missing into the framework of the Geneva peace process and push the Astana Guarantors to widen the scope of the Working Group on Detainees and Abductees beyond its current focus on low-level one-to-one prisoner exchange and into a scalable release of civilian prisoners.
To UN Member States:
- Coordinate efforts and endorse the Truth and Justice Charter and ensure that survivor-led short- and long-term plans for peace and accountability are the main driver of decision making;
- Support the creation of an independent and impartial mechanism to seek the truth about the fate and whereabouts of missing and forcibly disappeared people in Syria; and
- Exercise international and domestic law, including universal jurisdiction principles, to investigate and prosecute Syrian military and civilian officials responsible for carrying out war crimes and crimes against humanity against detainees in Syria. Ensure cooperation among states, including sharing of evidence bilaterally, where possible, with national prosecutors who are pursuing these cases in domestic courts.
Acknowledgments
This report was written by Physicians for Human Rights (PHR) staff members Houssam al-Nahhas, MD, MPH, MENA researcher (November 2020 – August 2021); Andrew Moran, Syria research and investigations associate; and an anonymous author. Adrienne L. Fricke, JD, MA, senior research fellow, Harvard Humanitarian Initiative, and visiting scientist at the Harvard T.H. Chan School of Public Health, contributed to the research and writing. Hala Mkhallalati, MSc, research associate, Saw Swee Hock School of Public Health, National University of Singapore, contributed to the writing and conducted interviews. Joseph Leone, former research and investigations fellow, contributed to the project concept memo. MENA interns Youssef Aziz, Sarah Kebaish, Samantha Scheer, and an anonymous MENA intern provided research assistance.
PHR leadership and staff contributed to the writing and editing of this report, including Michele Heisler, MD, MPA, medical director; Donna McKay, MA, executive director; Karen Naimer, JD, LLM, MA, director of programs; Michael Payne, deputy director of advocacy; and Susannah Sirkin, MEd, director of policy and senior advisor.
The report benefited from review by PHR Board Member Emeritus Robert S. Lawrence, MD; Mohammad Darwish, MD, MPH, associate faculty at the Center for Humanitarian Health, Department of International Health at John Hopkins Bloomberg School of Public Health; Mohamad Katoub, MD, research fellow, Syria Impacts Study, University of California, Berkeley, School of Public Health; and Steve Kostas, JD, PhD, senior legal officer, Open Society Justice Initiative. It was reviewed, edited, and prepared for publication by Claudia Rader, MS, senior communications manager, with assistance from Abigail Daly, communications intern. Hannah Dunphy, MA, digital communications manager, prepared the digital presentation.
PHR would like to thank the Open Society Justice Initiative, the Syrian Network for Human Rights, and the Violations Documentation Center for the data they shared. PHR is grateful to Ali Barazi and his associates for translation services. PHR is especially indebted to the former members of the Noor al-Hayat Medical Team who agreed to be interviewed.
This report is supported in part by funding from the German Federal Foreign Office’s Institute für Auslandsbeziehungen, through the zivik Funding Programme.
Endnotes
[1] These concessions included the repeal of a 48-year-old state of emergency law that the government had used for decades to arbitrarily detain perceived opponents.
[2] United Nations Human Rights Council (UNHRC), Independent International Commission of Inquiry (CoI) on Syria, “Assault on medical care in Syria” (A/HRC/24/CRP.2), September 17, 2013.
[3] United Nations Security Council, “Security Council Failing Thousands of People Detained, Abducted in Syria, Civil Society Speakers Say, Demanding Information about Missing Persons’ Whereabouts,” (A/HRC/46/55), August 7, 2019, https://www.un.org/press/en/2019/sc13913.doc.htm, at para 23.
[4] UNHRC, Report of the Independent International Commission of Inquiry on the Syrian Arab Republic (A/HRC/46/55), March 11, 2021.
[5] Truth and Justice Charter: A Common Vision on the Question of Enforced Disappearance and Arbitrary Detention in Syria by Syrian Victims’ and Family Members’ Organisations, February 2021, https:/www.impunitywatch.org/truth-and-justice-charter-syria.
[6] UNHRC, “Assault on medical care,” note 1. (“The deliberate targeting of hospitals, medical personnel and transports, the denial of access to medical care, and ill-treatment of the sick and wounded, has been one of the most alarming features of the Syrian conflict”).
[7] For a discussion of field hospitals, see Rayan Koteiche, “My Only Crime Was That I Was a Doctor: How the Syrian Government Targets Health Workers for Arrest, Detention, and Torture,” Physicians for Human Rights, December 4, 2019, https://phr.org/our-work/resources/my-only-crime-was-that-i-was-a-doctor/.
[8] Personal communication with former health care worker detainee, October 9, 2021, on file with PHR.
[9] For a discussion of Syrian detention centers’ extortion practices, see Association of Detainees and the Missing in Sednaya Prison (ADSMP), “Forcibly Disappeared in Syrian Detention Centers,” December 2020, https://www.admsp.org/wp-content/uploads/2021/07/Forcibly-Disappeared-in-Syrian-EN.pdf.
[10] Joseph Holliday, “The Assad Regime: From Counterinsurgency to Civil War,” The Institute for the Study of War, March 2013, http://www.understandingwar.org/sites/default/files/TheAssadRegime-web.pdf.
[11] Andrew Osborn, “Russia begins Syria air strikes in its biggest Mideast intervention in decades,” Reuters, September 30, 2015, https://www.reuters.com/article/us-mideast-crisis-russia/russia-begins-syria-air-strikes-in-its-biggest-mideast-intervention-in-decades-idUSKCN0RU0MG20150930; Christiaan Triebert, “How Times Reporters Proved Russia Bombed Syrian Hospitals,” New York Times, October 13, 2019, https://www.nytimes.com/2019/10/13/reader-center/russia-syria-hospitals-investigation.html.
[12] The main Syrian security services are the Department of Military Intelligence (Shu`bat al-Mukhabarat al-`Askariyya); the Air Force Intelligence Directorate (Idarat al-Mukhabarat al-Jawiyya); the Political Security Directorate (Idarat al-Amn al-Siyasi); and the General Intelligence Directorate (Idarat al-Mukhabarat al-`Amma).
[13] For an overview of the intelligence system, see Andrew Rathmell, “Syria’s Intelligence Services: Origins and Development: Origins and Development,” Journal of Conflict Studies 16, no. 2 (1996): 75-96.
[14] UNHRC, Report of the Independent International Commission of Inquiry on the Syrian Arab Republic (A/HRC/46/55), March11, 2021, at para 15.
[15] “Syria protests: Assad to lift state of emergency,” BBC News, April 20, 2011, https://www.bbc.com/news/world-middle-east-13134322.
[16] Human Rights Watch, “Syria: Counterterrorism Court Used to Stifle Dissent,” June 25, 2013, https://www.hrw.org/news/2013/06/25/syria-counterterrorism-court-used-stifle-dissent.
[17] Diwan, “Local Coordination Committees of Syria,” Carnegie Middle East Center, https://carnegie-mec.org/diwan/50426?lang=en.
[18] Open Society Justice Initiative (OSJI), a team of human rights lawyers and staff pursuing strategic litigation and other legal work to promote global human rights, national security, and more, https://www.opensocietyfoundations.org/who-we-are/programs/open-society-justice-initiative; Syrian Network for Human Rights (SNHR), an independent human rights organization working to monitor, document, and combat human and civil rights violations in Syria, https://sn4hr.org; Violations Documentation Center (VDC), a project of the Syrian Center for Media and Freedom of Expression that has worked since 2011 on documenting violations of human rights law and international humanitarian law in the context of the Syrian conflict, https://www.vdc-sy.info/index.php/en/about.
[19] For the governorate of detention, the team used references to cities, neighborhoods, towns, and other geographic identifiers to determine the governorate. The team used the most recent administrative map of Syria to distinguish between Damascus (Dimashq) and Rural Damascus (Rif Dimashq). When health care workers were detained while traveling between two different governorates and it was unclear where the detention occurred, the team recorded the governorate from which they were traveling.
[20] Data for professions was initially organized into 11 groups: surgeons, non-surgeon physicians, non-specified physicians, dentists, pharmacists, veterinarians, nurses, technicians, health science students, non-health background, and unknown. The “non-health background” group was composed of people without advanced training in health sciences, such as ambulance drivers, first aid providers, medical equipment distributors, and non-health sciences students. Note that some nurses included in this group may have four-year university degrees. The data does not distinguish between two- and four-year degrees for nursing.
[21] UN Office of the High Commissioner for Human Rights (OHCHR), “Definition of enforced disappearances,” https://legal.un.org/ilc/sessions/71/pdfs/english/cah_un_wg_disappearances.pdf.
[22] Only numbers equal to or greater than zero were accepted.
[23] The team made exceptions in three instances: one in which governorate of origin differed between two cases, but every other variable matched, including the person’s first name, father’s name, and family name; and two other instances where a single variable conflicted between cases, but the notes sections included detailed references to other detention events in the data set.
[24] Microsoft Corporation, (365), Microsoft Excel, retrieved from https://office.microsoft.com/excel.
[25] StataCorp, 2019, Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC.
[26] Written account on file with PHR MENA team.
[27] There is no authoritative figure for the total number of those arbitrarily detained or forcibly disappeared by the Syrian government, although the UN CoI estimates tens of thousands over the past decade. This is not a comprehensive analysis of detention-related events; however, the sample allows insight into trends in outcomes among individuals providing health care.
[28] This means that there were 1,644 cases in the data set that were initial detention events and 41 cases where a health care worker was detained for a second, third, or fourth time.
[29] As discussed in the methodology section, there are limitations on the information in the data set due to the unavailability of information about deaths and releases from the Syrian government, and the stigma of detention that may have contributed to the undercounting of detainees, and especially women.
[30] UNHRC, “Out of Sight, Out of Mind: Deaths in Detention in the Syrian Arab Republic,” February 3, 2016, A/HRC/31/CRP.1, https://www.refworld.org/docid/56b9f4c24.html.
[31] StataCorp, 2019, Stata Statistical Software: Release 16, College Station, TX: StataCorp LLC; All odd ratios were statistically significant with P values less than .001, unless otherwise noted.
[32] Physicians’ ability to leverage social networks and wealth may have decreased over time. The CoI noted in March 2021 that a wide range of corrupt practices involving extortion, bribery, and “exploiting family members’ desperate pursuit of information” have increased due to the worsening economic situation. CoI, March 11, 2021, (A/HRC/46/55), para 108.
[33] For a discussion of the importance of social networking and “wasta” generally, see Annika Kropf, “Wasta as a Form of Social Capital? An Institutional Perspective,” in Tanya Cariina Newbury-Smith, The Political Economy of Wasta: Use and Abuse of Social Capital Networking, 2016.
[34] CoI, A/HRC/46/55 para 108, note 32 above.
[35] Elisabeth Longuenesse, “Ingénieurs et médecins en Syrie: formation, emploi, statut social” Tiers-Monde, tome 36, n°143, 1995. (“The situation of the doctor is relatively favorable compared to the engineer or any other high-level profession: private practice ensures him at worst an income three times that of a university professor.”), PHR’s translation.
[36] For examples, see Human Rights Watch, “If the Dead Could Speak: Mass Deaths and Torture in Syria’s Detention Facilities,” December 16, 2015, https://www.hrw.org/report/2015/12/16/if-dead-could-speak/mass-deaths-and-torture-syrias-detention-facilities; ECCHR, “Photographs and data from the Caesar-File Group,” https://www.ecchr.eu/fileadmin/Hintergrundberichte/Background_Syria_Torture_CaesarFiles_GermanyCriminalComplaint_ECCHR_August_2019.pdf.
[37] UNHRC, “Out of Sight, Out of Mind.”
[38] PHR “My Only Crime Was That I Was a Doctor.”
[39] All names of team members are pseudonyms that PHR generated.
[40] PHR researchers reviewed the images and videos of Abdullah’s, Hassan’s, and Ibrahim’s bodies.
[41] Note that all names are pseudonyms. Interviews were conducted as research for the PHR report “My Only Crime Was That I Was a Doctor.”
[42] The “exceptional” courts were established for use during armed conflict by Legislative Decree No. 109 of 17 August 1968, which was amended to include periods of “domestic unrest.” See, Mikael Ekman, ed, “ILAC Rule of Law Assessment Report: Syria 2017,” International Legal Assistance Consortium, April 2017,http://www.ilacnet.org/wp-content/uploads/2017/04/Syria2017.pdf.
[43] Syria protests: Assad to lift state of emergency,” BBC News, April 20, 2011, https://www.bbc.com/news/world-middle-east-13134322 (cited above at note 13).
[44] In this report, the term “health care worker” refers to individuals who, at the time of attack or detention, were engaged professionally or as volunteers in the search for, or collection, transportation, diagnosis, or treatment of the wounded and sick (including provision of first aid) and in the prevention of disease.
[45] Rick Gladstone and Malachy Brown, “In Syria, Health Workers Risk Becoming ‘Enemies of the State,’” New York Times, December 4, 2019, https://www.nytimes.com/2019/12/04/world/middleeast/syria-health-workers-persecution.html.
[46] “Law 19, Anti-Terrorism Law,” http://www.parliament.gov.sy/arabic/index.php?node=55151&cat=4306.
[47] The Tahrir Institute for Middle East Policy, “Brief: Law No.19 of 2012: Counter-terrorism Law,” January 7, 2019, https://timep.org/reports-briefings/timep-brief-law-no-19-of-2012-counter-terrorism-law/. See also: Syrian Network for Human Rights, “At Least 10,767 Persons Still Face Trial in Counter-Terrorism Court, nearly 91,000 Cases Heard by the Court,” October 15, 2020, https://reliefweb.int/report/syrian-arab-republic/least-10767-persons-still-face-trial-counter-terrorism-court-nearly.
[48] Syrian Arab Republic’s Constitution of 2012, “Chapter II: Rule of Law,” 11, https://www.constituteproject.org/constitution/Syria_2012.pdf?lang=en.
[49] Abduction, assault, and kidnapping are all prohibited by the Syrian Penal Code (1949).
[50] For IHL to apply, the conflict between the government and the insurgents must meet a level of intensity in which the government “is obliged to use military force … instead of mere police forces.” In order to be a “party to the conflict,” a non-state armed group must possess a command structure and the capacity to sustain military operations. For a detailed introduction to the issue, see ICRC opinion paper, “How is the Term ‘Armed Conflict’ Defined in IHL?” March 2008, https://www.icrc.org/en/doc/assets/files/other/opinion-paper-armed-conflict.pdf.
[51] International Committee of the Red Cross (ICRC), The Geneva Conventions, August 12, 1949, 36, https://www.icrc.org/en/doc/assets/files/publications/icrc-002-0173.pdf.
[52] Customary International Humanitarian Law, ICRC, “Rule 99: Deprivation of Liberty,” Vol. II, Ch. 32, Sec. L.; Customary International Humanitarian Law, ICRC, “Rule 90: Torture and Cruel, Inhuman or Degrading Treatment,” Vol. II, Ch. 32, Sec. D.; Customary International Humanitarian Law, ICRC, “Rule 98: Enforced Disappearance,” Vol. II, Ch. 32, Sec. K.; Customary International Humanitarian Law, ICRC, “Rule 89: Violence to Life,” Vol. II, Ch. 32, Sec. C.
[53] Customary International Humanitarian Law, ICRC, “Rule 25: Medical Personnel, Vol. II, Ch. 7, Sec. A; Customary International Humanitarian Law, ICRC, “Rule 26: Medical Activities, Vol. II, Ch. 7, Sec. B.
[54] OHCHR, International Covenant on Civil and Political Rights, Art. 7, 9 10, 14, rat. March 23, 1976, https://www.ohchr.org/en/professionalinterest/pages/ccpr.aspx.
[55] UN General Assembly, Convention Against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, 10 December 1984, United Nations, Treaty Series, vol. 1465, p. 85, https://www.refworld.org/docid/3ae6b3a94.html.
[56] OHCHR, International Covenant on Economic and Social Rights, Art. 12, rat. January 3, 1976, https://www.ohchr.org/en/professionalinterest/pages/cescr.aspx.
[57] OHCHR, “About arbitrary detention,” https://www.ohchr.org/EN/Issues/Detention/Pages/AboutArbitraryDetention.aspx.
[58] Report of the Working Group on Enforced or Involuntary Disappearances, January 26, 2011, https://undocs.org/A/HRC/16/48.
[59] UN General Assembly resolution 70/175, annex, adopted on December 17, 2015, https://www.unodc.org/documents/justice-and-prison-reform/Nelson_Mandela_Rules-E-ebook.pdf.
[60] It is worth noting that the Syrian government has released only a few prisoners during the COVID-19 pandemic, despite fears of mass infections. Suleiman Al-Khalidi, “Syria slow to free prisoners despite coronavirus risk in crowded jails: rights groups,” Reuters, April 6, 2020, https://www.reuters.com/article/us-health-coronavirus-syria-jails/syria-slow-to-free-prisoners-despite-coronavirus-risk-in-crowded-jails-rights-groups-idUSKBN21O1WO.
[61] UN General Assembly, Rome Statute of the International Criminal Court (last amended 2010), 17 July 1998, ISBN No. 92-9227-227-6, https://www.refworld.org/docid/3ae6b3a84.html.
[62] ICRC, Protocol Additional to the Geneva Conventions of 12 August 1949, and relating to the Protection of Victims of International Armed Conflicts (Protocol I), 8 June 1977, 1125 UNTS 3, https://www.refworld.org/docid/3ae6b36b4.html.
[63] Diane Orentlicher, UN independent expert, “Updated Set of principles for the protection and promotion of human rights through action to combat impunity,” Economic and Social Council, E/CN.4/2005/102/Add.1, February 8, 2005, https://documents-dds-ny.un.org/doc/UNDOC/GEN/G05/109/00/PDF/G0510900.pdf?OpenElement.
[64] Report of the Working Group on Enforced or Involuntary Disappearances, January 26, 2011, https://undocs.org/A/HRC/16/48.
[65] UNHRC, Report of the Independent International Commission of Inquiry on the Syrian Arab Republic (A/HRC/46/55),March 11, 2021, para 105.
[66] Diagnoses include prolonged grief disorder (PGD), post-traumatic stress disorder (PTSD), and major depressive disorder (MDD). L.I.M Lenferink, et al, “Cognitive-Behavioral Correlates of Psychological Symptoms Among Relatives of Missing Persons,” J Cogn Ther 11,311–324 (2018).
[67] See note 9.
[68] Fadwa Mahmoud, Families for Freedom, as cited in Jeremy Sarkin, “Humans not Numbers: The Case for an International Mechanism to Address the Detainees and Disappeared Crisis in Syria,” May 2021, https://cad5e396-f48c-4e90-80f5-27ccad29f65e.filesusr.com/ugd/f3f989_ea155e7ebd6940d1b4a11cd0057af7d0.pdf.
[69] Truth and Justice Charter, at note 4.
[70] The organizations include The Association of Detainees and Missing Persons in Sednaya Prison, Caesar Families Association, the Coalition of Families of Persons Kidnapped by ISIS (Massar), Families for Freedom, and the Ta’afi Initiative.
[71] For a detailed discussion of the proposed mechanism, see Jeremy Sarkin, “Humans not Numbers.”
[72] The countries who have adopted universal jurisdiction legislation include Canada, Finland, France, Germany, The Netherlands, Norway, Sweden, and Switzerland. For an overview of the comparative legal frameworks in each country, see TRIAL International, “Prosecuting International Crimes: a Matter of Willingness,” May 5, 2020, https://trialinternational.org/latest-post/prosecuting-international-crimes-a-matter-of-willingness/.
[73] See e.g., “Joint Statement by Iran, Russia, Turkey on the International Meeting on Syria in Astana, 23-24 January 2017,” p.1, https:/www.peaceagreements.org/viewmasterdocument/2092. For a brief overview of the process, see France 24, “Syria: the Astana peace process,” September 5, 2018, https://www.france24.com/en/20180905-syria-astana-peace-process.
[74] Four UN Security Council resolutions on Syria (UNSC 2139, 2254, 2268, 2474) have addressed arbitrary detention and enforced disappearances. The UN Special Envoy for Syria has emphasized the need to release detainees and abductees and clarify the fate of missing persons in the third, fourth, and fifth Brussels Conference Co-chairs declarations. Regrettably, the recommendations from PHR’s 2019 report on the targeting of health care workers, “My Only Crime Was that I Was a Doctor,” still apply.