
Executive Summary
In August 2017, the armed forces of Myanmar (Tatmadaw) unleashed a campaign of widespread and systematic attacks on the country’s Rohingya communities, escalating previous episodes of violent human rights abuses committed against the Rohingya population. The United Nations (UN) and multiple human rights groups documented that Myanmar security forces committed rape, gang rape, sexual slavery, forced nudity, genital mutilation and other forms of violence targeting sexual organs, sexual assault, and threats and attempts at rape and sexual assault, followed by the killing of victims. In numerous instances, survivors recounted being forced to witness the rape or sexual assault of family or community members. Following what the Myanmar government called “clearance operations,” more than 720,000 Rohingya fled to neighboring Bangladesh. Analyses of these atrocities suggest that sexual violence is a deliberate strategy used by the Tatmadaw to intimidate, terrorize, punish, and forcibly displace the Rohingya civilian population from their land.
For more than 15 years, Physicians for Human Rights (PHR) has documented the persecution of the Rohingya and other ethnic minorities in Myanmar. In 2017 and 2018, PHR carried out forensic examinations of survivors and gathered qualitative and quantitative data corroborating the serious human rights violations committed against the Rohingya in August 2017.
Few studies have documented the experience of Rohingya refugees through the lens of the people who cared for them in Bangladesh – doctors, nurses, mental health experts, and other health professionals. PHR sought the perspective of health care workers in order to provide an independent corroboration of the patterns of violence sustained by the Rohingya community.
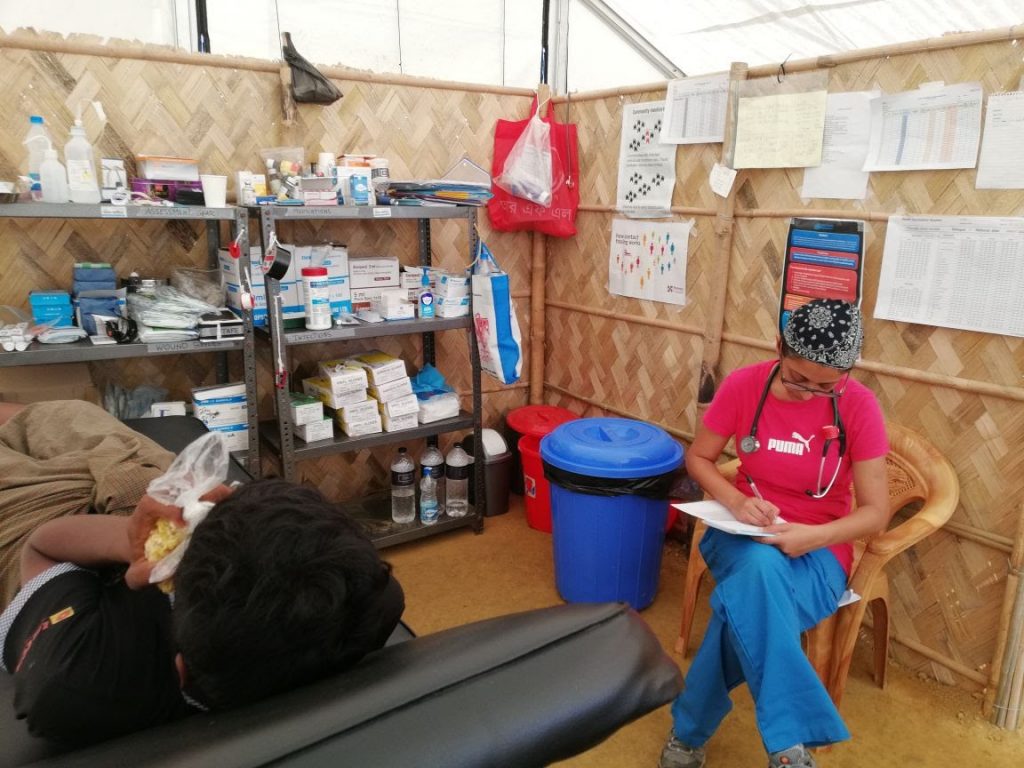
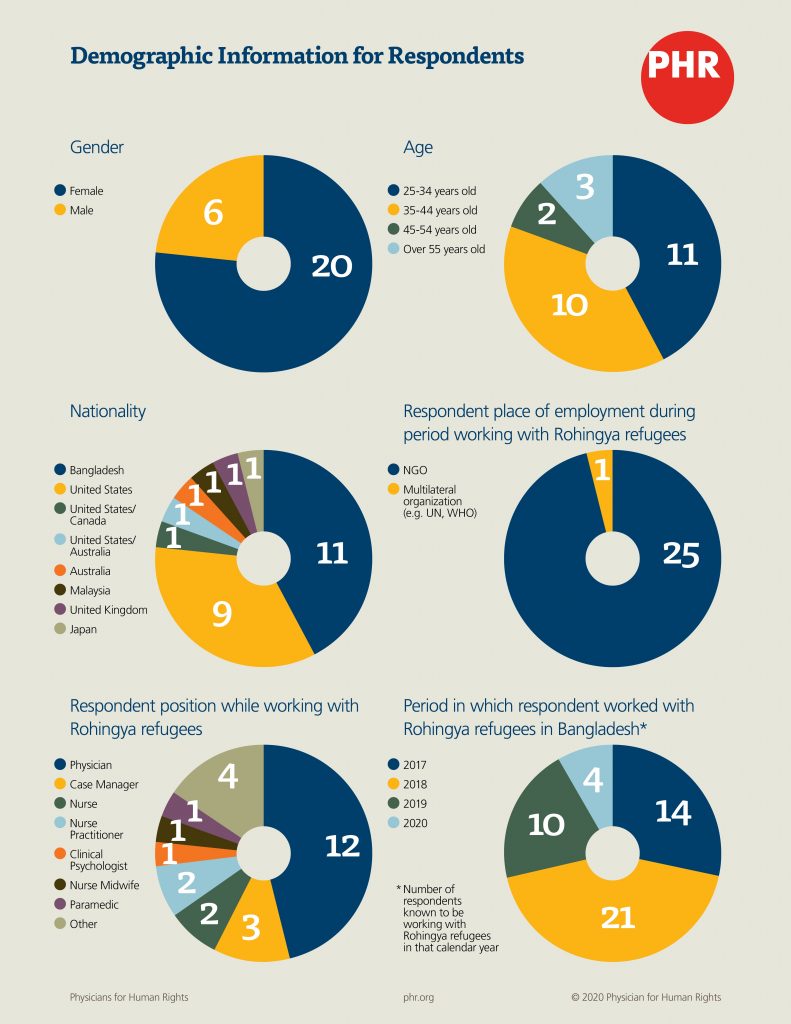
PHR interviewed 26 health care workers from a variety of disciplines who spent time in Bangladesh after August 2017 and worked closely with Rohingya refugees in a variety of health care settings. The interviews documented and explored their perceptions and understanding of patterns of injuries and conditions suffered by Rohingya refugees fleeing Myanmar who were evaluated in Bangladesh after August 2017, with a specific focus on sexual violence.
“Trauma shows up in a lot of ways for a lot of different people. Everyone there is traumatized, I would say, without a doubt.”
A physician working in Cox’s Bazar in 2017 and 2018
Sexual violence against the Rohingya in Myanmar was widespread and followed common patterns, according to accounts by these health care workers. These health professionals’ narratives help corroborate and attest to patterns of perpetration of sexual violence by members of the military and those in uniform, consistent with many other reports.[1]
In interviews conducted by PHR, health workers give further credence to the allegation that the Tatmadaw, the armed forces of Myanmar, was the primary perpetrator of widespread and systematic sexual violence against the Rohingya in Myanmar during the “clearance operations” of August 2017.
Health care workers interviewed as part of this study report that gang rape, sexual humiliation and other attacks on personal dignity, and sexual violence accompanied by other violent acts were typical experiences recalled by their patients and were reported to have been conducted by the Tatmadaw.
Health workers interviewed by PHR universally reported seeing evidence or being told of occurrences and patterns of sexual and gender-based violence committed against women, girls, men, boys, and gender fluid and transgender people by the Myanmar military. All health care workers PHR interviewed observed physical and psychological consequences of such acts against the Rohingya. They also found they were unable to adequately address the widespread and profound physical and psychological after-effects of the violence, due to barriers related to infrastructure, communication, culture, and lack of resources within the humanitarian response health care system in Bangladesh.
Health care workers shared that physical evidence of injuries consequent to rape and patient histories related to sexual violence were most often revealed during provision of care for other reasons, such as gynecological complaints or pregnancy-related care, as opposed to women seeking post-rape care services. The health workers’ recollection of the behavioral and mental health status of their patients further suggests that this sexual violence and other violations had a deep and long-lasting impact on these survivors, with high levels of trauma demonstrated years after the event. The health care workers interviewed consistently described the Rohingya as a population with vast, unmet needs for mental health support.
Finally, health care workers described multiple barriers faced by the Rohingya who fled to Bangladesh in accessing care, particularly in relation to sexual and gender-based violence and associated psychological consequences. These barriers include lack of screening protocols for physical and psychological consequences of sexual violence, limited availability of mental health care services, provider workload, patient privacy concerns, and stigma. These barriers decrease the Rohingya’s access to health services in refugee camps in Bangladesh, delay healing, and may compound the trauma they experienced as a result of the state of Myanmar’s violent campaign.
PHR recommends that meaningful efforts be made by the government of Myanmar to investigate allegations of widespread sexual violence by the Tatmadaw, prosecute those responsible, and work to provide human rights protections to the Rohingya currently living in Myanmar and any who choose to return in the future. PHR also calls on the government of Bangladesh and relevant humanitarian response actors to take all possible measures to address any barriers to care and ensure trauma-informed, survivor-centered approaches to respond to survivors’ needs. Finally, PHR recommends that the government of Myanmar and the regional and international community use all means at their disposal to support a range of justice and accountability efforts and ensure that the government of Myanmar complies with its obligations to prevent and punish the perpetration of grave human rights violations and related crimes, including sexual violence.

Background
In August 2017, the armed forces of Myanmar (Tatmadaw) unleashed a campaign of widespread and systematic violence on Rohingya communities in northern Rakhine state. The acts of 2017 were the culmination of decades of human rights violations and campaigns of violence targeting the Rohingya and other ethnic minorities. The Rohingya people, the majority of whom are Muslim, have lived for centuries in Rakhine state, on the western coast of Myanmar, a predominantly Buddhist country. In 1982, Myanmar’s military junta passed a Citizenship Law that stripped the Rohingya of citizenship; since then, they have been barred from their right to citizenship and have become stateless and subject to numerous human rights violations.[2] These have included restrictions on freedom of movement; denial of the right to health and education; forced displacement; arbitrary and illegal detentions and killings; forced labor; trafficking; and limited political participation,[3] among other violations.[4] The military government also physically constrained movement, imposed fees, and used intimidation tactics that denied Rohingya many fundamental rights, including the rights to health and education.
In October 2016 and August 2017, the Arakan Rohingya Salvation Army, a Rohingya insurgent group,[5] reportedly attacked Myanmar security forces. Following these alleged attacks, Myanmar security forces and local Buddhist civilians swiftly launched brutal “clearance operations.”[6] These counterattacks were, in the words of the 2018 United Nations (UN) Fact Finding Mission report, “immediate, brutal and grossly disproportionate,” targeting hundreds of villages and the entire Rohingya population.[7]
Ultimately, this violence drove more than 720,000 Rohingya to flee Myanmar for neighboring Bangladesh between August 25, 2017 and July 31, 2019. Most arrived in the first three months of the crisis, creating the world’s largest refugee camp near Cox’s Bazar.[8] Rohingya refugees arrived in an environment that was not prepared to accommodate them, to offer them adequate shelter and food, or to provide a health system structure equipped to meet their basic needs.[9] As Rohingya refugees were streaming over the border into Bangladesh, still raw from the physical effects and trauma of the violence committed against them, the Bangladeshi government and international organizations were racing to mobilize an emergency humanitarian response.
Research since 2017 conducted by Physicians for Human Rights (PHR), other non-governmental organizations, the media, and the UN documented serious human rights violations, including sexual violence, committed against the Rohingya population as part of the government of Myanmar’s “clearance operations.”[10] In a survey conducted by PHR and its partners, the vast majority of 604 Rohingya hamlet leaders reported violence in their hamlet, violence against civilians, and the destruction of fields, homes, and mosques.[11] The majority of respondents reported beatings, over half said people were shot, and more than a quarter reported rape or sexual assault in the hamlet.[12]
Studies documented that sexual violence was deployed as a deliberate, targeted strategy used by the Tatmadaw against the Rohingya civilian population in order to intimidate, terrorize, and punish them, and forcibly displace the Rohingya from their land.[13] These attacks were aggressive, sweeping, methodical, and perpetrated on a massive scale; the UN fact-finding mission found that the attacks “constituted crimes against humanity, war crimes, and underlying acts of genocide accompanied by inferences of genocidal intent.”[14] Rape, gang rape, sexual slavery, forced nudity, genital mutilation and other forms of violence targeting sexual organs, sexual assault, threats and attempts at rape and sexual assault, followed by the killing of victims were documented by the UN investigators, human rights and humanitarian organizations, and journalists, among others.[15] During the “clearance operations” starting in August 2017, Myanmar security forces raped and sexually assaulted women and girls as part of wider attacks on villages; there were many instances of gang rape with multiple perpetrators, or mass rape, where survivors reported that soldiers gathered them in groups and then raped or gang raped them.[16] Many victims are assumed to have been assaulted by their perpetrators to the point of death or left for dead.[17] Sexual violence against Rohingya men and boys was also documented. This violence often intersected with violence against women and girls, with men and boys forced to witness sexual violence against family or community members. Genital violence and anal rape were also reported as the common forms of sexual violence against males.[18]
Much of the extensive research and documentation of the violence experienced by Rohingya refugees while in Myanmar by PHR and other organizations has focused on collecting the experiences of individual Rohingya survivors. However, there are no studies that systematically capture the observations and perceptions of health care workers who interacted with many refugees or treated them for their injuries, both physical and psychological, from this violence. Their intimate and detailed knowledge of the health needs of Rohingya refugees who fled Myanmar uniquely positions health care workers to speak to the overall patterns of injuries and violations seen in this population and point to survivors’ ongoing needs. The documentation of this perspective also contributes to the current literature.
“Many of them seemed to be totally blank. No emotion was working on their mind. They couldn’t answer any question they were being asked. They cried continuously…. They described … so many deaths, then rapes and other fears.”
A clinical psychologist working with Rohingya refugees since 2017
Survivors’ responses to trauma are unique and a variety of factors influence their willingness to disclose details about their experience. Health care workers are generally trusted members of civil society and, seen as members of a caring profession, are often the first people to whom survivors may consider disclosing their trauma and intimate details of their experiences. For this reason, health care workers can serve as proxies for survivors. Interviewing health professionals enables the systematic collection of survivor and witness accounts, while protecting patient privacy and avoiding subjecting survivors to potentially traumatizing interviews.
PHR set out, in a methodologically rigorous way, to document and explore patterns of injuries and conditions suffered by Rohingya refugees seen in Bangladesh soon after August 2017, with a specific focus on sexual violence, via interviews with health care workers who worked with Rohingya refugees in Bangladesh between August 2017 and August 2020. We also sought to understand the barriers and facilitators to evaluating patients, documenting human rights violations, and delivering care to Rohingya survivors. The goals of this research were two-fold: first, to corroborate accounts of sexual violence reported as part of the 2017 attacks on the Rohingya with new data from health care workers, and, second, to describe the physical and mental health needs of Rohingya survivors and the availability of services to meet these needs.
Methodology
Physicians for Human Rights (PHR) conducted one-on-one semi-structured interviews with 26 health care workers, working for a variety of humanitarian organizations, who provided direct services to Rohingya refugees in Bangladesh for some period between August 2017 and August 2020. The research team included American and Bangladeshi social scientists and physicians who have experience documenting or responding to sexual and gender-based violence. Data was collected in two phases between November 2019 and August 2020. The study received institutional review board approval through Georgetown University and exemption through the PHR Ethics Review Board.
Study Population
The study was designed to explore Rohingya refugees’ experience of sexual and other forms of violence through interviews with health care workers who had worked with them in Bangladesh. Health care workers can provide narratives about individual patients based on their medical evaluations and clinical encounters. Given the number of patients seen over time by health care workers, they can also speak to the overarching patterns and trends in experiences of sexual violence and physical and psychological after-effects. Health care providers often have access to information that others do not, as people may be more open to sharing information that is more personal or private. Given known underreporting of sexual violence among the Rohingya,[19] speaking with health care workers who provided care to survivors for other health concerns allowed for collection of clinical perspectives on sexual violence that may not have been formally reported. For the purposes of this research, health care providers were defined broadly to include physicians, nurses, midwives, community health care workers, mental health and psychosocial support workers, case managers, and health volunteers. Health care workers were included if they had worked with Rohingya patients in Bangladesh any time after August 2017. Though those working in the refugee camps during the period immediately after August 2017 and into early 2018 were more likely to capture the acute effects of the violence, health care workers providing care to Rohingya survivors after 2018 were also able to share stories of survivors’ experiences of violence in Myanmar and speak to the long-term physical and mental impacts of this violence.
The study was specifically designed to capture information on sexual violence suffered by Rohingya refugees without speaking directly with survivors. PHR chose these methods to avoid subjecting survivors to potentially re-traumatizing interviews and to ensure that PHR was not contributing to repeat documentation of the same Rohingya survivors. No identifying information from the stories of individual survivors was collected.
Sampling Strategy
Respondents were identified through a chain referral sampling approach. Sampling and conduct of interviews occurred in two phases. During the first phase, members of the U.S.-based study team identified individuals and organizations engaged in work in Cox’s Bazar, Bangladesh, where the Rohingya refugee camps are located. During the second phase, Bangladeshi team members identified potential respondents currently working with the Rohingya refugees. Throughout both phases, study inclusion criteria and emergent findings were used to identify important profiles of respondents to ensure sample diversity and data responsive to the research objectives.[20] As is standard practice with qualitative research, “data saturation,” the point at which no new information or themes are observed in the data, was used to establish the final sample size to support maximizing variability and ensure sufficient data to identify themes and patterns.[21]
Data Instruments
The data collection instruments included a semi-structured interview guide and a brief demographic form to capture the health professionals’ education, employment, and work experience with the Rohingya. The interview guide covered eight key areas, including: 1) respondents’ professional background and contextual details of work with the Rohingya; 2) general experiences treating Rohingya patients; 3) knowledge of and experiences treating Rohingya patients in relation to injuries due to physical violence; 4) knowledge and experiences treating Rohingya patients in relation to sexual and gender-based violence; 5) knowledge and experiences related to the mental health status of Rohingya patients; 6) stigma and factors associated with disclosure among Rohingya regarding sexual and gender-based violence; 7) knowledge related to human trafficking of Rohingya refugees; and 8) challenges in addressing trauma and health care. While the overall topics in the interview guide remained the same throughout the project, as data was collected and analyzed, changes were incorporated into the questions and probes to ensure coverage of emergent themes.
Data Collection and Management
All interviews except one were conducted virtually using Zoom, Skype, and WhatsApp. Each interview took approximately 50 minutes. Interviews were conducted in English by two physicians and one social scientist based in the United States, and data was transcribed verbatim by a professional transcription service (Rev). Interviews conducted in Bangla were conducted by one social scientist based in Bangladesh, and data was transcribed into Bangla and then translated into English by a team of qualified transcribers and translators. Translated transcripts were reviewed by the interviewer, fluent in both English and Bangla, for accuracy of translation. Transcribed interviews were uploaded into a qualitative data management program (Dedoose).[22] Transcribed data was reviewed by team members and a coding dictionary was developed. Codes covered the research objectives (e.g., sexual violence, mental health) as well as emergent issues from the data review (e.g., patient-provider relationships).
After the completion of a first round of coding, the coders conducted a qualitative intercoder reliability assessment on a sample of transcripts, which indicated an overall consistency in the use of the codes.
Data Analysis
The research team reviewed the coded data, representing excerpted portions of the interview transcripts, to identify cogent themes and patterns and create a cohesive narrative responsive to the project’s research objectives and reflective of the data. The analytical process was iterative and employed regular team debrief sessions to further reflect upon and analyze this data.
The data analysis plan included the following steps: 1) creating documents compiling all excerpted text for each of the codes; 2) reviewing and cleaning the documents to reduce duplications due to multiple coders; 3) identifying themes and creating tables for each code word; 4) cross-referencing themes across codes to establish linkages; 5) selecting illustrative examples for each theme; and 6) developing summaries based on the data within the search documents to address the research objectives. These data analysis summaries are interpreted within the context of other data and published sources on sexual and gender-based violence among the Rohingya and the medical, legal, and social implications of the findings. Data included in this report is that which addresses the specific objectives regarding sexual violence and associated physical and psychological trauma, and availability of resources to address that trauma.
Limitations
As a qualitative study, the interpretation and analysis of data is subject to interpretation biases introduced by the researchers. The research team was multidisciplinary, drawn from a variety of cultural backgrounds, and worked collaboratively to address potential biases in the interpretation of results. As previously noted, a qualitative exercise to check for consistency in the application of codes in the data analysis phase was employed to address this potential limitation.
As study respondents were asked to recall patient histories and their experiences from events dating as far back as 2017, recall bias is inherent in the data presented. However, some of our respondents had written notes, a journal, or a blog from their time spent in Cox’s Bazar; as they were given a summary of the main research themes prior to interviews, this allowed them a chance to review prior to the interview. Some respondents did not begin treating Rohingya patients until 2018 or later; they were therefore not able to comment directly on injuries sustained in Myanmar, but could speak to the longer-term impacts, both physical and mental, of the violence experienced by their patient population.
The sample of study respondents represented a diversity of geographic and cultural backgrounds but did not include respondents who were Rohingya. Observations regarding culturally mediated behaviors must therefore be viewed as highly contextual. The survivors’ stories recounted in these interviews were communicated through multiple cultural and linguistic filters, and, often, relay conversations conducted through the help of an interpreter. Despite these limitations, there were significant similarities across the collected narratives in terms of the experiences of the Rohingya.
As with all qualitative research, our sample was relatively small and not random. Therefore, there are limitations in terms of the generalizability of this data regarding the experiences of the many health care workers and their organizations involved in the humanitarian efforts over the past three years in Cox’s Bazar.

Findings
Health care workers in Physicians for Human Rights’ (PHR) sample universally reported seeing evidence or being told of occurrences and patterns of sexual and gender-based violence committed against Rohingya women, girls, men, boys, and gender fluid and transgender people by the Myanmar military. All health care workers PHR interviewed observed some of the physical and psychological consequences of such acts against the Rohingya. Health care workers found they were unable to adequately address the widespread and profound physical and psychological after-effects, due to barriers related to infrastructure, communication, culture, and lack of resources within the humanitarian response health care system in Bangladesh.
Health care workers who treated survivors consistently described patterns of sexual violence perpetrated against the Rohingya, including gang rape and sexual violence accompanied by other violent acts such as beatings, shooting, and killing of family members.
PHR’s findings are organized into two sub-sections that capture, first, the health care workers’ accounts of Rohingya survivors’ experiences of sexual violence, focusing on the patterns of perpetration, and, second, their accounts of the interactions of Rohingya survivors with the humanitarian response system in Bangladesh.
Survivor Experiences
Sexual and Gender-Based Violence (SGBV) Experienced by the Rohingya in Myanmar
Health professionals interviewed by PHR universally shared accounts recounting widespread sexual violence against Rohingya women and girls, perpetrated by members of the Myanmar military, men in uniform, or police.
According to many of the health care workers interviewed by PHR, Rohingya women and girls articulated their histories of sexual violence during the course of clinical and other health services that were not specific to SGBV-related concerns, such as during mental health evaluations, routine gynecological care, maternal health visits, or related to vague physical symptoms encountered in primary care clinics.
“Providers were mostly focused on physical symptoms and I think they were overwhelmed…. At the clinic itself, we didn’t have the time, or we didn’t have the personnel to deal with mental health problems.”
A nurse working at a primary health clinic in Kutupalong camp in 2018
Health care workers who treated survivors consistently described patterns of sexual violence perpetrated against the Rohingya, including gang rape and sexual violence accompanied by other violent acts, such as beatings, shooting, and killing of family members.
“Most of the cases are very similar. Families killed in front of them and raped, [survivors] escaped in the bush across the border.” A nurse midwife working in Kutupalong camp in 2017
“They give some example[s] like, when the army [was] at their villages and initially they [were] trying to beat them, and if there is any female … they raped them, and after rape, they killed them.” A clinical psychologist working in Cox’s Bazar in 2018
Health care workers told PHR that their patients reported that men and women were separated during the violent attacks and that the men were killed after being separated from the women. The women, who were forced to watch the men be killed, were then raped; many of them described leaving Myanmar for Bangladesh following these violent attacks. One health professional described hearing similar stories following this pattern:
“Most of the women tell me [a] very, very similar story. When they were in Myanmar … a group of men who had uniform[s] [which] look like a police or army, something like that, came to their house and … [t]hey were raped in front of their family. After that, they took all the men…. They beat them and killed them, and they put all men into the fire and all women are taken to somewhere else in [an] empty house and they had to take off their clothes and they were naked. Men who ha[d] a kind of uniform look came to the house and they raped those women every day until they became unconscious. When those women [woke] up, [there was] fire around the house, so they tried to run away to the river which is a border to Bangladesh, and they crossed the river … to come to Bangladesh.” A nurse midwife working in Kutupalong camp in 2017
Another health professional described an almost identical tactic shared with them by patients of separating and killing the men and raping the women.
“When the Myanmar military would come to a village, they would immediately split the men and the women into two groups and they would pretty much immediately kill the men in front of the family and bury them in mass graves, and then the women would most likely be raped at that time and then either … moved to a different section or … out of that village.” A nurse working at a primary health clinic in Kutupalong camp in 2018
Multiple health care workers who spoke to PHR heard from their patients aboutwomen being confined in houses where they were repeatedly raped:
“She and, I think, around 14 other women had been taken and locked into a house, and … they were all gang raped.” A nurse practitioner working in an outpatient clinic in 2017
When asked about who committed these acts of sexual and gender-based violence, the majority of health care professionals interviewed by PHR recalled patients describing the perpetrators as members of the Myanmar military, men in uniform, or police.
“She was raped by one of the Myanmar military personnel.” An emergency room physician working in Kutupalong camp in December 2017
“It was the military … those who are associated with the army of that country.” A psychosocial support officer and case manager working in Balukhali camp since 2018
“About those who perpetrated them [the rapes], they said that [it was] a group of military people.” A clinical psychologist working with Rohingya refugees since 2017
The perpetrators were described as acting in groups and engaging in gang rapes in a systematic, organized fashion.
“Her age is between 42 to 45 years. The situation was the same, 25 militaries attacked their home at night all of a sudden. After the attack, the men of the house ran to the hill near the river, escaping through the kitchen door. After the men ran away, the woman was alone … her son was hiding in [the] poultry house. For that [her son hearing her gang rape while hiding] she is still ashamed and wishes to die. This woman is also a victim of gang-rape by three military [men]. Her physical condition was so bad that it was beyond describable in words. Her uterus was very badly damaged. It used to bleed a lot after every few days. And she had a lot of pain.” A paramedic and psychosocial support officer working in Cox’s Bazar since 2017
Many of the health care workers interviewed in this study reported learning that rape had been committed by multiple perpetrators. One health care worker discussed the case of a young girl about 12 or 13 years old.
“Six of them fled from their home together, along with many other people of their locality. Some women got separated…. Seeing an abandoned house … they took shelter in that house. There were five women in total who took shelter there, including her [the young girl’s] mother, elder sister, and aunt. Then four to five military officers attacked there. They blindfolded their eyes and tied up their hands and feet. Once they were tied up, they became victims of gang rape. After the gang rape, they decided to burn these women. Their eyes were [blind]folded…. One person’s hand was tied up with another person’s. But how this teenage girl managed to untie her hands only Allah knows that. She freed her hands. Then she removed the blindfolds off her eyes and saw that they were bringing some hay from a little away, dried hay. The military men, the military men were bringing dried hay to burn these women. She was tied to her mother. Her mother was done for a long time and she was senseless. Her mother was not moving, she couldn’t understand whether her mother was alive, so she fled away from there to a piece of land where arum [a flowering plant] was being farmed that was just beside there. She entered that arum-land and, while doing so, she said she became senseless. According to what she [said], I think that they were given something that made them senseless…. After that, when the girl crawled into that land, she was shot. The flesh on her back got teared at different parts. Then she crawled with all her energy, crossing over a lot of dead bodies, she told that she informed others of the many dead bodies lying down there through gestures. And that her mother and others with her were burnt. Her mother and others were burnt. All of them. She saw that happening…. She had no clothes on her. She said that none of them had. Then one man put off his lungi while wearing just a piece of fabric, wrapped her with that lungi. She was covered in blood. In that condition, he took her on his shoulder with much struggle, two or three days/could not recall properly … they came to the border of Bangladesh.” A paramedic and psychosocial support officer working in Cox’s Bazar since 2017
Multiple health care workers interviewed for this study reported hearing of instances where their patients were forced to witness acts of violence, including sexual violence, against family members:
“They had to leave their country all of a sudden, their houses were set on fire, their farming lands, their farming lands were set on fire, and even something like killing his brother by shooting in front of him or raping his sister in front him has also happened.” A coordinator of services for male and transgender Rohingya survivors since 2018
“To make them talk, it takes time to get started and, of course, they cry. Also, they say I want to die, or I want to commit suicide, this kind of a thing.”
A nurse midwife working in Kutupalong camp in 2017
Disclosure of Experiences of Sexual Violence
Rohingya women generally revealed a history of sexual violence incidents during provision of care for other reasons, such as gynecological complaints, as opposed to encounters for post-rape care services, according to health care workers.
“She had complaints of vaginal discharge, so I asked her if I could examine her vaginally. And then, when I did the exam, it looked like she had some trauma, just from the scars on her perineum. So, I asked her a few questions about that, and then she started crying and talked to me about her experience of rape at the hands of the military, the Myanmar military.” A nurse practitioner working at an outpatient clinic in Kutupalong camp in 2017
Health care providers also described patients sharing experiences of sexual violence only after being asked directly during the medical intake.
“Because I knew that there was a history of sexual violence among the population, I was alert to the possibility of that. And then I asked … if she had had any problems with the military, or with anybody, when she was leaving Myanmar. And she hesitated a minute and then she started crying and said that she and I think around 14 other women had been taken and locked into a house, and that they were all gang raped. And some of them did not survive, but she was able to survive. She was now 40 years old.” A nurse practitioner working at an outpatient clinic in Kutupalong camp in 2017
Many of the health care workers learned of their patients’ experiences of sexual violence while the women were receiving pregnancy-related care. Respondents recalled seeing higher numbers of pregnant women during months that corresponded to the patients having conceived during the period of violence inflicted on the villages in Myanmar, in and around August 2017.
“Of course, they had no way to check if they are pregnant or not and by the time they notice, it’s already 20 weeks and that was a time they come to the clinic. That was in November, because the crisis happened the end of August and most of the incidents happened the end of August up to beginning of September.” A nurse midwife working in Kutupalong camp in 2017
One health care worker noted an increase in births in the spring of 2018, which they perceived as correlated with conception having occurred during the events leading up to and during the August 2017 violence.
“It was … nine months after August of 2017. So, there was a huge increase in the births because of all the women who were raped.” A physician working in Kutupalong camp in 2018
These estimations of increased pregnancy and birth rates are consistent with published studies and observations by other organizations[23] suggesting rates above the historical baseline among Rohingya refugees fleeing to Bangladesh.[24]
A few health professionals stated that they suspected that many children seen in their clinics were born of rape.
“The second time I went back [to the camps] in July [2018], that would have been … 11 months [after the violence], so many of the babies that were products of rape had been born. It was untalked about. Nobody said anything and the babies would be brought in…. They’d be accepted into the community, into the family. Obviously, the mom was there, but there was no discussion of how that baby came into being.” A pediatrician working in Cox’s Bazar in 2017 and 2018
Some health care workers were specialists in women’s health who managed sexual and reproductive health, and who described women asking to terminate their pregnancies (reportedly related to rape prior to arrival in Bangladesh).
“They were interested in this [abortion]. They were interested because everyone in the family knew that she was unmarried. Moreover, she couldn’t tolerate the fact that she was going to be the mother of a child [born of rape].” A paramedic and psychosocial support officer working in Cox’s Bazar since 2017
A health care worker described how difficult it was for survivors to both grapple with their unwanted pregnancy and contemplate asking for a termination of their pregnancy, given cultural and religious norms and legal restrictions on abortion in Bangladesh.[25]
“The midwife came and said, ‘Madam, a patient … has come, she wants [to have a] miscarriage, which means she does not want to keep the baby anymore … she … [wants to] have an abortion…. What can I say?…. When I started talking to that woman, she would burst into tears…. After asking her some questions deeply, like, ‘Why do you want to ruin the baby?’ She was told the Islamic thing that it is a great sin to ruin a baby. Then we would see that many became [emotional] and one or two [women were] saying that ‘I have a child; it is not mine and I … I was not even married. I don’t want to keep this baby.’” A clinical supervisor and health post manager in Balukhali camp since 2018
Despite the legal restrictions on abortion in Bangladesh, the accepted family planning strategy of menstrual regulation to “regulate the menstrual cycle when menstruation is absent for a short duration” is allowed up to 12 weeks after a women’s last menstrual cycle.[26] This approach provided an avenue for humanitarian organizations in Cox’s Bazar to offer comprehensive reproductive health options for Rohingya survivors.[27] A few clinicians told PHR that women also used informal or traditional abortion practices to attempt a self-induced abortion. When these attempts led to complications, they would present to clinics for care.
“[They had had] failed attempted terminations when they came.… [The staff] would call me because the patients were very unwell. At that point, obviously, we didn’t really discuss what had happened in terms of whether they were, who was responsible for that. We didn’t know, but we definitely saw a significant number of termination[s] … self-induced terminations of pregnancy when we were there”. A physician working with Rohingya refugees in 2017 and 2018
Sexual Violence Experienced by Non-Female Patients
The perpetration of sexual violence was not limited to women and girls. Health workers also shared stories of providing care to non-female-identified patients – including men and boys and gender fluid and transgender individuals – who were survivors of sexual violence in Myanmar, though they were often very reluctant to share details.
“We have found … adults and young boys, they also became victims of physical violence…. There are one or two who had become victims of sexual violence, there are one or two like this.” A clinical psychologist working with Rohingya refugees since 2017
Accounts of these experiences included narratives of direct sexual violence, as well as instances of being forced to witness the rape or sexual assault of family members and extortion and duress related to their sexual orientation or gender identity.
“Those who became victims among the gender diverse population [gender fluid, transgender], they became such victims even [in Myanmar] …They were victims of different type[s] of teasing, they were victims of different types of harassment. But what they feared … the most [in Myanmar] was that they … [would be] killed…. Those groups [Rohingya “thugs” in Bangladesh] used these people [coerced the gender fluid or transgender person into sexual acts] [by threatening] to rape the sisters…[or] to rape his mother.” A coordinator of services for male and transgender Rohingya survivors since 2018
Mental Health Status of Survivors
Many of the women who had been raped exhibited signs of mental health conditions such as depression and post-traumatic stress disorder (PTSD), according to the health workers who treated them.
“We … found that most of them [the refugees] were suffering from PTSD. They had full-blown symptoms. We noticed that … [they] even didn’t feel comfortable in talking to us. We were taking care of them, but they couldn’t manage to trust us completely…. At that time, there were some symptoms in them like their response, anxiety, hastiness, I mean very unstable, and some were in depression, like they were depressed and were not talking at all…. And it was like they came through such a crisis, many of them seemed to be totally blank. No emotion was working on their mind. They couldn’t answer any question they were being asked. They cried continuously. Upon being asked about anything, the first answers they gave were about what they had seen there. How they have come here. They described the difficulties of the situation, how much they had to walk, so many deaths, then rapes and other fears. That they were scared, these things were very common in them.” A clinical psychologist working with Rohingya refugees since 2017
“To make them talk, it takes time to get started and, of course, they cry. Also, they say I want to die, or I want to commit suicide, this kind of a thing.” A nurse midwife working in Kutupalong camp in 2017
While some health care workers found that patients were able to verbalize their traumatic experiences and encouraged this, others found that patients were reluctant to express their feelings and share their experiences, displaying passivity during their treatment and remaining silent and motionless. Health professionals drew parallels between the trauma they witnessed in Rohingya populations and the trauma they saw in other victims of abuse.
“Most of the stories of trauma came from the patient’s mouth, like, ‘This is what happened to me,’ not necessarily ‘This is an injury, here are the scars.’ They said the trauma stories. I tried to have them express it as often as I could because my philosophy [is that for] patients who have gone through this, it’s part of the healing. We might be the only person that they might be able to narrate this story to. Whenever I had the opportunity or if I wasn’t as busy, I would try in a mindful way, just kind of ask the patient if they would be willing to share what happened…. I’m not a psychologist, I’m not a clinical psychiatrist, but I felt like I had to act like one for a lot of the patients because they’re coming in with vague symptoms like … muscle aches or stomach pain. That’s sometimes somatization of trauma. That was an often thing that we saw as well.” A volunteer physician working in Cox’s Bazar in 2018
One clinician described their patient:
“I found her absent-minded. She didn’t look at me, didn’t talk, and only kept on crying. I observed different kind(s) of abnormal behavior.” A paramedic and psychosocial support officer working in Cox’s Bazar since 2017
Psychosomatic complaints were very common, and with further probing, were presumed to stem from trauma.
“A huge number of our patients had somatic complaints, like very vague. Like, ‘I’ve had a headache or a stomachache or backache.’ And then, when you dig deeper into how long have these things been going on, it’s been going on as long as they left their home or as long as they’ve been living in the camps. So, we certainly saw a lot of patients who we couldn’t find anything wrong with them clinically and it seemed like the providers would attribute it to just a stress reaction that’s manifested in a physical way. And that was very, very common.” An emergency nurse working in satellite health clinics in December 2017
“We try to identify the causes in medical science like blood loss or nutritional deficiency, it could be seen that those were not found. But … [if] she is feeling weak … or cannot concentrate in anything, then we would assume that it was a psychosomatic disorder and of course it was a mental disorder and surely they were suffering from some mental problem.” A clinical supervisor and health post manager in Balukhali camp since 2018
Continued Experiences of Sexual Violence
Sexual violence experienced by many of the female refugees did not stop at the Myanmar-Bangladesh border. Once the refugees were settled in Cox’s Bazar, health care providers began to hear stories about and see evidence of intimate partner violence (IPV) perpetrated by Rohingya men. These incidents were attributed to the trauma of violence experienced in Myanmar and stress related to life in refugee camps. Multiple health care workers interviewed for this study described regularly seeing injuries resulting from IPV. This represents an ongoing source of violence and trauma for Rohingya survivors.
“Trauma shows up in a lot of ways for a lot of different people. Everyone there is traumatized, I would say, without a doubt. So, men taking that out on their wives is definitely something that we saw for sure.” A physician working in Cox’s Bazar in 2017 and 2018
“Hitting, punching, kicking on any part of the body, including the head, and even if you’re pregnant it could still be the abdomen…. We’ve had women whose husbands have tried to hang them, whose husbands have tried to poison them, who have been burned.” A nurse practitioner working at an outpatient clinic in Kutupalong camp in 2017
Survivors’ Interaction with the Humanitarian System in Bangladesh
“What you realize is, as a doctor, you feel like everyone’s going to present to health care immediately, but there’s so many conflicting priorities for people in that setting that they have to try and deal with because they basically often have nothing.” A physician working with Rohingya refugees in 2017 and 2018
During the early days of the Rohingya influx into Bangladesh in late 2017 and early 2018, refugees had very limited access to health resources, as the existing infrastructure was inadequate to handle the arrival of such a large number of people. As refugees began arriving in Cox’s Bazar, the response was coordinated by the government of Bangladesh, through the Refugee Relief and Repatriation Commission, the UN High Commission for Refugees (UNHCR), and the International Organization for Migration. While the Cox’s Bazar region was already home to displaced Rohingya refugees, the influx starting in August 2017 quadrupled this population in the span of two months, putting an enormous strain on the environment and existing infrastructure.[28] At that time, lifesaving care and the provision of basic necessities, food, water, clothing, housing, and sanitation were prioritized. Mental health and non-acute physical health problems were often deprioritized and left unattended. The health system also had to handle outbreaks of infectious diseases, such as diphtheria and measles. As a result, the Rohingya’s extensive health needs resulting from the violence – including sexual violence – experienced in their home villages in Myanmar and during the long journey to Bangladesh were not addressed immediately.
As the crisis evolved, international agencies and NGOs arrived in the camps to set up health centers, health clinics, and community-based services for the Rohingya, with different mandates and specializations. Often, these health posts were staffed with a mix of Bangladeshi and international health care professionals serving in long-term and short-term positions, some of which were volunteer response positions.
Respondents reported that, in the beginning of the crisis, there was little coordination between the various humanitarian assistance groups, resulting in overlap in some services, inadequate care for certain groups (e.g., pregnant women), and a haphazard referral system. Over time, organizations started coordinating a response to the crisis using the cluster approach, where organizations are grouped by sector to reduce overlaps and gaps in service.[29] The health sector was coordinated jointly by the government of Bangladesh, through the Civil Surgeon’s Office of Cox’s Bazar District and the World Health Organization.[30] Through this approach, a health infrastructure developed to support standardization and quality improvement and extension of needed social support to survivors.
An ongoing barrier to Rohingya survivors is that Bangladesh has not granted the Rohingya official documentation and legal status as refugees. Without this status, Rohingya survivors do not have the rights that it would afford and face denial of freedom of movement and access to public services, which, in turn, prevents them from accessing essential basic legal protections and services for survivors of sexual violence.[31]
“One of the other challenges … was the Rohingya not having refugee status and … if we ever needed to transport them to a higher level of care, actually being able to transport them past a certain [geographic] point to other hospitals was difficult.” A physician at a Balukhali inpatient department in 2017 and 2018
However, in addition to challenges that Rohingya survivors faced to access services because of the chaotic care environment, they also faced key barriers to reporting human rights violations due to a variety of cultural and systemic issues outlined below. As demonstrated in the survivor stories above, these barriers did not prohibit survivors from sharing their experiences, but, without special consideration to these challenges, the burden fell on survivors to navigate a care environment that was not well suited to their needs.
Stigma
Social stigma and fear that they would be rejected or blamed by their own families and communities hindered some survivors from disclosing their experiences of rape or sexual assault. Female survivors were reluctant to discuss and disclose sexual and gender-based violence that occurred in Myanmar out of fear they would not be able to get married or would be rejected by their husband.
“So, one evening, my midwife came with one nine-months pregnant lady and they were saying that she never had any antenatal checkup. I was wondering why and after a while we … [learned] that she was raped nine months ago and just because it’s a matter of shame to disclose it within their community, or to come to the facility here. They kept her inside the house; she didn’t receive any antenatal checkup or anything.” A medical officer working at a health post in Camp 17 since 2018
“It’s like they didn’t even talk about it [rape] among themselves, and they didn’t want to know, because of the fear of ramifications. And they probably felt so helpless, too. So, it sounds like even among the family groups, they really didn’t talk about what happened when those raids would happen.” A nurse practitioner working at an outpatient clinic in Kutupalong camp in 2017
In many cases, as demonstrated in the survivor stories shared above, survivors chose to disclose their experiences to health care workers, whom they trusted. However, stigma around sexual and gender-based violence was so great that one health care worker shared that, at times, they felt unsafe reporting pregnancies resulting from rape, for fear of retaliation from the survivor’s family and community members.
“I was afraid myself, because they were staring at me and still, I can remember, they were saying that something happened [related to] satanic belief, like … [some] really bad thing happened to her.… They were asking me, ‘Is it abdominal tumor or not?’ Although I was 100 percent sure this is a case of pregnancy, but as I lived really close to [the] Rohingya community within a tent, a single doctor, no other support, I had to write it as abdominal tumor with a query mark…. Still, I can remember the case because it was not an abdominal tumor, but I wrote it just because of my own safety.” A medical officer at a health post in Camp 17 in 2018

Challenges with Communication and Rapport Building
Respondents shared that they felt that a long history of denial of health care, negligence, and abuse in Myanmar made the Rohingya reluctant to seek care in Bangladesh and made it difficult for Rohingya patients to speak openly with health professionals.[32]
“They haven’t ever seen a provider in Myanmar. We were the first clinician they’ve ever seen in their lifetime…. There [were] definitely many, many cases where it was clear that this was absolute neglect of having access to health care. I would say pretty much every patient we saw, we were the first clinician they had ever seen in their lifetime, even the elderly patients.” A volunteer physician working in Cox’s Bazar in 2018
Rohingya were perceived by respondents to be “private people.” They would come to health centers to see a doctor for treatment but would remain silent and reluctant to discuss their problems or what had happened to them in Myanmar.
“When they come to the doctor, [they feel] they are to state why they are there, and they are not there to have a social conversation about their problems. So, they barely go into any details about anything that they have suffered unless people really sit down and ask about it.” An emergency room physician working in Cox’s Bazar in December 2017
Some respondents noted that this privacy and reluctance to share may come from the dehumanization and violations experienced in Myanmar.
“I sensed that a lot of them felt like they were treated their entire life as though they weren’t even a human being.” A volunteer physician working in Cox’s Bazar in 2018
Respondents noted that active listening, comforting with physical touch, body language, and showing care worked as strategies to treat physical illness and develop trust.
Importantly, none of the study respondents were Rohingya health care workers. As a result, observations regarding “openness” to discuss personal issues and other culturally mediated behaviors are highly contextual and viewed through an outsider’s lens.
Building rapport with the Rohingya was a challenge for health care workers across specialties and countries of origin. A lack of direct communication, the use of a translator, absence of Rohingya health workers or support staff, and cultural barriers made it difficult to understand Rohingya patients’ actions and motivations.
“I think their culture is so different that it was very hard to understand what they were thinking or feeling. It seemed like they were scared. Anything you tell them, they will say, ‘Yes, yes, yes.’ – they wouldn’t ask any questions. And to me, that’s a pretty bad sign because they do not understand anything that you’re saying. And then, no matter what you said, whether it’s right or wrong, they wouldn’t ask for clarification or ever say that they didn’t understand.” A volunteer physician working with Rohingya refugees in January 2018

Gender sensitivities
Sensitivities around the interactions between males and females and expectations of modesty provided an additional cultural barrier to the provision of care. Female patients were resistant to any kind of physical examination and categorically disallowed male providers to conduct these.
“I’m a western man, western white man speaking with a Rohingya woman patient and even if there was just kind of a simple gynecological complaint, many Rohingya women would prefer just to continue with their complaint than allowing a strange man to examine them, even with another woman in the room.” An outpatient attending physician in Kutupalong camp in 2018 and 2019
According to the health professionals, when working with male translators, special steps had to be taken to make female patients feel comfortable providing information.
“When we did exams, he would step behind the curtain and translate from behind the curtain.” A physician working in Kutupalong camp in 2018
If the gender dynamics in the exam room were not culturally appropriate, the patient might not disclose important information or deliver a complete history that would help in assuring the necessary treatment. Respondents shared stories where the workload and staffing at health centers did not make it possible to observe cultural best practices (e.g. having a female physician and female translator for female patients). In these cases, some health care providers felt that they were not able to deliver culturally competent care. When the patient, translator, and doctor were of the same sex, they would be most comfortable in relaying information between them and the chances of getting the right information from the patients was far higher.
“We have hired two female Bangladeshi translators who translate for the female providers, and they do a very good job of that. People seem to feel comfortable with them and to really confide in them. But if I have to use a male translator … then it’s often happened that people will come back later and tell me ‘I had this problem at that time, but I didn’t tell you because you had a male translator.’” A nurse practitioner working at an outpatient clinic in Kutupalong camp in 2017
Some health care workers reported that conducting clinical encounters through interpreters from the Rohingya community made provision of care easier, as they had someone to help provide culturally appropriate care and, in some cases, patients were able to be more open with translators than with providers. Some health care workers described their translators as a key partner in the exam room, able to skillfully navigate the discussion of challenging topics with Rohingya survivors.
“Part of what was so amazing about him was that it did feel like he was able to get women to open up. To me, being able to tell somebody that they were suicidal is a huge trust. He built rapport with them and was able to really help them figure out…. They did a lot of talking.” A physician working in Kutupalong camp in 2018
Some health care workers, on the other hand, shared that working through interpreters actually made provision of care to survivors more challenging in terms of addressing stigma and building rapport. They also shared that a lack of detailed medical terminology in the Rohingya language was a major challenge. Most of the time, they would use translators to understand the specifics of the health problems, but not all the interpreters were familiar with the Rohingya cultural context, as they were not Rohingya themselves, but local Bangladeshis.
“I think that was made worse by the fact that the dialect that our interpreters had, which was like a Bangladeshi dialect, … wasn’t exactly the same as the Rohingya language. So, there was maybe some language barrier there, too … because sometimes from their tone I couldn’t tell if they were necessarily being sensitive in the way that they were asking questions or the answers that they were giving.” A volunteer physician working with Rohingya refugees in January 2018
Translators were also often not trained in medical interpretation. Health professionals shared that they sometimes felt the interpreters were summarizing rather than translating the whole story told by the Rohingya patient, a frequent issue when conducting interviews and obtaining medical information through translation. They hypothesized that this might be because of limited skills in translating verbatim, lack of training or awareness of medical terminology, fear of secondary trauma for themselves, or the hospital/health center being too busy and time with patients being limited, increasing pressure to summarize.
Provider workload
One frequently discussed impediment to providing care for survivors was the health care providers’ workload, many referrals, long wait times for patients, and limited time allotment to evaluate patient needs. The pressure of provider workload made it particularly difficult to provide trauma-informed care to survivors of sexual violence.
“When people would call, and I would answer my phone sometimes like 30 to 60 times an hour of people referring patients. I was just unable to…. We just have such a large number of [patients]. It was very challenging for us.” A physician working with Rohingya refugees in 2017 and 2018
“Sometimes we have to see 80, 90 patients, one person, one doctor, and it’s so difficult for one doctor to see 80 plus patients. It’s very challenging for us.” A medical officer working in the Rohingya response since February 2018
Respondents reported that hundreds of patients would be lined up to receive services even before the clinic opened. Respondents noted that addressing trauma within the short visits was not feasible.
“They would start lining up, I don’t know, three, four in the morning. We’d get there … there’d be 300 of them.… I don’t think that there was a lot of care. There was no ob/gyn care at all. There was no mental health care other than [organization redacted].” A pediatrician working in Cox’s Bazar in 2017 and 2018
Privacy Concerns
Respondents also discussed the physical structure of the clinics, which made it difficult to ensure privacy and adequate time for patients to discuss trauma.
“Our clinic was like bamboo, like thin bamboo walls…. There was really limited privacy overall.” A nurse working at a primary health clinic in Kutupalong camp in 2018
Health professionals stated that the lack of privacy and inadequate resources to maintain confidentiality during counseling held the patients back from opening up about their experiences.
“We tried to provide the counseling, and for the counseling we need ideal setups. So, sometimes it is very tough when we try to make confidentiality and rapport building, and sometimes there is … [a] secret issue. Lots of noises over there, so clients sometimes feel discomfort to give enough information. Sometimes … [beside] the room, there is another room, they are talking and working and even they are laughing sometimes.” A clinical psychologist working in Cox’s Bazar in 2018
Barriers to effective referral systems
Initially, there was a lack of coordination among the health services and clear referral pathways were not in place. Over time, as partners became more aware of each other and the camp-level coordination system was more established, a clearer system for referral was developed. For sexual violence survivors, respondents shared that they had to take an active role in the referral process, both by contacting organizations in advance to confirm availability and share patient information confidentially, and to follow up to ensure that the patient was seen. PHR noted uneven referral pathways and different referral systems used by different providers.
“We sent her to Cox’s Bazar, explained the situation to the doctor over the phone. So, they, too, maintained the confidentiality of the matter. I arranged for that so that my patient could get the better treatment, the right treatment. I kept a record of that in the register over there.” A paramedic and psychosocial support officer working in Cox’s Bazar since 2017
“There was a lot of network problems some days ago and phones could hardly be reached. During that time, we found it hard to refer.… Before referring, … I need to confirm that the concerned person is available there. Otherwise, the survivor would take the trouble of going there and coming back without any result. In fact, we telephone our relevant focal person, GBV [gender-based violence] focal or legal assistant, and we check if they are available and only then send the survivor.” A psychosocial support officer and case manager working in Balukhalicamp since 2018
“We are closely involved with the protection sector of those concerned camps. If we need referral for any case, if we need to provide treatment beyond our authority, then we send the person to the concerned sector of the concerned camp by maintaining a referral slip.” A coordinator of services for male and transgender Rohingya survivors since 2018
Respondents noted that the government of Bangladesh played a key role in the referral system, as the camp in charge (CIC) – the government’s administrative head of each refugee camp – supports referral systems and has to approve patient movement outside of the camp, which is especially critical for survivors seeking psychological support that is not available in the camp.
“One of the main objectives of the camp orientation meetings was to encourage support between one service provider and another. The CICs used to play an important role in this. When we would find that we are not getting any result after referring, we used to tell the CIC and [they] would then take effective action.” A GBV case management officer working in camps in Teknaf and Ukhia since March 2018
Inconsistent Screening Protocols
The availability and use of screening protocols for both physical and psychological conditions varied over time and between institutions. Workload and inexperience of some of the health care providers affected consistent use of screening protocols.
“I think that the screening that we did was probably poor and I think the amount of people we were seeing per day was so high, I think people just didn’t have maybe the right training or we just had too many patients and I don’t think that we were equipped to deal with it. We certainly did not do any screening like in our triage area, that’s for sure, that was where the nurses were, they were just doing blood pressure, vital signs…. I think that providers were mostly focused on physical symptoms and I think they were overwhelmed, and I think they didn’t know what resources even existed or they assume that no resources existed. At the clinic itself, we didn’t have the time, or we didn’t have the personnel to deal with mental health problems. And I think it was unclear at the time exactly what resources existed. I know at the time, there was one, I believe there was one like psychiatrist for the entire Kutupalong camp –so I was told — for 700,000 people.” A nurse working at a primary health clinic in Kutupalong camp in 2018
The screening protocols that were used often focused on general mental health screening, using tools commonly employed in clinical settings in the “global north,” written and validated in English and not necessarily in local languages and cultural contexts. Screening protocols or instruments targeted specifically to sexual violence were rarely, if ever used, for a variety of reasons.
“Were there any protocols to screen every female, or every female coming in with some gynecological issues or mental health issues? No, there were no protocols for that…. So, for me personally, it was just if somebody came in with gynecological complaints, and then, when I examined them, if it seemed at all like it could be more than vaginal candida, a yeast infection, then I would often ask them if they had had any history … if they had any trouble with sexual violence in the past. I was not doing a routine screening.” A nurse practitioner working at an outpatient clinic in Kutupalong camp in 2017
“If I did suspect [some] kind of depression, I just went through SIG-E-CAPS.[33] I wouldn’t use anything like PHQ9,[34] nor would I use the PTSD questionnaire. Just because I think especially with the PTSD questionnaire … it’s like 20 questions and all that just needs to be translated. And sometimes, too, there were a lot of difficult translation issues because our translators were not medical translators. They knew English because they had studied. They were Rohingya that somehow in Burma managed to study chemistry or law or some other field. And so oftentimes they just didn’t really know the English word for a lot of things, medical things, concepts and whatnot.” An outpatient attending physician in Kutupalong camp in 2018 and 2019
“Sometimes, I think in the psychological point of view, language is a very challenging barrier, and also there is no standard based tools, psychological tools. Which tools we use … in Myanmar refugee[s], and which skills are used in [a] Malaysian[35] context. We try to use that, but those for the refugee context, they don’t have any standardized tools.” A clinical psychologist working in Cox’s Bazar in 2018
Limited mental health services
Despite the need for mental health experts and resources, there were limited programs available within the camps and an inadequate number of health care workers with a background or training in mental health care. Many respondents shared that they were reluctant to approach patients about their experiences in Myanmar. This reluctance was a result of both fears of retraumatizing patients and inadequate referral resources for those who were experiencing psychological trauma.
“I didn’t have the resources I needed to be able to go into that with people. I didn’t have any mental health backup, so it didn’t feel appropriate to go into it. That felt more like it would have been for my curiosity and not for their therapeutic treatment. If I had had mental health treatment there, 100 percent [I] would have asked everybody, but I just didn’t.” A physician working in Kutupalong camp in 2018
With limited personnel trained in mental health services, there were also concerns about follow up with patients and knowing whether they were getting the help that they needed.
“If anyone needs that, a specialized GBV service like … legal [services], or they need protection, we try to refer [the patient elsewhere], and it sometimes works. And sometimes it is also the problem like, if a client comes to us, [and] … she needs the psychological services, we are providing one or two sessions. When they go to another organization, and solv[e] … that problem, they’re not returning to us [for] … follow-up…. So, sometime … we don’t know what is the condition of [those] … cases. This is the problem.” A clinical psychologist working in Cox’s Bazar in 2018
“I think just, well what are we going to do now with this information? Because United States Preventive Services Task Force,[36] they just say only screen for depression if there are resources available to treat it. And I think especially in the first maybe six to eight months of the crisis, there still wasn’t a lot in the way of mental health or psychosocial support.” An outpatient attending physician in Kutupalong camp in 2018 and 2019
After the initial influx of Rohingya refugees, as the mental health needs of survivors became clearer, local organizations and international NGOs recognized the need for mental health services, including specialized services for sexual and gender-based violence. In some cases, they were able to introduce these services, but these services were not widely available or easily accessible for all survivors.
“At the time I was there, [organization redacted] was accepting referrals for women who had faced gender-based violence with the rape cases. Any time there was a suspected case of gender-based violence, we would send the patients to that program. It would be like a written referral and our staff would explain to the patient where they’re located within the town. As far as counseling services, at that time there was, I would say, next to nothing, except for those cases of severe gender-based violence.” A volunteer physician working in Cox’s Bazar in 2018
“Mental health services are just so much in need. One of the times I was there, I was lucky. We had a dual trained internist and psychiatrist…. She did a group [therapy] visit one day, which was organized by the Rohingya. The women didn’t want to talk initially, … [but] by the end of the group visit, they were hugging, and they were hugging her, they were smiling. This was maybe a 30-minute, 45-minute session. Just to see that healing within one session…. I think the most effective thing besides treating some of the medical issues was actually just being a set of ears listening to them, validating that they’re human…. Just something simple like touching them and validating that they are human, looking at them in their eyes and making that connection, I felt that was more powerful than the antibiotics and the nebulizer treatment that I was giving them.” A volunteer physician working in Cox’s Bazar in 2018
Health care workers shared that men, boys, and transgender people were less likely than women to disclose their experiences and limited services for this population further marginalized them. Services for sexual violence survivors were often concentrated on women and girls and often offered in “women-friendly spaces” where men, boys, and transgender people would not be welcomed. Organizations providing services responsive to the specific needs of men, boys, and transgender people were less numerous and often spread thin in order to be able to provide services and case management across many camps.
“We are trying to provide them at least with their primary demand that is … the required treatment, so that he remains free from the risk of getting HIV, so that he doesn’t have to come for other diseases.… We are trying to keep him healthy … through our own health services and … the other service centers, or the services provided by the like-minded NGOs.… They cannot share their sexual treatments with any other places because of their identity.… They fear of having their identity disclosed. So, after we came here, at least they found this support that they can share their feelings with the counselors we have here … the ones at the community level here.” A coordinator of services for male and transgender Rohingya survivors since 2018
Conclusion

Sexual violence against the Rohingya in Myanmar was widespread and followed common patterns, according to accounts by health care workers who cared for Rohingya refugees who fled to Bangladesh following the violence in Myanmar in 2017.
These health professionals’ narratives help corroborate and attest to patterns of perpetration of sexual violence by members of the Myanmar military and those in uniform, consistent with many other reports.[37]
In interviews conducted by Physicians for Human Rights (PHR), health care providers give further credence to the allegation that the Tatmadaw, the armed forces of Myanmar, was the primary perpetrator of widespread and systematic sexual violence against the Rohingya in Myanmar during the “clearance operations” in August 2017.
Health care workers interviewed as part of PHR’s study report that gang rape, sexual humiliation and other attacks on personal dignity, and sexual violence accompanied by other violent acts were typical experiences recalled by their patients.
Sexual and gender-based violence was perpetrated not only against women and girls, but also against men, boys, and gender-fluid and transgender people.
Health workers reported learning about a multitude of atrocities and violations that included killings, rape, violence against both the victim and their family, beatings, destruction of property, burning of homes and fields, and murder. Additionally, health care workers interviewed in this study reported hearing accounts of survivors being forced to witness the rape or sexual assault of family or community members as a tactic the Tatmadaw employed to perpetrate violence, intimidate, and forcibly displace the Rohingya from their land.
Some health workers noted higher than expected rates of births in the spring of 2018 and attributed them to pregnancies conceived as a result of rapes that occurred in Myanmar in the summer of 2017. Many women, they noted, sought to end these pregnancies with the help of health professionals or independently.
Sexual violence had a deep and longlasting impact on the mental health of Rohingya survivors. Health care workers consistently described the Rohingya as a population with vast, as yet unmet needs for mental health support.
Health professional accounts also demonstrate that survivors of sexual violence did not often report their experiences and faced strong cultural pressure and stigma to remain silent. This was particularly true for survivors who were not female identified: men, boys, gender fluid, and transgender. Because of this stigma, many survivors were identified only when they sought health care for other reasons, including for gynecological complaints and unwanted pregnancies resulting from or presumed to have resulted from rape. This points to a high likelihood for an underestimation of the true number of those affected by sexual and gender-based violence (SGBV), and, as a result, to a potentially large number of survivors of sexual violence who have not sought care and have an unmet need for post-rape and post-violence services.
Sexual violence had a deep and long-lasting impact on the mental health of Rohingya survivors treated by health care workers in this study. Health care workers consistently described the Rohingya as a population with vast, as yet unmet needs for mental health support.
The refugee experiences recounted by health care workers indicate repeated trauma experienced by Rohingya survivors: from the initial act of sexual violence in Myanmar, through their flight to Bangladesh, to their lack of access to appropriate medical care or psychosocial and mental health support upon arrival in Bangladesh. Additionally, survivors experienced ongoing traumatization due to continued SGBV (largely due to intimate partner violence) in the camps and ongoing unmet mental health needs.
In addition, the health care workers described multiple barriers faced by Rohingya in relation to seeking health care, particularly in relation to SGBV and associated psychological consequences. These barriers include limited availability of mental health care services, lack of screening protocols for physical and psychological conditions, provider workload, communication challenges, patient privacy concerns, and stigma. These barriers not only decrease the Rohingya’s access to health services but compound the trauma they experienced as a result of the state of Myanmar’s violent “clearance operations”.
Justice and Accountability
The narratives of health professionals who had an intimate lens into the Rohingya experience underscore the impact of sexual and gender-based violence on all aspects of Rohingya survivors’ lives – their security, physical and mental health and well-being, and economic, political, and social status, among other areas — as well as the enduring consequences of sexual violence for Rohingya communities. Survivors’ experiences are further compounded by the stigma associated with sexual violence and increased vulnerability as a result of displacement, with limited opportunities for rehabilitation or redress to date. The observations of health workers also shed light on the lack of access to appropriate medical care or psychosocial and mental health support upon the Rohingya’s arrival in Bangladesh and survivors’ limited choices about their reproductive health. Meanwhile, the protracted nature of the violations documented by Physicians for Human Rights (PHR) and other organizations suggest that forced repatriation of the Rohingya to Myanmar may lead to further atrocities.[38] [39]
As a preliminary matter, justice for the Rohingya will require recognition of the basic rights to which they are entitled under international law, regardless of their legal status.[40] [41] The state of Myanmar must honor its obligations derived from international human rights law, customary international law, and international humanitarian law.[42] [43] Accordingly, Myanmar not only has a duty to respect, protect, and fulfill the basic rights of all Rohingya currently living in Myanmar and those who choose to return in the future, but to do so without discrimination. [44] [45] Myanmar’s human rights obligations also give rise to its duties to investigate and prosecute violations of international human rights and international humanitarian law committed against the Rohingya and to provide survivors access to effective remedies.[46] The state of Bangladesh is also obligated to adopt all possible measures to address any barriers to care and to the Rohingya’s needs.[47] This includes investigating and prosecuting intimate partner violence and other forms of sexual violence committed against the Rohingya while in Bangladesh.
“ I asked … if she had had any problems with the military, or with anybody, when she was leaving Myanmar. And she hesitated a minute and then she started crying and said that she and I think around 14 other women had been taken and locked into a house, and that they were all gang raped. And some of them did not survive, but she was able to survive.”
A nurse practitioner working at an outpatient clinic in Kutupalong camp in 2017
Myanmar is further bound by non-derogable peremptory norms of general international law (jus cogens[48]) which prohibit, among other things (inter alia), acts such as genocide, crimes against humanity, and torture.[49] Since judicial authorities have long held that sexual violence may serve as the basis for these acts,[50] the state of Myanmar has an obligation to cease these grave violations by the Tatmadaw and other security forces against the Rohingya and to prosecute those responsible.[51] Myanmar is also prohibited from upholding the Tatmadaw’s violent attacks on the Rohingya as lawful, or supporting in any way the commission of these serious breaches of international law.[52] Whereas the violent attacks on the Rohingya have continued, all states also have obligations to invoke Myanmar’s responsibility to prevent these atrocities against the Rohingya, consistent with Myanmar‘sobligations to the international community as a whole.[53]
Since the government of Myanmar has yet to initiate credible investigations[54] into escalating waves of violence against the Rohingya more than three years on, this study highlights the important role that health care workers in Bangladesh who treated the Rohingya can play in substantiating the occurrence of mass atrocities and sexual crimes to facilitate investigations and prosecution in international and domestic jurisdictions.[55] As of this writing, there are several processes ongoing at the international level that seek justice and accountability for serious crimes committed against the Rohingya. These include a case filed at the International Court of Justice by The Gambia against Myanmar for violation of the Genocide Convention,[56] an ongoing investigation by the Office of the Prosecutor at the International Criminal Court into crimes against humanity of deportation, other inhuman acts, and persecution on the grounds of ethnicity and/or religion,[57] [58] and a criminal complaint filed by Rohingya and Latin American human rights groups against Myanmar officials for crimes against humanity and genocide under Argentina’s universal jurisdiction law.[59] The UN also established an Independent Investigative Mechanism for Myanmar, which became operational in August 2019 and which continues to develop case files and analyze materials to be shared with competent authorities.[60]
This report not only adds to the body of documentation demonstrating that the Tatmadaw perpetrated mass atrocities against the Rohingya in Myanmar, but, in sharing the highly credible observations of health care workers, may lay the foundation for reconceptualization of the types of acts that lead to convictions for sexual crimes.[61] [62] The documentation also casts light on the circumstances in which sexual violence occurred in the Myanmar context and may contribute to determinations about how these crimes are adjudicated.[63] Beyond considering the Tatmadaw’s modus operandi, relevant analysis would also factor in the geographic and temporal scope of the violations, that they are “systematic or widespread” in nature, and that they coerce displacement. Consideration should also be given to variance in the treatment of different population groups, pregnancy or abortion rates, and the extent of damage to Rohingya survivors and communities.
PHR thoroughly documented the long-term trauma experienced by survivors and the social, religious, and cultural constraints to their participation in accountability processes. This report’s findings may bolster other evidence gathered, avoiding the potential re-traumatization of survivors, in trying to establish the occurrence of atrocities and related sexual crimes.[64] The observations of health workers treating the Rohingya may also inform protective measures and other forms of assistance for survivors,[65] including the potential relocation of international judicial hearings closer to Cox’s Bazar.[66]
In view of the pervasive physical and psychological sequelae documented in this study, Rohingya victims who were directly and indirectly harmed by the Tatmadaw’s attacks are entitled to reparations from individual perpetrators and the state of Myanmar for the harm suffered.[67] Under the laws of state responsibility, the international community is also due reparations for Myanmar’s breaches of its erga omnes obligations.[68] As a matter of urgency, judicial processes reviewing the Rohingya’s claims should be accompanied by reparations programs and victims’ funds that address the deeply entrenched gender discrimination and inequalities that perpetuate sexual violence and are compensatory, retributive, and restorative in nature.[69] The contributions of survivors and health professionals in reparations program design will be crucial, as specialized medical care may be required to respond to the serious injuries and health complications documented among Rohingya survivors.[70]
The compelling observations of health care workers detailed in this report further accentuate the need for international justice and accountability efforts to be complemented by other forms of transitional justice that prioritize the needs and perspectives of Rohingya survivors and their communities.[71] These efforts may include, but are not limited to, formal and local or community-based truth and reconciliation initiatives, other reparations and compensation programs, the reform of discriminatory laws and institutions, and the preservation of historical memory to honor the Rohingya’s experiences – all designed to prevent recurrence of the violations in question.[72] The accounts of health care providers treating the Rohingya can help inform the factual record of events that guide these processes, while also providing insight into the context, the terminology that Rohingya survivors may use to describe sexual violence, and the role of trauma and stigma in influencing their decisions about justice and the future.[73]
Recommendations
The findings of this report – specifically regarding the scale, brutality, and patterns of sexual violence experienced by the Rohingya in Myanmar, the ongoing experiences of intimate partner violence experienced in Bangladesh, and the severe barriers to care – demand concerted action at the national, regional, and international level. As the state of Myanmar has repeatedly failed to abide by its responsibility to protect the Rohingya and prevent atrocities, it is incumbent on states and other international actors to take appropriate measures to support survivors’ immediate needs for effective, long-term care, victim-centered justice processes, and greater steps towards accountability and guarantees of non-recurrence. In line with states’ and other international actors’ legal obligations and responsibilities to support justice and accountability for survivors, Physicians for Human Rights calls for the immediate and meaningful consideration of the following recommendations:
To the Government of Myanmar:
- Initiate prompt, independent, and impartial criminal investigations into all allegations of grave human rights violations, including the use of sexual violence as a tactic of war, by the Tatmadaw;
- Formally acknowledge the scale and severity of crimes, including sexual violence, committed against the Rohingya by the Tatmadaw and other security forces, and ensure that perpetrators of human rights violations are brought to justice in an independent civil court with provisions for victims to access remedies;
- Urgently undertake legislative reforms that guarantee human rights protections to all ethnic groups, including the Rohingya, in line with obligations under international law;
- Guarantee the safe, dignified, and voluntary repatriation of Rohingya refugees by ensuring robust, codified protections of their human rights, including guarantees of citizenship, restoration of homes and land, and official commitments to prevent any repetition of these crimes.
To the Government of Bangladesh:
- Facilitate access to appropriate medical care for survivors of sexual violence, specifically Rohingya survivors, including psychosocial support;
- Ensure that Rohingya refugees have access to legal protections, immediately granting the Rohingya legal status and official documentation as refugees, and ensure that any plans to repatriate or relocate the Rohingya is premised on safe, dignified, and voluntary return;
- Facilitate efforts to investigate all allegations of grave human rights violations, including sexual violence committed against the Rohingya in Myanmar, including ensuring access to conduct investigations and gather evidence;
- Take increased action to strengthen investigation of and response to rape, sexual assault, and violence within marriage to ensure Rohingya survivors receive adequate protection and access to medical and psychosocial support.
To Humanitarian Agencies, Donors, and Local Service Providers:
- Work toward greater access to comprehensive, survivor-centered care for survivors of sexual violence, including ensuring immediate and long-term access to psychosocial and mental health support for all Rohingya refugees, in recognition of the trauma associated with Myanmar’s “clearance operations” experienced by this population;
- Promote greater access to justice for survivors of sexual violence, including ensuring that those who want to disclose incidents have access to legal support and mechanisms;
- Create and implement reporting and documentation mechanisms for sexual and gender-based violence (SGBV), as well as formal mechanisms to have forensic evidence collected and preserved by trained members of the health sector;
- Promote greater involvement of the Rohingya community in health care service provision and access to justice, particularly related to SGBV and mental health;
- Train and educate service providers across all disciplines and specialties in standards of appropriate, high-quality survivor care that considers and respects survivors’ desires about reporting;
- Ensure health providers and interpreters are adequately trained to identify signs of abuse in vulnerable populations, including child, male, lesbian, gay, bisexual, transgender, queer/questioning, and intersex survivors, to ensure these groups receive adequate medical and psychosocial care;
- Introduce standardized protocols for the systematic documentation of sexual violence to support access to justice for survivors of SGBV and related crimes;
- Create communication materials and campaigns that de-stigmatize SGBV and encourage reporting and seeking health support through available medical and mental health services.
To the International Community:
- Pursue all available means to ensure that all perpetrators of grave violations of human rights, including sexual violence, against the Rohingya are held to account;
- Support the development of a comprehensive international criminal justice process with the necessary financial, technical, legal, and political resources required, ensuring a survivor-centered approach;
- Ensure Myanmar’s compliance with the provisional measures issued by the International Court of Justice to take all measures within its power to protect the Rohingya from genocide, as well as to prevent the perpetration of any further atrocity crimes;
- Recognize that forced witnessing of sexual crimes and sexual humiliation are forms of inhumane acts intentionally causing great suffering, or serious injury to body or to mental or physical health, and should be prosecuted as such;
- Pursue reparations for survivors of sexual violence within judicial processes that are transformative, rehabilitative, and retributive, while ensuring survivor-centered approaches to program design and implementation;
- Ensure international justice and accountability efforts are complemented by other forms of transitional justice designed to prevent recurrence of atrocities and which prioritize the needs and perspectives of Rohingya survivors and their communities;
- Support the safe, dignified, and voluntary repatriation of refugees only with assurances for, and international monitoring of, safety and individual choice, with explicit human rights protections, including citizenship, for the Rohingya.
Acknowledgements
This report was co-written by Shahanoor Akter Chowdhury, MA, MSS, PHR consultant; Lindsey Green, MA, PHR senior program coordinator, Program on Sexual Violence in Conflict Zones; Linda Kaljee, PhD, senior research investigator, Henry Ford Health System, Global Health Initiative; Thomas McHale, SM, PHR deputy director, Program on Sexual Violence in Conflict Zones; and Ranit Mishori, MD, MHS, PHR senior medical advisor, professor of family medicine, Georgetown University School of Medicine.
Research design and implementation was conducted by the report authors as well as by Sharid Bin Shafique, MSS, PHR consultant, and Annekathryn Goodman, MD, MPH, professor of obstetrics, gynecology and reproductive biology, Harvard Medical School, director of Strength and Serenity MGH Global Initiative to End Gender-Based Violence, Massachusetts General Hospital.
Legal analysis was provided by Pratima Narayan, JD, senior program manager, Global Initiative for Justice, Truth and Reconciliation, International Coalition of Sites of Conscience.
Staff of PHR contributed to the writing and editing of this report, including DeDe Dunevant, director of communications; Michele Heisler, MD, MPA, medical director; Karen Naimer, JD, LLM, MA, director of programs; Michael Payne, senior advocacy officer and interim advocacy director; Lawrence Robinson, MA, advocacy coordinator; and Susannah Sirkin, MEd, director of policy.
External review was provided by a range of experts in the fields of medicine, law, and human rights in Myanmar, including Adam Richards, MD, PhD, MPH, PHR board member, senior technical advisor, Community Partners International, and Yasmin Ullah, Rohingya human rights activist.
The report was edited and prepared for publication by Claudia Rader, MS, PHR senior communications manager. Hannah Dunphy, PHR digital communications manager, managed the digital presentation.
Bibliography
Adams, Patrick. “Opinion | How Bangladesh Made Abortion Safer.” The New York Times, December 28, 2018, sec. Opinion. https://www.nytimes.com/2018/12/28/opinion/rohingya-bangladesh-abortion.html.
AFP. “Rape in Myanmar Is ‘Silent Emergency.’” Bangkok Post, March 2, 2020. https://www.bangkokpost.com/world/1869804/rape-in-myanmar-is-silent-emergency.
Ahmed, Kaamil. “Nine Months on, a Race against Time to Find Pregnant Rohingya Rape Survivors.” The New Humanitarian, April 16, 2018. https://www.thenewhumanitarian.org/feature/2018/04/16/nine-months-race-against-time-find-pregnant-rohingya-rape-survivors.
Aljazeera. “Myanmar Finds War Crimes but No Genocide in Rohingya Crackdown.” Aljazeera, January 21, 2020. https://www.aljazeera.com/news/2020/01/21/myanmar-finds-war-crimes-but-no-genocide-in-rohingya-crackdown/.
Bachelet, Michelle. “Increasing Women’s Access to Justice in Post-Conflict Societies.” United Nations. United Nations. Accessed September 28, 2020. https://www.un.org/en/chronicle/article/increasing-womens-access-justice-post-conflict-societies.
“‘Bangladesh Is Not My Country’: The Plight of Rohingya Refugees from Myanmar.” New York, New York: Human Rights Watch, August 2018.
Baro, Daniela. “Children Witnessing Atrocities against Parents or Caregivers, a Human Rights Perspective.” International Rehabilitation Council for Torture Victims 16, no. 3 (2006): 30.
Bassiouni, M. Cherif. “International Crimes: Jus Cogens and Obligatio Erga Omnes.” Law and Contemporary Problems 59, no. 4 (October 1, 1996): 63–74.
Beech, Hannah, Saw Nang, and Marlise Simons. “‘Kill All You See’: In a First, Myanmar Soldiers Tell of Rohingya Slaughter – The New York Times.” The New York Times, September 8, 2020. https://www.nytimes.com/2020/09/08/world/asia/myanmar-rohingya-genocide.html.
Bensouda, Fatou. “Statement of the Prosecutor of the International Criminal Court, Fatou Bensouda, Following Judicial Authorisation to Commence an Investigation into the Situation in Bangladesh/Myanmar,” November 22, 2019. https://www.icc-cpi.int/Pages/item.aspx?name=20191122-otp-statement-bangladesh-myanmar.
Brouwer, Anne-Marie de. “Cases of Mass Sexual Violence Can Be Proven without Direct Victim Testimony.” Contemporary Issues Facing the International Criminal Court, January 1, 2016, 282–94. https://doi.org/10.1163/9789004304451_034.
CEDAW. “CEDAW General Recommendation No. 32 on the Gender-Related Dimensions of Refugee Status, Asylum, Nationality and Statelessness of Women.” UN, 2014. http://digitallibrary.un.org/record/807254.
Chamber I. “Judgement” Prosecutor v. Jean-Paul Akayesu, No. ICTR-96-4 (International Criminal Tribunal for Rwanda September 2, 1998).
Chynoweth, Sarah. “‘It’s Happening to Our Men as Well’: Sexual Violence Against Rohingya Men and Boys.” Women’s Refugee Commission, November 2018. https://www.un.org/sexualviolenceinconflict/wp-content/uploads/report/auto-draft/Rohingya-Report-Final-.pdf.
Correa, Cristian. “Getting to Full Restitution: Guidelines for Court-Ordered Reparations in Cases Involving Sexual Violence Committed during Armed Conflict, Political Violence, or State Repression,” April 2017. https://www.ictj.org/sites/default/files/ICTJ-Briefing-Court-Reparations-2017.pdf.
Dedoose, Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data. (version 8.3.35). Los Angeles, CA: SocioCultural Research Consultants, LLC, 2020. www.dedoose.com.
Eggett, Craig. “Clarification and Conflation: Obligations Erga Omnes in the Chagos Opinion.” EJIL: Talk! (blog), May 21, 2019. https://www.ejiltalk.org/clarification-and-conflation-obligations-erga-omnes-in-the-chagos-opinion/.
Fetters, Tamara, Sayed Rubayet, Sharmin Sultana, Shamila Nahar, Shadie Tofigh, Lea Jones, Ghazaleh Samandari, and Bill Powell. “Navigating the Crisis Landscape: Engaging the Ministry of Health and United Nations Agencies to Make Abortion Care Available to Rohingya Refugees.” Conflict and Health 14, no. 1 (December 2020): 50. https://doi.org/10.1186/s13031-020-00298-6.
Gelineau, Kristen. “Rohingya Methodically Raped by Myanmar’s Armed Forces.” Associated Press, December 11, 2017.
Gilmore, Sunneva. “Meeting the Needs of Victims of Sexual Violence through Reparations.” IntLawGrrls (blog), November 1, 2019. https://ilg2.org/2019/11/01/meeting-victims-needs-through-reparations-for-sexual-violence/.
Global Justice Center. “Discrimination To Destruction: A Legal Analysis of Gender Crimes Against the Rohingya.” Global Justice Center, September 2018. https://globaljusticecenter.net/files/Discrimination_to_Destruction.pdf.
———. “Myanmar/Burma’s Binding Obligations Under International Law,” November 2012. https://www.globaljusticecenter.net/documents/BindingObligations.pdf.
Gorlick, Brian. “The Rohingya Refugee Crisis, International Justice, and Rethinking Solutions.” Andrew & Renata Kaldor Centre for International Refugee Law at UNSW Sydney, September 21, 2020. https://www.kaldorcentre.unsw.edu.au/publication/rohingya-refugee-crisis-international-justice-and-rethinking-solutions.
Guttmacher Institute. “Menstrual Regulation and Unsafe Abortion in Bangladesh.” Guttmacher Institute, March 2017. https://www.guttmacher.org/fact-sheet/menstrual-regulation-unsafe-abortion-bangladesh.
Haar, Rohini J., Karen Wang, Homer Venters, Satu Salonen, Rupa Patel, Tamaryn Nelson, Ranit Mishori, and Parveen K. Parmar. “Documentation of Human Rights Abuses among Rohingya Refugees from Myanmar.” Conflict and Health 13, no. 1 (December 2019): 42. https://doi.org/10.1186/s13031-019-0226-9.
Henckaerts, Jean-Marie, Louise Doswald-Beck, Carolin Alvermann, and International Committee of the Red Cross, eds. Customary International Humanitarian Law. Cambridge ; New York: Cambridge University Press, 2005.
Htusan, Esther. “Lack of Health Care Deadly for Burma’s Rohingya.” Washington Post, May 8, 2014, sec. World. https://www.washingtonpost.com/world/lack-of-health-care-deadly-for-burmas-rohingya/2014/05/08/ac5a9ae8-d6e6-11e3-8a78-8fe50322a72c_story.html.
Human Rights Watch. “Myanmar’s Investigative Commissions: A History of Shielding Abusers.” Human Rights Watch, September 2018. https://reliefweb.int/sites/reliefweb.int/files/resources/201809myanmar_commissions.pdf.
Hutchinson, Susan. “Gendered Insecurity in the Rohingya Crisis.” Australian Journal of International Affairs 72, no. 1 (January 2, 2018): 1–9. https://doi.org/10.1080/10357718.2017.1402291.
Institute on Statelessness and Inclusion. “Statelessness and Human Rights: The Convention on the Elimination of All Forms of Discrimination Against Women,” 2018. https://www.refworld.org/docid/5f50a8e54.html.
Inter-Agency Standing Committee. “Reference Module for Cluster Coordination at Country Level,” July 2015. https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/cluster_coordination_reference_module_2015_final.pdf.
International Center for Transitional Justice. “When No One Calls It Rape: Addressing Sexual Violence Against Men and Boys,” December 7, 2016. https://www.ictj.org/publication/sexual-violence-men-boys.
International Court of Justice. “Press Release: The Court Indicates Provisional Measures in Order to Preserve Certain Rights Claimed by The Gambia for the Protection of the Rohingya in Myanmar,” January 23, 2020. https://www.icj-cij.org/files/case-related/178/178-20200123-PRE-01-00-EN.pdf.
———. “Press Release: The Republic of The Gambia Institutes Proceedings against the Republic of the Union of Myanmar and Asks the Court to Indicate Provisional Measures,” November 11, 2019. https://www.icj-cij.org/files/case-related/178/178-20191111-PRE-01-00-EN.pdf.
———. “Reparation for Injuries Suffered in the Service of the United Nations, Advisory Opinion,” April 11, 1949. https://www.icj-cij.org/files/case-related/4/004-19490411-ADV-01-00-EN.pdf.
International Criminal Court. “Rules of Procedure and Evidence,” September 2002. https://www.icc-cpi.int/iccdocs/pids/legal-texts/rulesprocedureevidenceeng.pdf.
International Law Commission. “Draft Articles on Responsibility of States for Internationally Wrongful Acts, with Commentaries,” 2001.
———. “Report of the International Law Commission on the Work of Its Fifty-Third Session (23 April–1 June and 2 July–10 August 2001),” 2001, 209.
———. “Responsibility of States for Internationally Wrongful Acts,” 2001. https://doi.org/10.1007/978-1-4020-8367-9_22.
Ives, Mike. “Rohingya Face Health Care Bias in Parts of Asia, Study Finds.” The New York Times, December 5, 2016, sec. World. https://www.nytimes.com/2016/12/05/world/asia/rohingya-myanmar-health-care.html.
Johnson, Jeffrey C. Selecting Ethnographic Informants. Vol. 22. Qualitative Research Methods. Newbury Park, CA: SAGE Publications, 1990.
Khin, Maung Tun. “Complainant Files a Criminal Complaint of Genocide and Crimes against Humanity Committed against the Rohingya Community in Myanmar–Universal Jurisdiction,” 2019. https://burmacampaign.org.uk/media/Complaint-File.pdf.
Lavery, Kirsten. “The Path Towards Justice: Accountability for International Crimes Against the Rohingya of Burma.” United States Commission on International Religious Freedom, 2020.
Lupig, Diane. “Investigation and Prosecution of Sexual and Gender-Based Crimes before the International Criminal Court.” Journal of Gender, Social Policy & the Law 17 (2009): 62.
Medecins Sans Frontieres. “‘No One Was Left’ Death and Violence Against the Rohingya in Rakhine State, Myanmar.” Medecins Sans Frontieres, March 2018. https://msf.or.ke/sites/default/files/msfpublications/no-one-was-left.pdf.
Messner, Nicole, Andrea Woods, Agnes Petty, Parveen K. Parmar, Jennifer Leigh, Ernest Thomas, Douglass Curry, et al. “Qualitative Evidence of Crimes against Humanity: The August 2017 Attacks on the Rohingya in Northern Rakhine State, Myanmar.” Conflict and Health 13, no. 1 (December 2019): 41. https://doi.org/10.1186/s13031-019-0227-8.
Mills, Laura, and Rupa Patel. “Shot While Fleeing: Rohingya Disabled by Myanmar Authorities’ Targeted Violence.” Physicans for Human Rights, June 25, 2019. https://phr.org/our-work/resources/shot-while-fleeing-rohingya-disabled-by-myanmar-authorities-targeted-violence/.
Ministerie van Buitenlandse Zaken. “Joint Statement of Canada and the Kingdom of the Netherlands.” Diplomatieke_verklaring. Ministerie van Algemene Zaken, December 9, 2019. https://www.government.nl/documents/diplomatic-statements/2019/12/09/joint-statement-of-canada-and-the-kingdom-of-the-netherlands.
Morse, Jaimie. “Documenting Mass Rape: Medical Evidence Collection Techniques as Humanitarian Technology.” Genocide Studies and Prevention 8, no. 3 (October 2014): 63–79. https://doi.org/10.5038/1911-9933.8.3.6.
Morse, Janice M. “The Significance of Saturation:” Qualitative Health Research, July 1, 2016. https://doi.org/10.1177/104973239500500201.
“MSF Shocked at Shutdown in Myanmar.” BBC News, February 28, 2014, sec. Asia. https://www.bbc.com/news/world-asia-26379804.
Human Rights Watch. “Myanmar Bars Rohingya Candidates from Elections, Again,” August 18, 2020. https://www.hrw.org/news/2020/08/18/myanmar-bars-rohingya-candidates-elections-again.
Fortify Rights. “Myanmar: Ensure Rohingya Participation in Elections,” August 12, 2020. https://www.fortifyrights.org/mya-inv-2020-08-12/.
UN News. “Myanmar: Upcoming Elections an Opportunity to Take a New Inclusive Democratic Path,” August 28, 2020. https://news.un.org/en/story/2020/08/1071232.
Nu, Wai Wai, and Maggi Quadrini. “Myanmar’s Justice System Is Failing Survivors of Sexual Violence.” The Diplomat, February 13, 2020. https://thediplomat.com/2020/02/myanmars-justice-system-is-failing-survivors-of-sexual-violence/.
Office of the High Commissioner for Human Rights. “CESCR General Comment No. 14: The Right to the Highest Attainable Standard of Health (Art. 12),” August 11, 2000.
Office of the Prosecutor. Situation in the People’s Republic of Bangladesh/Republic of the Union of Myanmar, No. ICC-01/19-7 (International Criminal Court July 4, 2019).
Oosterveld, Valerie. “Sexual and Gender-Based Violence in Post-Conflict Sierra Leone: The Contribution of Transitional Justice Mechanisms to Domestic Law Reform.” In Evaluating Transitional Justice: Accountability and Peacebuilding in Post-Conflict Sierra Leone, edited by Kirsten Ainley, Rebekka Friedman, and Chris Mahony, 129–51. Rethinking Peace and Conflict Studies. London: Palgrave Macmillan UK, 2015. https://doi.org/10.1057/9781137468222_7.
Parmar, Parveen K., Jennifer Leigh, Homer Venters, and Tamaryn Nelson. “Violence and Mortality in the Northern Rakhine State of Myanmar, 2017: Results of a Quantitative Survey of Surviving Community Leaders in Bangladesh.” The Lancet Planetary Health 3, no. 3 (March 1, 2019): e144–53. https://doi.org/10.1016/S2542-5196(19)30037-3.
Patten, Pramila. Statement by the Special Representative of the Secretary-General on Sexual Violence in Conflict, Ms. Pramila Patten, § UN Security Council Briefing on Myanmar (2017). https://www.un.org/sexualviolenceinconflict/statement/statement-by-the-special-representative-of-the-secretary-general-on-sexual-violence-in-conflict-ms-pramila-patten-security-council-briefing-on-myanmar-12-december-2017/.
Physicians for Human Rights. “Patterns of Anti-Muslim Violence in Burma: A Call for Accountability and Prevention.” New York, NY: Physicians for Human Rights, 2013.
———. “Stateless and Starving: Persecuted Rohingya Flee Burma and Starve in Bangladesh.” Cambridge, Mass.: PHR, 2010.
———. “The Chut Pyin Massacre: Forensic Evidence of Violence against the Rohingya in Myanmar.” Physicians for Human Rights, July 2018. https://rohingya.phr.org/wp-content/uploads/2018/07/PHR-Chut-Pyin-report-July-2018.pdf.
———. “Where There Is Police, There Is Persecution: Government Security Forces and Human Rights Abuses in Myanmar’s Northern Rakhine State.” New York, NY: Physicians for Human Rights, 2016.
———. “Widespread and Systematic: Violence against the Rohingya in Myanmar.” Physicians for Human Rights, August 2018. https://doi.org/10.1163/2210-7975_HRD-2259-20180060.
Prosecutor v. Anto Furundizja, No. IT-95-17/1 (International Criminal Tribunal for the former Yugoslavia December 10, 1998).
Redress. “Making Sense of Reparations at the International Criminal Court.” Koninklijke Brill NV, June 20, 2018. https://doi.org/10.1163/2210-7975_HRD-5555-20180007.
Riley, Andrew, Yasmin Akther, Mohammed Noor, Rahmat Ali, and Courtney Welton-Mitchell. “Systematic Human Rights Violations, Traumatic Events, Daily Stressors and Mental Health of Rohingya Refugees in Bangladesh.” Conflict and Health 14, no. 1 (August 20, 2020): 60. https://doi.org/10.1186/s13031-020-00306-9.
Ryan, Sophie. “When Women Become the War Zone: The Use of Sexual Violence in Myanmar’s Military Operations.” Global Responsibility to Protect 12, no. 1 (February 17, 2020): 37–63. https://doi.org/10.1163/1875984X-01201004.
Sellers, Patricia Viseur. “The Prosecution of Sexual Violence in Conflict: The Importance of Human Rights as Means of Interpretation.,” 2007, 41.
“Situation Refugee Response in Bangladesh.” Accessed July 20, 2020. https://data2.unhcr.org/en/situations/myanmar_refugees.
Strategic Executive Group. “JRP for Rohingya Humanitarian Crisis: March-December 2018,” 2018. https://reporting.unhcr.org/sites/default/files/JRP%20for%20Rohingya%20Humanitarian%20Crisis%20-%20March%202018.PDF.
Sultana, Razia. “Rape by Command. Sexual Violence as a Weapon against the Rohingya.” Kaladan Press Network, February 2018. https://www.kaladanpress.org/images/document/2018/RapebyCommandWeb3.pdf.
Opinio Juris. “The International Court of Justice and the Rohingya: The Long Road Ahead for Accountability,” November 6, 2019. http://opiniojuris.org/2019/11/06/the-international-court-of-justice-and-the-rohingya-the-long-road-ahead-for-accountability/.
The Office of the Prosecutor, International Criminal Court. “Policy Paper on Sexual and Gender-Based Crimes,” June 2014.
Thuy Seelinger, Kim, Helene Silverberg, and Robin Mejia. “The Investigation and Prosecution of Sexual Violence.” Human Rights Center, University of California Berkeley, May 2011. https://www.law.berkeley.edu/wp-content/uploads/2015/04/The-Investigation-and-Prosecution-of-Sexual-Violence-SV-Working-Paper.pdf.
Tsai, Jennifer, and Simon Robins. “Strengthening Participation in Local-Level and National Transitional Justice Processes: A Guide for Practitioners.” International Coalition of Sites of Conscience, June 2018. https://www.sitesofconscience.org/wp-content/uploads/2018/06/Strengthening-Participation-Toolkit-online.pdf.
UN Committee on the Elimination of Discrimination Against Women (CEDAW). “CEDAW General Recommendation No. 24: Article 12 of the Convention (Women and Health),” 1999. https://www.refworld.org/docid/453882a73.html.
———. “Concluding Observations on the Report of Myanmar Submitted under the Exceptional Reporting Procedure.” UN, March 18, 2019. http://digitallibrary.un.org/record/3800291.
———. “General Recommendation No. 30 on Women in Conflict Prevention, Conflict and Post-Conflict Situations,” November 1, 2013. https://www.refworld.org/docid/5268d2064.html.
UN Human Rights Committee. “General Comment No. 36 (2018) on Article 6 of the International Covenant on Civil and Political Rights, on the Right to Life,” October 20, 2018. https://tbinternet.ohchr.org/Treaties/CCPR/Shared%20Documents/1_Global/CCPR_C_GC_36_8785_E.pdf.
UN Human Rights Council. “Report of the Independent International Fact-Finding Mission on Myanmar.” UN Human Rights Council, September 12, 2018. https://documents-dds-ny.un.org/doc/UNDOC/GEN/G18/274/54/PDF/G1827454.pdf?OpenElement.
———. “Sexual and Gender-Based Violence in Myanmar and the Gendered Impact of Its Ethnic Conflicts.” UN Human Rights Council, August 22, 2019. https://www.ohchr.org/Documents/HRBodies/HRCouncil/FFM-Myanmar/sexualviolence/A_HRC_CRP_4.pdf.
UN News. “For Rohingya Refugees, Imminent Surge in Births Is Traumatic Legacy of Sexual Violence – Special Report.” UN News, May 11, 2018. https://news.un.org/en/story/2018/05/1009372.
———. “Reparations for Sexual Violence in Conflict – ‘What Survivors Want Most, yet Receive Least,’” October 30, 2019. https://reliefweb.int/report/world/reparations-sexual-violence-conflict-what-survivors-want-most-yet-receive-least.
UN Secretary General. “Guidance Note of the Secretary-General : Reparations for Conflict-Related Sexual Violence.” UN, 2014. http://digitallibrary.un.org/record/814902.
UN Special Rapporteur on the promotion of truth, justice, reparation and guarantees of non-recurrence. “The Foundation of the Mandate and the Importance of a Comprehensive Approach That Combines the Elements of Truth-Seeking, Justice Initiatives, Reparations and Guarantees of Non-Recurrence in a Complementary and Mutually Reinforcing Manner.” United Nations, December 27, 2016. https://undocs.org/en/A/HRC/34/62.
United Nations. “Charter of the United Nations: 1 UNTS XVI, Arts. 55(c) and 56, 103,” October 24, 1945. https://www.un.org/en/charter-united-nations/index.html.
———. “Universal Declaration of Human Rights: 217 A (III), Art. 15,” December 10, 1948. https://www.un.org/en/universal-declaration-human-rights/.
———. “Vienna Convention on the Law of Treaties,” May 23, 1969. https://www.refworld.org/docid/3ae6b3a10.html.
United Nations Committee on Economic, Social and Cultural Rights. “CESCR General Comment No. 22 (2016) on the Right to Sexual and Reproductive Health (Article 12 of the International Covenant on Economic, Social and Cultural Rights) E/C.12/GC/22,” May 2, 2016. https://undocs.org/E/C.12/GC/22.
United Nations General Assembly. “Basic Principles and Guidelines on the Right to a Remedy and Reparation for Victims of Gross Violations of International Human Rights Law and Serious Violations of International Humanitarian Law,” March 21, 2006. https://www.ohchr.org/EN/ProfessionalInterest/Pages/RemedyAndReparation.aspx.
———. “Convention on the Rights of Persons with Disabilities,” December 13, 2006. https://www.refworld.org/docid/4680cd212.html.
———. “Convention on the Rights of the Child,” November 20, 1989. https://www.ohchr.org/Documents/ProfessionalInterest/crc.pdf.
———. “International Covenant on Civil and Political Rights,” December 16, 1966. https://www.ohchr.org/Documents/ProfessionalInterest/ccpr.pdf.
———. “International Covenant on Economic, Social and Cultural Rights,” December 16, 1966. https://www.refworld.org/docid/3ae6b36c0.html.
———. “Optional Protocol to the Convention on the Rights of the Child on a Communications Procedure : Resolution / Adopted by the General Assembly,” January 27, 2012. https://www.refworld.org/docid/5290acdc4.html.
United Nations High Commissioner for Refugees. “Convention Relating to the Status of Refugees.” Refworld, July 28, 1951. https://www.refworld.org/docid/3be01b964.html.
———. “Human Rights and Arbitrary Deprivation of Nationality: Report of the Secretary-General,” December 19, 2013. https://www.refworld.org/docid/52f8d19a4.html.
———. “The Rights of Non-Citizens,” 2006. https://www.refworld.org/docid/46ceabb22.html.
Van Shaak, Beth. “Obstacles on the Road to Gender Justice: The International Criminal Tribunal for Rwanda as Object Lesson.” American University Journal of Gender, Social Policy & the Law 17, no. 2 (2009).
Frontier Myanmar. “We, the Rohingya, Can’t Wait for Justice from Faraway Courts,” May 28, 2020. https://www.frontiermyanmar.net/en/we-the-rohingya-cant-wait-for-justice-from-faraway-courts/.
Wheeler, Skye. “All of My Body Was Pain”: Sexual Violence against Rohingya Women and Girls in Burma. New York: Human Rights Watch, 2017.
WHO and United Nations Office on Drugs and Crime (UNODC). “Strengthening the Medico-Legal Response to Sexual Violence.” World Health Organization, November 2015. http://www.who.int/reproductivehealth/publications/violence/medico-legal-response/en/.
“Who Are the Rohingya Group behind Attacks?” BBC News, September 6, 2017, sec. Asia. https://www.bbc.com/news/world-asia-41160679.
Endnotes
[1] Wheeler, All of My Body Was Pain; UN Human Rights Council, “Sexual and Gender-Based Violence in Myanmar and the Gendered Impact of Its Ethnic Conflicts”; UN Human Rights Council, “Report of the Independent International Fact-Finding Mission on Myanmar”; Patten, Statement by the Special Representative of the Secretary-General on Sexual Violence in Conflict, Ms. Pramila Patten; Chynoweth, “‘It’s Happening to Our Men as Well’: Sexual Violence Against Rohingya Men and Boys”; Gelineau, “Rohingya Methodically Raped by Myanmar’s Armed Forces”; Medecins Sans Frontieres, “‘No One Was Left’ Death and Violence Against the Rohingya in Rakhine State, Myanmar”; Ryan, “When Women Become the War Zone”; Global Justice Center, “Discrimination To Destruction: A Legal Analysis of Gender Crimes Against the Rohingya”; Sultana, “Rape by Command. Sexual Violence as a Weapon against the Rohingya.”
[2] Parmar et al., “Violence and Mortality in the Northern Rakhine State of Myanmar, 2017”; Physicians for Human Rights, “Where There Is Police, There Is Persecution”; Physicians for Human Rights, “Stateless and Starving”; Physicians for Human Rights, “Patterns of Anti-Muslim Violence in Burma.”
[3] As of this writing, Rohingya are barred from participating in Myanmar’s November 2020 election, both as voters and candidates.
[4] Haar et al., “Documentation of Human Rights Abuses among Rohingya Refugees from Myanmar”; “Myanmar,” August 28, 2020; “Myanmar,” August 12, 2020; “Myanmar Bars Rohingya Candidates from Elections, Again.”
[5] “Who Are the Rohingya Group behind Attacks?”
[6] Physicians for Human Rights, “The Chut Pyin Massacre: Forensic Evidence of Violence against the Rohingya in Myanmar.”
[7] Physicians for Human Rights; UN Human Rights Council, “Report of the Independent International Fact-Finding Mission on Myanmar.”
[8] “Situation Refugee Response in Bangladesh.”
[9] “Bangladesh Is Not My Country.”
[10] Physicians for Human Rights, “Widespread and Systematic”; Parmar et al., “Violence and Mortality in the Northern Rakhine State of Myanmar, 2017”; Physicians for Human Rights, “The Chut Pyin Massacre: Forensic Evidence of Violence against the Rohingya in Myanmar”; UN Human Rights Council, “Report of the Independent International Fact-Finding Mission on Myanmar”; Medecins Sans Frontieres, “‘No One Was Left’ Death and Violence Against the Rohingya in Rakhine State, Myanmar.”
[11] Parmar et al., “Violence and Mortality in the Northern Rakhine State of Myanmar, 2017.”
[12] Physicians for Human Rights, “Widespread and Systematic.”
[13] UN Human Rights Council, “Sexual and Gender-Based Violence in Myanmar and the Gendered Impact of Its Ethnic Conflicts”; UN Human Rights Council, “Report of the Independent International Fact-Finding Mission on Myanmar”; Beech, Nang, and Simons, “‘Kill All You See’: In a First, Myanmar Soldiers Tell of Rohingya Slaughter – The New York Times.”
[14] UN Human Rights Council, “Sexual and Gender-Based Violence in Myanmar and the Gendered Impact of Its Ethnic Conflicts”; Sultana, “Rape by Command. Sexual Violence as a Weapon against the Rohingya.”; Ryan, “When Women Become the War Zone”; Wheeler, All of My Body Was Pain; Gelineau, “Rohingya Methodically Raped by Myanmar’s Armed Forces”; Global Justice Center, “Discrimination To Destruction: A Legal Analysis of Gender Crimes Against the Rohingya.”
[15] UN Human Rights Council, “Sexual and Gender-Based Violence in Myanmar and the Gendered Impact of Its Ethnic Conflicts”; Wheeler, All of My Body Was Pain; Ryan, “When Women Become the War Zone”; Chynoweth, “‘It’s Happening to Our Men as Well’: Sexual Violence Against Rohingya Men and Boys”; Medecins Sans Frontieres, “‘No One Was Left’ Death and Violence Against the Rohingya in Rakhine State, Myanmar”; Patten, Statement by the Special Representative of the Secretary-General on Sexual Violence in Conflict, Ms. Pramila Patten; Global Justice Center, “Discrimination To Destruction: A Legal Analysis of Gender Crimes Against the Rohingya.”
[16] Wheeler, All of My Body Was Pain; UN Human Rights Council, “Sexual and Gender-Based Violence in Myanmar and the Gendered Impact of Its Ethnic Conflicts.”
[17] Medecins Sans Frontieres, “‘No One Was Left’ Death and Violence Against the Rohingya in Rakhine State, Myanmar”; Global Justice Center, “Discrimination To Destruction: A Legal Analysis of Gender Crimes Against the Rohingya.”
[18] Chynoweth, “‘It’s Happening to Our Men as Well’: Sexual Violence Against Rohingya Men and Boys.”
[19] UN Human Rights Council, “Sexual and Gender-Based Violence in Myanmar and the Gendered Impact of Its Ethnic Conflicts.”
[20] Johnson, Selecting Ethnographic Informants.
[21] Morse, “The Significance of Saturation.”
[22] Dedoose, Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data.
[23] Ahmed, “Nine Months on, a Race against Time to Find Pregnant Rohingya Rape Survivors”; UN News, “For Rohingya Refugees, Imminent Surge in Births Is Traumatic Legacy of Sexual Violence – Special Report.”
[24] Hutchinson, “Gendered Insecurity in the Rohingya Crisis.”
[25] Guttmacher Institute, “Menstrual Regulation and Unsafe Abortion in Bangladesh.”
[26] Guttmacher Institute.
[27] Adams, “Opinion | How Bangladesh Made Abortion Safer”; Fetters et al., “Navigating the Crisis Landscape.”
[28] Strategic Executive Group, “JRP for Rohingya Humanitarian Crisis: March-December 2018.”
[29] Inter-Agency Standing Committee, “Reference Module for Cluster Coordination at Country Level.”
[30] Strategic Executive Group, “JRP for Rohingya Humanitarian Crisis: March-December 2018.”
[31] “Bangladesh Is Not My Country.”
[32] Ives, “Rohingya Face Health Care Bias in Parts of Asia, Study Finds”; “MSF Shocked at Shutdown in Myanmar”; Htusan, “Lack of Health Care Deadly for Burma’s Rohingya.”
[33] Mnemonic for: Sleep, Interest, Guilt, Energy, Concentration, and Appetite, Psychomotor, and Suicidal ideation.
[34] PHQ-9 is the depression module of Patient Health Questionnaire (PHQ). A self-administered version of the PRIME-MD diagnostic instrument for common mental disorders.
[35] In this quotation Malaysia is used as an example of a different context for which screening tools would be used.
[36] “U.S. Preventive Services Task Force is an independent, volunteer panel of national experts in disease prevention and evidence-based medicine. The Task Force works to improve the health of all Americans by making evidence-based recommendations about clinical preventive services.” (https://www.uspreventiveservicestaskforce.org/uspstf/)
[37] Wheeler, All of My Body Was Pain; UN Human Rights Council, “Sexual and Gender-Based Violence in Myanmar and the Gendered Impact of Its Ethnic Conflicts”; UN Human Rights Council, “Report of the Independent International Fact-Finding Mission on Myanmar”; Patten, Statement by the Special Representative of the Secretary-General on Sexual Violence in Conflict, Ms. Pramila Patten; Chynoweth, “‘It’s Happening to Our Men as Well’: Sexual Violence Against Rohingya Men and Boys”; Gelineau, “Rohingya Methodically Raped by Myanmar’s Armed Forces”; Medecins Sans Frontieres, “‘No One Was Left’ Death and Violence Against the Rohingya in Rakhine State, Myanmar”; Ryan, “When Women Become the War Zone”; Global Justice Center, “Discrimination To Destruction: A Legal Analysis of Gender Crimes Against the Rohingya”; Sultana, “Rape by Command. Sexual Violence as a Weapon against the Rohingya.”
[38] In its General Recommendations, The Convention on the Elimination of all Forms of Discrimination Against Women (CEDAW) has also observed ”State parties have an obligation to ensure that no woman will be expelled or returned to another State where her life, physical integrity, liberty and security of person would be threatened, or where she would risk suffering serious forms of discrimination, including serious forms of gender-based persecution or gender-based violence…”
[39] International Court of Justice, “Press Release: The Court Indicates Provisional Measures in Order to Preserve Certain Rights Claimed by The Gambia for the Protection of the Rohingya in Myanmar”; CEDAW, “CEDAW General Recommendation No. 32 on the Gender-Related Dimensions of Refugee Status, Asylum, Nationality and Statelessness of Women.”
[40] Notwithstanding Myanmar’s domestic laws and regional commitments, the Rohingya are entitled to protection under public international law.
[41] United Nations, “Charter of the United Nations: 1 UNTS XVI, Arts. 55(c) and 56, 103”; United Nations, “Universal Declaration of Human Rights: 217 A (III), Art. 15”; United Nations High Commissioner for Refugees, “Convention Relating to the Status of Refugees”; United Nations High Commissioner for Refugees, “Human Rights and Arbitrary Deprivation of Nationality.”
[42] In addition to the Genocide Convention, Myanmar has ratified, inter alia, the Four Geneva Conventions of 12 August 1949, as well as the International Covenant on Economic, Social and Cultural Rights; Convention on the Elimination of All Forms of Discrimination against Women (CEDAW); the Convention on the Rights of the Child (CRC); Convention on the Rights of Persons with Disabilities (CRPD); Optional Protocol to the Convention on the Rights of the Child on a communications procedure (CRC-OP-SC).
[43] Global Justice Center, “Myanmar/Burma’s Binding Obligations Under International Law”; United Nations General Assembly, “International Covenant on Economic, Social and Cultural Rights”; United Nations General Assembly, “Convention on the Rights of the Child”; United Nations General Assembly, “Convention on the Rights of Persons with Disabilities”; United Nations General Assembly, “Optional Protocol to the Convention on the Rights of the Child on a Communications Procedure”; Henckaerts et al., Customary International Humanitarian Law.
[44] States have a duty to guarantee the human rights of all persons within their territories or under their jurisdictions, without distinction. Further, states may only distinguish between citizens and non-citizens where it serves a legitimate State objective and is necessary and proportional to the achievement of this objective.
[45] United Nations, “Universal Declaration of Human Rights: 217 A (III), Art. 15”; United Nations High Commissioner for Refugees, “The Rights of Non-Citizens”; UN Human Rights Council, “Report of the Independent International Fact-Finding Mission on Myanmar.”
[46] UN Human Rights Council, “Report of the Independent International Fact-Finding Mission on Myanmar”; United Nations, “Universal Declaration of Human Rights: 217 A (III), Art. 15”; United Nations General Assembly, “Basic Principles and Guidelines on the Right to a Remedy and Reparation for Victims of Gross Violations of International Human Rights Law and Serious Violations of International Humanitarian Law.”
[47] United Nations General Assembly, “International Covenant on Economic, Social and Cultural Rights”; United Nations Committee on Economic, Social and Cultural Rights, “CESCR General Comment No. 22 (2016) on the Right to Sexual and Reproductive Health (Article 12 of the International Covenant on Economic, Social and Cultural Rights) E/C.12/GC/22”; Office of the High Commissioner for Human Rights, “CESCR General Comment No. 14: The Right to the Highest Attainable Standard of Health (Art. 12)”; UN Committee on the Elimination of Discrimination Against Women (CEDAW), “Refworld | CEDAW General Recommendation No. 24”; UN Committee on the Elimination of Discrimination Against Women (CEDAW), “General Recommendation No. 30 on Women in Conflict Prevention, Conflict and Post-Conflict Situations”; United Nations General Assembly, “Convention on the Rights of the Child”; United Nations General Assembly, “International Covenant on Civil and Political Rights”; UN Human Rights Committee, “General Comment No. 36 (2018) on Article 6 of the International Covenant on Civil and Political Rights, on the Right to Life”; United Nations High Commissioner for Refugees, “Convention Relating to the Status of Refugees”; Institute on Statelessness and Inclusion, “Refworld | Statelessness and Human Rights.”
[48] Norms accepted and recognized by the international community as a whole.
[49] United Nations, “Vienna Convention on the Law of Treaties”; International Law Commission, “Report of the International Law Commission on the Work of Its Fifty-Third Session (23 April–1 June and 2 July–10 August 2001)”; Eggett, “Clarification and Conflation.”
[50] Chamber I, “Judgement” Prosecutor v. Jean-Paul Akayesu.
[51] International Law Commission, “Responsibility of States for Internationally Wrongful Acts”; UN Human Rights Council, “Report of the Independent International Fact-Finding Mission on Myanmar”; Bassiouni, “International Crimes”; International Law Commission, “Draft Articles on Responsibility of States for Internationally Wrongful Acts, with Commentaries.”
[52]International Law Commission, “Report of the International Law Commission on the Work of Its Fifty-Third Session (23 April–1 June and 2 July–10 August 2001)”; International Law Commission, “Draft Articles on Responsibility of States for Internationally Wrongful Acts, with Commentaries.”
[53] International Law Commission, “Report of the International Law Commission on the Work of Its Fifty-Third Session (23 April–1 June and 2 July–10 August 2001)”; Eggett, “Clarification and Conflation.”
[54] Aljazeera, “Myanmar Finds War Crimes but No Genocide in Rohingya Crackdown”; Human Rights Watch, “Myanmar’s Investigative Commissions: A History of Shielding Abusers.”
[55] Morse, “Documenting Mass Rape”; The Office of the Prosecutor, International Criminal Court, “Policy Paper on Sexual and Gender-Based Crimes”; Van Shaak, Beth, “Obstacles on the Road to Gender Justice: The International Criminal Tribunal for Rwanda as Object Lesson”; Nu and Quadrini, “Myanmar’s Justice System Is Failing Survivors of Sexual Violence”; AFP, “Rape in Myanmar Is ‘Silent Emergency.’”
[56] International Court of Justice, “Press Release: The Republic of The Gambia Institutes Proceedings against the Republic of the Union of Myanmar and Asks the Court to Indicate Provisional Measures”; Ministerie van Buitenlandse Zaken, “Joint Statement of Canada and the Kingdom of the Netherlands.”
[57] While the Office of the Prosecutor at the ICC submitted her request for an investigation, specifying the crimes enumerated in articles 7(1)(d), (h) and (k) of the Rome Statute, she expressly requested authorization to investigate other conduct that emerges during the course of her investigations which may violate art. 5. These include the crimes of genocide; crimes against humanity; war crimes; and the crime of aggression.
Office of the Prosecutor, Situation in the People’s Republic of Bangladesh/Republic of the Union of Myanmar; Bensouda, “Statement of the Prosecutor of the International Criminal Court, Fatou Bensouda, Following Judicial Authorisation to Commence an Investigation into the Situation in Bangladesh/Myanmar.”
[59] Lavery, “The Path Towards Justice: Accountability for International Crimes Against the Rohingya of Burma”; Khin, “Complainant Files a Criminal Complaint of Genocide and Crimes against Humanity Committed against the Rohingya Community in Myanmar–Universal Jurisdiction.”
[60] UN Independent Investigative Mechanism for Myanmar (IIMM), available at https://iimm.un.org/. The mandate of the UN Independent International Fact-Finding Mission on Myanmar (FFM) which served as a precursor to the IIMM concluded in September 2019.
[61] Acknowledging the sexual acts that constitute criminal offenses vary by jurisdiction; forced witnessing and sexual humiliation are not currently specified within the definitions of sexual violence. While this does not in itself preclude prosecuting these violations, the manner in which the courts have reviewed these cases has not been consistent.
[62] WHO and United Nations Office on Drugs and Crime (UNODC), “Strengthening the Medico-Legal Response to Sexual Violence”; Baro, “Children Witnessing Atrocities against Parents or Caregivers, a Human Rights Perspective”; Prosecutor v. Anto Furundizja; Chamber I, “Judgement” Prosecutor v. Jean-Paul Akayesu; Chynoweth, “‘It’s Happening to Our Men as Well’: Sexual Violence Against Rohingya Men and Boys.”
[63] WHO and United Nations Office on Drugs and Crime (UNODC), “Strengthening the Medico-Legal Response to Sexual Violence”; Baro, “Children Witnessing Atrocities against Parents or Caregivers, a Human Rights Perspective”; Prosecutor v. Anto Furundizja; Chamber I, “Judgement” Prosecutor v. Jean-Paul Akayesu; Lupig, “Investigation and Prosecution of Sexual and Gender-Based Crimes before the International Criminal Court”; Thuy Seelinger, Silverberg, and Mejia, “The Investigation and Prosecution of Sexual Violence”; Chynoweth, “‘It’s Happening to Our Men as Well’: Sexual Violence Against Rohingya Men and Boys.”
[64] Brouwer, “Cases of Mass Sexual Violence Can Be Proven without Direct Victim Testimony”; Thuy Seelinger, Silverberg, and Mejia, “The Investigation and Prosecution of Sexual Violence.”
[65] UN Committee on the Elimination of Discrimination Against Women (CEDAW), “Concluding Observations on the Report of Myanmar Submitted under the Exceptional Reporting Procedure”; Sellers, “The Prosecution of Sexual Violence in Conflict: The Importance of Human Rights as Means of Interpretation.”
[66] Office of the Prosecutor, Situation in the People’s Republic of Bangladesh/Republic of the Union of Myanmar.
[67] UN Secretary General, “Guidance Note of the Secretary-General”; United Nations General Assembly, “Basic Principles and Guidelines on the Right to a Remedy and Reparation for Victims of Gross Violations of International Human Rights Law and Serious Violations of International Humanitarian Law.”
[68] International Law Commission, “Draft Articles on Responsibility of States for Internationally Wrongful Acts, with Commentaries”; International Court of Justice, “Reparation for Injuries Suffered in the Service of the United Nations, Advisory Opinion.”
[69] UN Committee on the Elimination of Discrimination Against Women (CEDAW), “General Recommendation No. 30 on Women in Conflict Prevention, Conflict and Post-Conflict Situations”; International Criminal Court, “Rules of Procedure and Evidence”; Redress, “Making Sense of Reparations at the International Criminal Court”; Correa, “Getting to Full Restitution: Guidelines for Court-Ordered Reparations in Cases Involving Sexual Violence Committed during Armed Conflict, Political Violence, or State Repression.”
[70] UN News, “Reparations for Sexual Violence in Conflict – ‘What Survivors Want Most, yet Receive Least’”; Gilmore, “Meeting the Needs of Victims of Sexual Violence through Reparations.”
[71] “We, the Rohingya, Can’t Wait for Justice from Faraway Courts”; “The International Court of Justice and the Rohingya”; Gorlick, “The Rohingya Refugee Crisis, International Justice, and Rethinking Solutions.”
[72] UN Special Rapporteur on the promotion of truth, justice, reparation and guarantees of non-recurrence, “The Foundation of the Mandate and the Importance of a Comprehensive Approach That Combines the Elements of Truth-Seeking, Justice Initiatives, Reparations and Guarantees of Non-Recurrence in a Complementary and Mutually Reinforcing Manner”; Bachelet, “Increasing Women’s Access to Justice in Post-Conflict Societies”; Tsai and Robins, “Strengthening Participation in Local-Level and National Transitional Justice Processes: A Guide for Practitioners”; Oosterveld, “Sexual and Gender-Based Violence in Post-Conflict Sierra Leone”; International Center for Transitional Justice, “When No One Calls It Rape.”
[73] Riley et al., “Systematic Human Rights Violations, Traumatic Events, Daily Stressors and Mental Health of Rohingya Refugees in Bangladesh.”