A child in Yemen and a child in Syria. Separated by hundreds of miles, they share the experience of warfare – in Syria, a conflict that has churned along for over six years, in Yemen, a war that’s intensified since 2015. Children in both countries share an uncertain future, with the ever-present specter of illness, trauma, and death.
Both countries are on the verge of a total collapse of their respective health systems. But this is not a byproduct of warfare. It is an intentional tactic utilized by parties to the conflict in both countries, emblematic of the deterioration of international laws and norms that are designed to protect hospitals and health care workers in times of war.
A Saudi-led intervention in Yemen has decimated civilian infrastructure, including medical facilities and personnel. The destruction of airports, roads, and ports has led to perilous shortages of medicine, equipment, and staff. Compounding the suffering, there have been at least 160 attacks on health professionals and hospitals in the past two years. Less than half of the country’s medical facilities are still functioning.
In Syria, that country’s government and its Russian allies have waged an all-out assault on the health care system, targeting hospitals and doctors in an effort to inflict maximum suffering in opposition-held areas. While opposition and Islamic State fighters are also complicit in hospital attacks, Syrian government forces and their Russian allies are responsible for more than 90 percent of the 454 medical facility attacks that Physicians for Human Rights (PHR) has documented since 2011.
We have documented these attacks on hospitals and clinics, doctors and medics, pediatric wards and maternity hospitals. The deliberate or reckless destruction of health care is a war crime with devastating impact. Not only do these strikes kill those who are trained to provide care in times of conflict; they also kill untold numbers of people who will die of preventable deaths without access to routine and emergency care.
In addition to bombing health facilities and personnel, parties to both conflicts have cut off supplies of food, medicine, and vital medical equipment. Since last August, Yemen’s main international airport has been closed and seaports have been attacked. Now the country is on the brink of famine, and health professionals are struggling to treat the injured and dying without sufficient medicine and supplies.
In January, one Yemeni doctor told Watchlist on Children and Armed Conflict that he sees patients who travel hundreds of miles, past checkpoints and along dangerous roads, because local hospitals have run out of blood, oxygen, and other critical supplies. “But it’s the cases of malnutrition we have seen,” he said, “where children are suffering the most.”
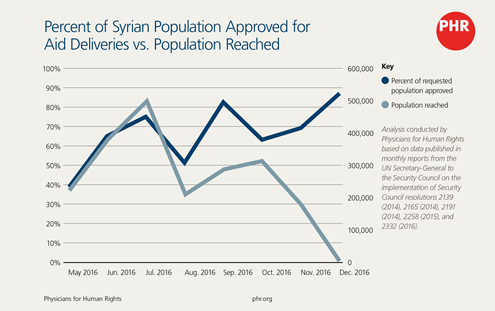
In Syria, too, life-saving aid has been intentionally blocked from reaching civilians, particularly in areas under siege. Last year, PHR documented dozens of preventable deaths from malnutrition and lack of medical aid in the besieged town of Madaya, including young children. After an April chemical weapon strike in the northern town of Khan Sheikhoun, where aid is in short supply, health professionals there didn’t have the necessary supplies to treat victims.
“After all these years, we have become accustomed to death,” a Syrian doctor told Physicians for Human Rights. “But when you see children injured, it is hard.” Indeed, in the hours after the attack, social media carried images of young children, struggling to breathe and foaming at the mouth.
“More than one member of our staff cried,” said the Syrian doctor. “We are always doing our best, but we couldn’t provide any help.”
A year ago today, the UN Security Council – unable to come to a consensus about how to stop the bleeding in Syria or Yemen – issued a resolution reasserting core tenets of international law: that medical personnel and facilities are protected and that humanitarian aid must flow freely.
Since that time, these attacks have continued with impunity. The pace is relentless, and accountability seems distant. Warring parties in both countries have powerful allies on the Security Council. Russia has not only covered for the crimes of Syria, Russian forces have also carried out these crimes alongside the Syrian military. Meanwhile, the United States and the United Kingdom have turned a blind eye to Saudi atrocities, fueled by American- and British-supplied weaponry.
The United Nations needs to lead the charge against these heinous attacks. The World Health Organization must systematically document strikes against medical facilities and personnel; the UN Security Council must convene regular briefings on conflicts experiencing such attacks; and the Security Council must mandate prompt, impartial investigations into all reported attacks to ensure that perpetrators will be held accountable for these egregious violations of international law.
An entire generation of Syrian and Yemeni children will carry the mental and physical scars of these conflicts. War crimes trials and transparency and naming and shaming cannot erase those wounds. But they will send a signal to those who act with an utter disregard for international law and human rights: the world is watching. And justice must come.