Press release available in English and Ukrainian.
Executive Summary
On February 24, 2022, the Russian Federation began its full-scale invasion of Ukraine. This act of aggression against a sovereign nation is a gross violation of international law, one that has been widely condemned by the international community. In the year that has followed, attacks on civilians and civilian objects have been a hallmark of the war, with violence against the Ukrainian health care system a prominent feature of Russia’s unlawful conduct. One notorious incident came only two weeks after the full-scale invasion began, when Russia’s air force bombed a maternity and children’s hospital in the city of Mariupol. The photograph of a heavily pregnant woman being carried from the hospital on a stretcher, who later died, together with her baby, became an early, stark example of the brutal, indiscriminate way in which Russia has waged its illegal war.
This report – a joint undertaking among eyeWitness to Atrocities (eyeWitness), Insecurity Insight, the Media Initiative for Human Rights (MIHR), Physicians for Human Rights (PHR), and the Ukrainian Healthcare Center (UHC) – documents the staggering toll that Russia’s aggression has had on Ukraine’s health care system since February 2022. Using 10 case studies and a joint dataset of attacks, this report shows how Russia appears to be violating international humanitarian law by deliberately and indiscriminately targeting Ukraine’s health care system as part of a broader attack on its civilian population and infrastructure. As the report details, the apparent targeting of the health care system is carried out through a variety of means, including: (1) attacks on health care facilities, (2) attacks on ambulances, (3) destruction of critical health infrastructure and theft of supplies, and (4) assaults, torture, and ill-treatment of health workers, including doctors, nurses, and paramedics.
For 35 days, Ukraine’s health care infrastructure was damaged every single day. In the first two weeks of the invasion, an average of four to five hospitals and clinics were attacked daily.
Targeting functioning health care infrastructure and workers in an armed conflict and carrying out indiscriminate attacks that affect civilian infrastructure – including hospitals and clinics – are war crimes. When committed as part of a state policy on a widespread or systematic basis, such attacks are also crimes against humanity. Based on the evidence gathered in this report, there is a reasonable basis to believe that attacks on Ukraine’s health care system constitute war crimes and comprise a course of conduct that could potentially constitute crimes against humanity as well. This evidence urgently warrants immediate investigation by prosecutorial authorities.
The broader impact of these attacks – in terms of the ability of the Ukrainian government to ensure the human right to access adequate health care – is equally devastating. While it is too soon to know the full extent of this war’s damage on Ukraine, a recent health needs assessment conducted by the World Health Organization (WHO) notes that “spiraling costs, logistical hurdles and damaged infrastructure are making access to essential services all the more challenging for growing numbers of civilians.”
This report breaks new ground by providing the most comprehensive documentation to date of attacks on Ukraine’s health care system as well as their devastating impact on the right to health. The report draws on a dataset of attacks – collectively developed from open-source and confidential information over the course of 2022 – supplemented by detailed case studies based on visits to hospitals in four different regions of Ukraine to inspect attack sites, assess damage, take photographs, and conduct semi-structured interviews with hospital staff who were present at the time of the attacks.
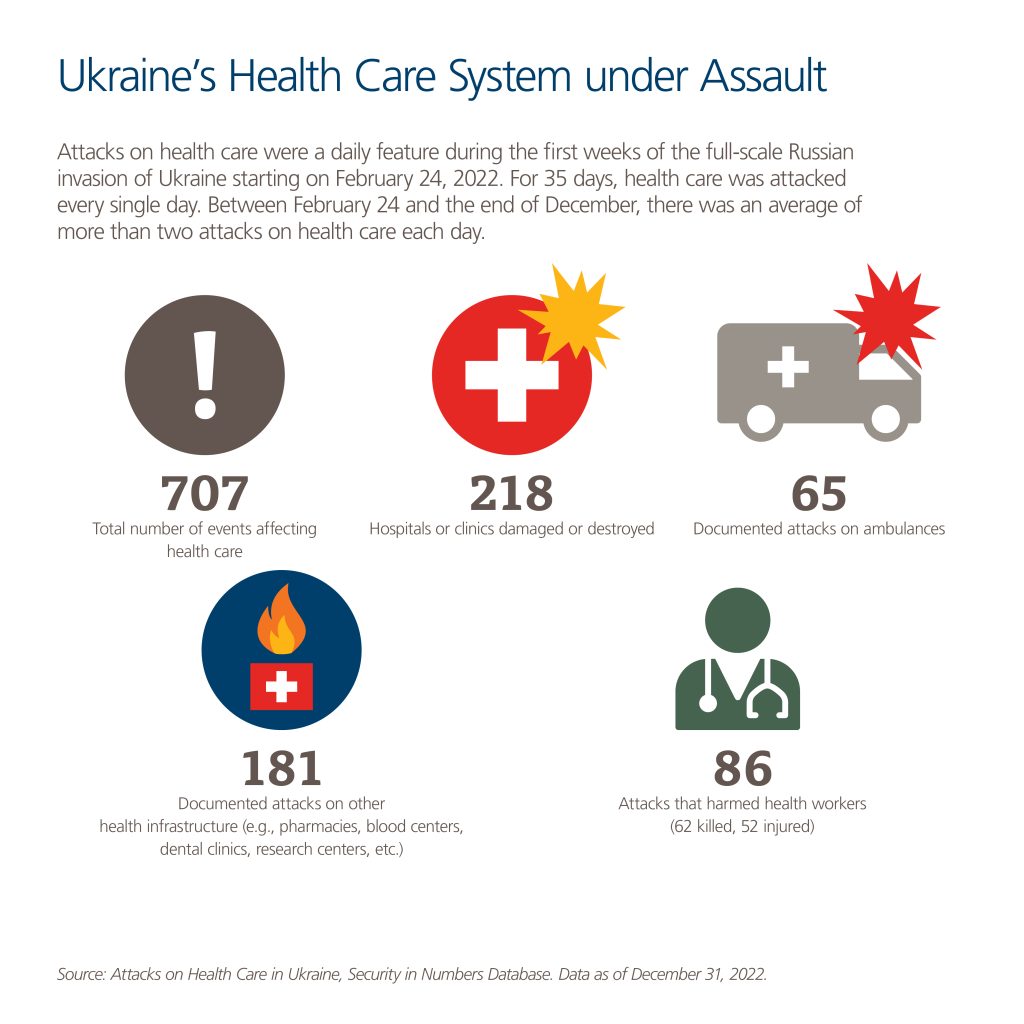
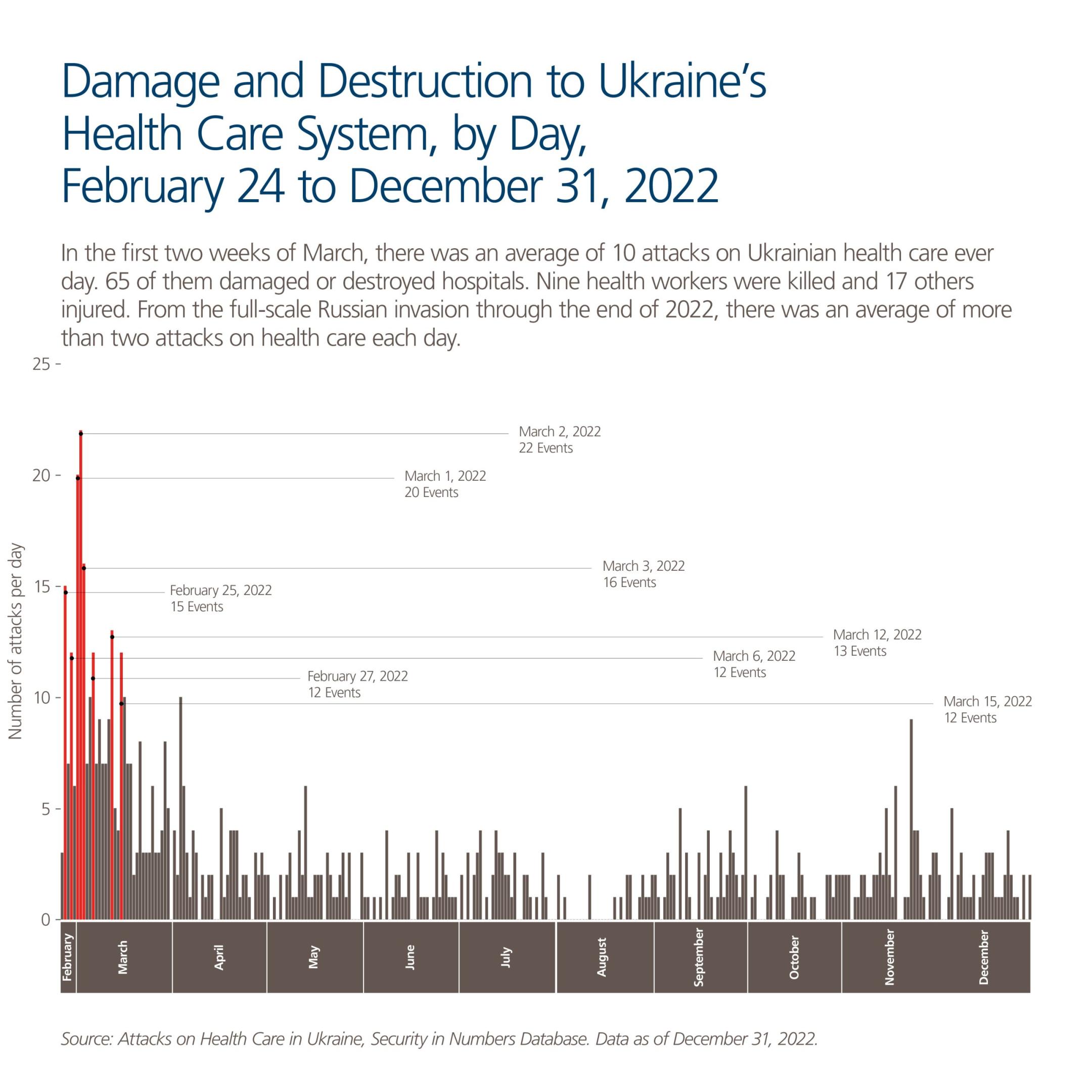
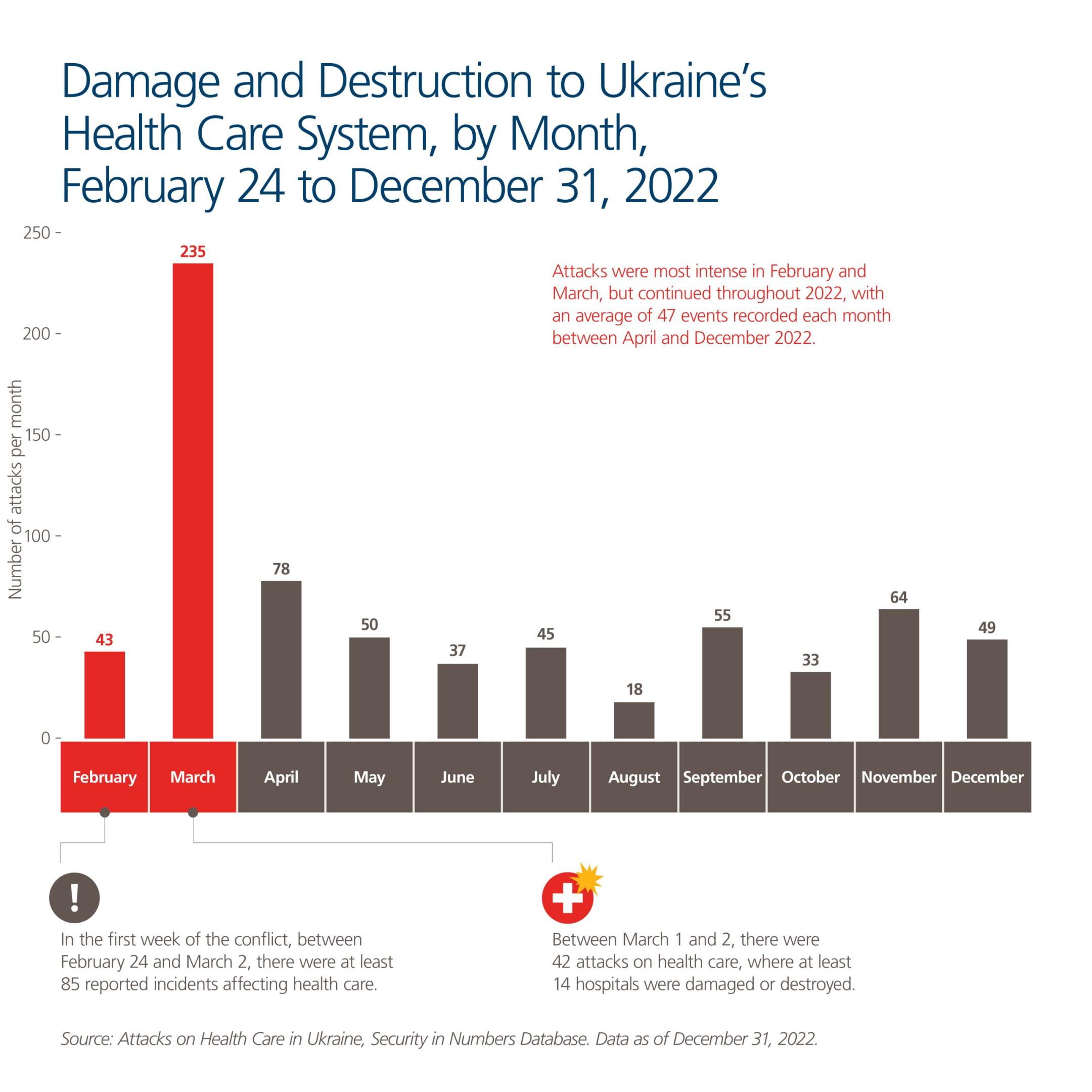
The findings are stark. During just the first weeks of the Russian full-scale invasion, there were constant, daily attacks on Ukraine’s health care system. For 35 days, Ukraine’s health care system was damaged every single day. Assaults were particularly intense in February and March; during the first two weeks of the invasion, an average of four to five hospitals and clinics were attacked daily. Attacks continued throughout the year, with 235 attacks on health care overall in March and an average of 47 attacks each month from April through December 2022. Over the entire period studied in this report (February 24-December 31, 2022), there was an average of more than two attacks on health care each day.
Targeting functioning health care infrastructure and workers in an armed conflict and carrying out indiscriminate attacks that affect civilian infrastructure – including hospitals and clinics – are war crimes.
Between February 24 and December 31, 2022, the research team documented a total of 707 attacks on Ukraine’s health care system.
- There were 292 documented attacks that damaged or destroyed 218 hospitals and clinics. Many health facilities were attacked more than once.
- There were 65 documented attacks on ambulances.
- There were 181 documented attacks on other health infrastructure (e.g., pharmacies, blood centers, dental clinics, research centers, etc.).
- 86 attacks on health care workers were documented, with 62 health workers killed and 52 injured. Many others were threatened, imprisoned, taken hostage, and forced to work under Russian occupation.
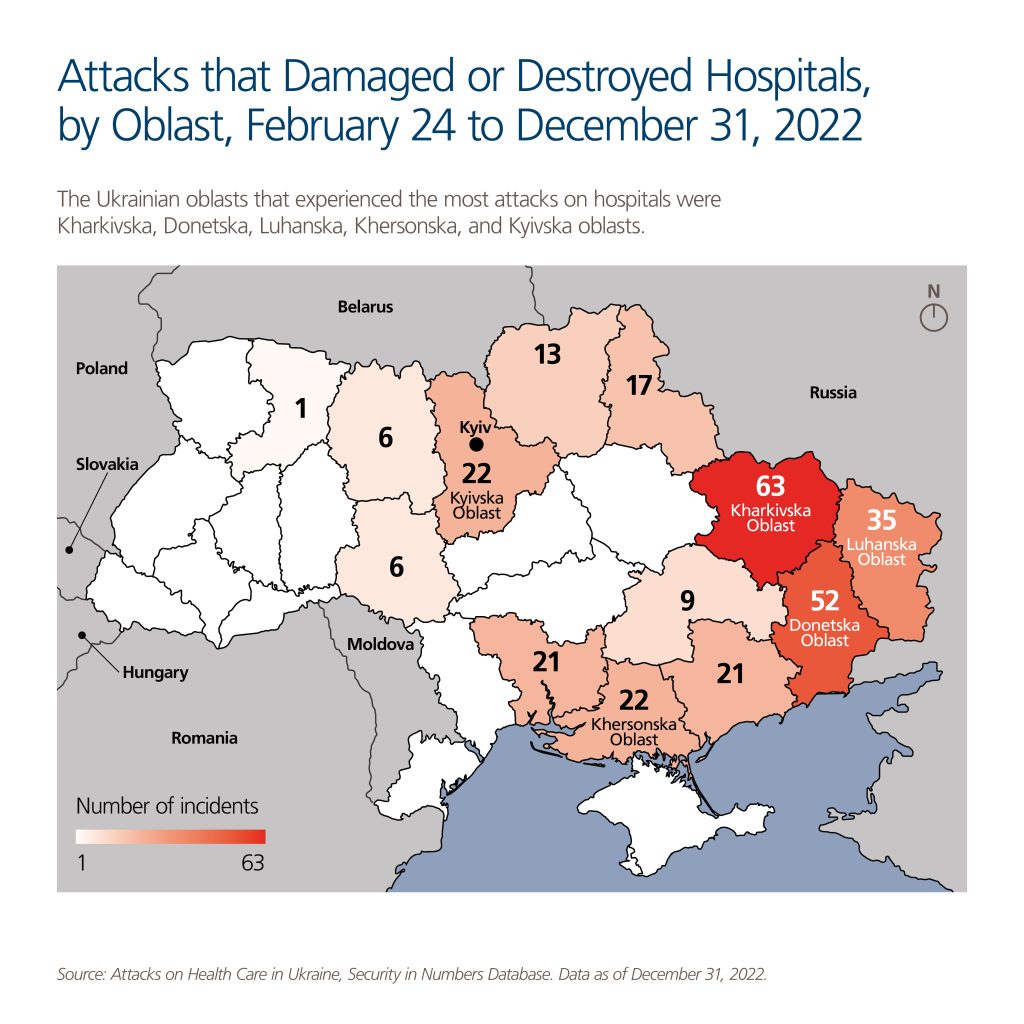
One out of 10 of Ukraine’s hospitals have been directly damaged from attacks, with the heaviest destruction in the eastern oblasts of Kharkivska, Donetska, and Luhanska, and also in Khersonska and Kyivska.
In some cities and towns, nearly all the health facilities were harmed in some way. In Mariupol, in the southern part of Donetska oblast, almost 8 out of 10 points of health care service provision, sites where medical assistance is available, were either damaged or destroyed.
“They saw very well, they knew that this was a medical institution.” “We hoped this would somehow save us. But it turns out nothing is sacred in this war.”
Dr. Alla Barsehian, director of Bashtanka Multiprofile Hospital, which was heavily damaged in an attack.
In the Makariv municipality – where three health facilities and 30 pharmacies have been damaged or destroyed – the scale of the attacks has led to the severe disruption of health services and infrastructure in the area.
In 10 oblasts, 48 hospitals were hit multiple times, underscoring not only the indiscriminate nature of attacks but also the possibility that they were deliberately targeted. For instance, the Severodonetsk City Multiprofile Hospital in Luhanska oblast was hit 10 times between March and May 2022. One hospital in Kharkivska oblast was hit five times, and another was hit four times.
Many hospitals bore internationally recognized symbols of their status as medical centers, which were clearly visible from the air. Bashtanka Multiprofile Hospital, which was heavily damaged in an April attack, was marked with a Red Cross painted on a white canvas placed on the roof.[1] According to Dr. Alla Barsehian, the Bashtanka Multiprofile Hospital director, drones flew over the facility and “they saw very well, they knew that this was a medical institution.”[2] “We hoped this would somehow save us. But it turns out nothing is sacred in this war.”[3]
The scale of these attacks underscores the broader destabilizing effects they have on Ukraine’s population, from reduced access to critical medications to severely restricted access to health care and vastly diminished vaccine rates. An International Organization for Migration survey found that, as of the beginning of December 2022, one in every three Ukrainians was experiencing the lack of medical services.
The Russian Federation’s continued aggression – leading to both targeted and indiscriminate attacks on Ukraine’s health care facilities, amongst other civilian infrastructure – constitutes a gross violation of international law. Russia must cease these attacks and end its aggression. Accountability for war crimes and crimes against humanity, as well as for the crime of aggression, will be critical; however, Russia is also obligated to make reparations for its breaches of international law, including compensating the Ukrainian state and individual Ukrainians – and other killed or injured nationals – for devastating loss of life and injury, extensive destruction, and the enormous costs of reconstruction. Because protecting health care is a shared responsibility of all parties to an armed conflict, all parties to the conflict must ensure compliance with international humanitarian law principles.
To other engaged actors, the report makes the topline recommendations below (full recommendations can be found starting on p. 82).
Selected Recommendations
To the International Criminal Court’s Office of the Prosecutor, the Prosecutor General of Ukraine, the Independent International Commission of Inquiry on Ukraine, and other National Prosecutors:
- Prioritize investigation of attacks on health care facilities and health care workers and commit resources to prosecuting cases specifically focused on these violations as war crimes and crimes against humanity.
To the Diplomatic Community, including Member States of the European Union, the United Nations (UN) Security Council, and the Organization for Security and Co-operation in Europe:
- Publicly condemn attacks on health care personnel and facilities in Ukraine, and urge compliance with the Geneva Conventions, Additional Protocol I, and UN Security Council Resolution 2286, including rules on medical impartiality.
- Continue to exert all available political, economic, and diplomatic pressure on the Russian Federation to immediately cease both indiscriminate and targeted attacks on civilians and civilian infrastructure, including on health care workers, facilities, and vehicles, as well as to withdraw from Ukrainian territory.
To the Government of Ukraine:
- Ratify the Rome Statute of the International Criminal Court and adopt domestic implementing legislation that sufficiently captures the substantive crimes and modes of liability provided for under the Rome Statute.
To the UN Human Rights Council and its Member States:
- Renew the mandate of the UN Independent International Commission of Inquiry on Ukraine on an open-ended basis and ensure robust funding and support for its continued functioning.
- Convene a thematic debate to address widespread and systematic attacks on Ukraine’s health care system and the need to ensure criminal accountability.

Introduction
On February 24, 2022, the Russian Federation began its full-scale invasion of Ukraine. This act of aggression against a sovereign nation is a gross violation of international law, one that has been widely condemned by the international community. In the year that has followed, attacks on civilians and civilian objects have been a hallmark of the war, while violence against the Ukrainian health care system has featured prominently in its conduct. One notorious incident came only two weeks after the full-scale invasion began, when Russia’s air force bombed the Women’s and Children’s Health Territorial Medical Association, a maternity and children’s hospital in the city of Mariupol. The photograph of a heavily pregnant woman being carried from the hospital on a stretcher, who later died together with her baby, became an early, stark example of the brutal, indiscriminate way in which Russia has waged its illegal war.
Critically, February 2022 was not the first Russian attack on Ukraine’s sovereignty, nor was it the first time it targeted the country’s health care system. Indeed, the current aggression stretches back to at least 2014, when, following the Revolution of Dignity that ousted Ukraine’s former president, Viktor Yanukovych, Russia moved to annex Crimea from Ukraine, and both supported and directed pro-Russian separatists in a long-running conflict in the country’s eastern, Donbas region.[4] As a 2019 study concluded, “healthcare infrastructure in the Donbas region has experienced significant degradation, with one-third or more of the large care facilities damaged as the result of combat operations.”[5]
Protecting health care is a shared responsibility of all parties to an armed conflict. International humanitarian law (IHL), which is the body of law that applies to armed conflicts, sets out detailed rules that seek to protect health care from conflict-related violence, principally by limiting the means and method of warfare. Health care facilities, providers, and ambulances are further afforded special protection under IHL so as to mitigate the impact of conflict on their work and ensure the delivery of care to the sick and injured. Beyond protection, however, there is a pressing need to ensure accountability when IHL rules and principles are violated.
This report documents the damage and destruction done to Ukraine’s health care system – including attacks on health care facilities and violence against health care workers – during the first year of Russia’s full-scale invasion. Drawing on detailed case studies and a joint dataset of 707 reported attacks, it shows how Russia appears to be violating IHL by deliberately and indiscriminately targeting Ukraine’s health care system as part of a broader attack on Ukraine’s civilian population and infrastructure. The database and case studies below show that, rather than Ukraine’s health care system being protected from the effects of Russia’s war of aggression, the system has been devastated by it. As the report details, the apparent targeting of the health care system is carried out through a variety of means, including: (1) attacks on health care facilities, (2) attacks on ambulances, (3) destruction of critical health infrastructure and theft of supplies, and (4) assaults, torture, and ill-treatment of health workers, including doctors, nurses, and paramedics.
Targeting functioning health care infrastructure and workers in an armed conflict and carrying out indiscriminate attacks that affect civilian infrastructure, including hospitals and clinics, are war crimes. When committed as part of a state policy on a widespread or systematic basis, such attacks are also crimes against humanity.
Building on the dataset and case studies, the legal analysis in the report’s final section offers a roadmap for investigators and prosecutors to build cases that focus on attacks on Ukraine’s health care system, in order to promote accountability for these crimes.[6] It shows that there is a reasonable basis to believe that attacks on Ukraine’s health care system constitute war crimes and comprise a course of conduct that could potentially constitute crimes against humanity as well. This evidence urgently warrants immediate investigation by prosecutorial authorities.
The broader impact of these attacks, in terms of the ability of the Ukrainian government to ensure the human right to access adequate health care, is equally devastating. While it is too soon to know the full extent of this war’s damage on Ukraine, a recent health needs assessment conducted by the World Health Organization (WHO) notes that “spiraling costs, logistical hurdles and damaged infrastructure are making access to essential services all the more challenging for growing numbers of civilians.”[7] Similarly, a recent report by the United Nations (UN) Human Rights Monitoring Mission in Ukraine notes that, “The extent of damage to educational and medical facilities directly impacts the enjoyment of the rights to health and education. Children, women in need of perinatal care and persons with vulnerabilities who require stable access to healthcare are particularly affected.”[8]
This report proceeds in three parts. The first outlines overall numbers of documented attacks on health care facilities and health care workers from February 24, 2022 to December 31, 2022, based on a dataset and interactive map that has been collectively developed from open-source and confidential information over the course of the year.[9] The early impact of these devastating, crushing attacks on Ukraine’s health care system, and their historical roots in other conflicts in which Russian forces have been engaged –Chechnya, Georgia, Syria – is also examined. The second part offers 10 detailed case studies that illustrate the kinds of attacks that have been perpetrated on hospitals, health care workers, and medical transport in Ukraine since February 2022. The final section outlines the legal framework for understanding how these attacks may constitute war crimes and crimes against humanity under international law, and then provides a broad overview of specific crimes that may have been committed, all of which require further investigation as part of a comprehensive, multifaceted approach to accountability. This includes: (1) enforcement through international criminal law as set forth in the Rome Statute of the International Criminal Court (ICC) (which has jurisdiction over international crimes committed in Ukraine); (2) a consideration of available charges under Ukrainian criminal law; and (3) the availability of prosecutions in third countries under the principle of universal jurisdiction. All three are critical, complementary avenues for criminal accountability.
The principle of equal application under IHL dictates that the law applies to all parties in an armed conflict; it binds both Ukraine and Russia. This report, however, focuses on the conduct of Russian forces over the course of 2022, because the scale and weight of available evidence point towards attacks perpetrated against Ukraine’s health care system in the course of Russia’s aggression. The authors are aware of reports of Ukraine allegedly not abiding by certain IHL obligations as well, for instance by failing to move civilians away from areas of fighting – including in the vicinity of hospitals – and a non-specific claim that hospitals were used as military outposts.[10] Investigation of violations of a duty to remove civilians from areas of fighting is beyond the scope of this report. Another claim is that Ukraine fired from health care facilities or otherwise used them for military purposes. Despite efforts, the authors have not seen or been able to obtain evidence of a hospital attack or misuse of hospitals for military purposes by Ukrainian forces.[11] If or when evidence points to unlawful conduct on the part of Ukrainian forces in relation to health facilities (or other protected sites), these incidents should similarly be investigated by relevant domestic or international authorities. Under IHL, if a health facility is being intentionally misused to gain a military advantage, the facility would lose its protection; however, as discussed further below, the attacker still has a duty to warn and to minimize harm to civilians.
The report does not identify individual suspected perpetrators among Russian forces. To do so would require the gathering of additional testimony, documentation, and other evidence, which will be incumbent upon the ICC and competent national authorities. A full investigation of this kind should expose the criminal accountability not just of perpetrators directly responsible for carrying out the criminal acts outlined in the report, but of those ultimately, as well as indirectly, responsible for designing, developing, pursuing, and instructing others to destroy and weaken Ukraine’s health care system.
Methodology
This report used a mixed-methods approach to document and legally analyze case studies of attacks on Ukraine’s health care system as well as the devastating impact these attacks have had on the right to health. It documents visible destruction to the health care system combined with witness testimonies and other reported descriptions of how the damage occurred in areas of Ukraine, where such information is available. Drawing on an incident dataset of attacks collectively developed by the authoring organizations and supplemented by the case studies, the report then analyzes these attacks for potential violations of international criminal law and Ukrainian criminal law. The events and data herein focus on the period from February 24, 2022, when Russia’s full-scale invasion of Ukraine began, to the end of December 2022.
The report draws on a range of sources: audiovisual evidence, open-source research, primary source interviews, and public reports from several international fact-finding bodies – including the Independent International Commission of Inquiry on Ukraine, established by the United Nations Human Rights Council in March 2022, the UN Human Rights Monitoring Mission in Ukraine, and the Moscow Mechanism of the Organization for Security and Cooperation in Europe – as well as non-governmental organizations.
Partner Organizations
This research is a joint undertaking among organizations based both inside and outside Ukraine, each of which shares an interest in ensuring the protection of health care in conflict and in ensuring compliance with international humanitarian law (IHL). Each brings a unique background to the collaboration:
eyeWitness to Atrocities, initiated by the International Bar Association in 2015, seeks to bring the perpetrators of atrocities to justice by providing legal and technical expertise in building photo and video dossiers that can be authenticated for use in criminal investigations or trials.
Insecurity Insight is a humanitarian to humanitarian (H2H) organisation that aims to elevate the voices of those affected by insecurity and to raise awareness of the impact of violence. Insecurity Insight has been monitoring violence against health care since 2008 and generates data for the Safeguarding Health in Conflict Coalition (SHCC) on attacks on health care. Its innovative data collection and analysis methods have generated insights relevant for aid workers, aid agencies, and those concerned with the protection of health workers, educators, internally displaced persons, and refugees.
Media Initiative for Human Rights (MIHR) advocates for Ukraine’s integration into the free world. Its main areas of activity are the investigation of war crimes committed in connection with the Russian aggression in Ukraine and advocacy to support compliance with and observance of human rights and freedoms.
Physicians for Human Rights (PHR) is a human rights organization that documents and seeks accountability for violations of human rights and other international crimes. It has a particular focus on protecting health facilities, workers, and volunteers providing medical assistance and care during conflict.
Ukrainian Healthcare Center (UHC) is a think tank based in Kyiv, Ukraine, providing consultancy, analytics, and educational services. Its core competencies include health system policy and governance, health economics and financing, and health system transformation. UHC began documenting attacks on health care in February 2022, after the large-scale Russian invasion began.
As organizations with presence in Ukraine, both UHC and MIHR served as the initial point of contact with Ukrainian health care professionals. As explained below, UHC’s monitoring of attacks on health facilities and existing contacts with many hospital staff and directors enabled the sharing of sensitive information and, in several cases, access to the health facility to undertake further interviews and analysis. Similarly, MIHR researchers were able to speak with medical personnel who were originally trapped in occupied territories of Ukraine but later managed to escape. These individuals trusted MIHR to share their experience through semi-structured interviews, which are described further in the report’s case studies.
Site Visits and Interviews
Between April and November 2022, UHC and MIHR researchers gathered first-hand accounts of attacks on health care in Ukraine, visiting areas that were accessible at the time of research. These included areas that were either initially the site of heavy fighting as part of the Russian offensive or were occupied by Russian forces but later liberated. UHC’s research teams visited hospital sites in four different regions of Ukraine now under the control of the Ukrainian government – Makariv (Kyivska oblast, May 23, 2022), Chernihiv (Chernihivska oblast, July 14-15, 2022), Trostianets (Sumska oblast, August 11, 2022), and Izium and Balakliia (Kharkivska oblast, November 18, 2022) – to inspect attack sites, assess damage, take photographs, and conduct semi-structured interviews with hospital staff who were present at the time of the attack.[12] During these months, MIHR researchers also interviewed several Ukrainian doctors and medics about their experiences providing health care during bombardment by Russian forces or under occupation. Three of these interviews – with health care professionals who managed to escape or were later freed from captivity – are recounted in detail.
This report’s methodology was approved by PHR’s Ethics Review Board (ERB) in order to ensure compliance with U.S. requirements for human subject research.[13] Accordingly, for all interviews, the research teams obtained informed oral consent from each subject after the subject received a detailed explanation of the five partner organizations, the purpose of the investigation, and the potential benefits and risks of participation. All interviews were conducted using a range of security precautions and protections. First, participants could stop the interview at any time or refuse to answer any questions. Audio recordings of interviews were only made with the explicit permission of the interviewee. Second, all images obtained by UHC or through the eyeWitness app – which has been used in Ukraine since 2017 to capture photos, video, and sound and to record metadata – are stored on secure systems owned by each respective organization. All interview files are stored on a secure, password protected file-sharing system to which only the partner organizations have access. Finally, while all health personnel interviewed for the report were spoken with after they had managed to escape occupied territories, the identities of several have been withheld upon their request to ensure their safety and anonymity. Subjects are only described in a manner that does not identify them or provide any identifying characteristics unless they specified that they wished to be identified. Interviews were conducted in Ukrainian and translated into English.
Dataset
To understand the scale and extent of attacks on health care, the report draws, in part, on an incident dataset that research partners developed over the course of 2022. The dataset brings together 707 individual incidents from a range of sources, including open-source research, the eyeWitness app, witness and victim accounts, site visits undertaken by UHC, and networks from organizations working on the ground. It has been compiled using an incident-based approach to evidence collection, where individual incidents are collected, verified, and combined to allow for an analysis of patterns of violence over time and in different locations.
The dataset follows Insecurity Insight’s standard data structure as developed for the Safeguarding Health in Conflict Coalition, of which it, PHR, and UHC are members. Insecurity Insight has been monitoring violence against health care since 2008 and generates data for the Safeguarding Health in Conflict Coalition on attacks on health care in all active conflicts. In March and May 2022, Insecurity Insight provided regular, near-time updates on reported incidents of attacks on health care in Ukraine.[14] In its monitoring of attacks, Insecurity Insight used established online data search methods, including both algorithms and manual searches; it then combined this information with confidential event contributions from long-term partner organizations to compile its dataset of attacks on health care in Ukraine.[15] This data can be visually explored in online interactive maps and downloaded from the Humanitarian Data Exchange.[16]
UHC’s data collection began as an effort to verify attacks reported by the World Health Organization (WHO) and the Ukrainian Health Ministry in March 2022. For each event, UHC followed a two-level verification protocol that was adapted from the Berkeley Protocol on Digital Open Source Investigations.[17] It included conducting open-source research of news reporting about an attack (including social media posts), consulting photographic or video evidence of damaged or destroyed hospitals, reviewing satellite imagery, and/or speaking with witnesses to an incident. This included, in some cases, interviewing representatives from the affected hospitals by phone or in person to confirm the attack and the level of damage the facility sustained.[18]
For this report, the research teams undertook a cross-checked merger of UHC and Insecurity Insight’s previously independent datasets, reconciling any identical attacks, to create a unified online documentation of attacks on Ukraine’s health care system, including health care facilities and personnel.[19] All incidents were then reviewed and verified based on a range of criteria within the limits of research partners’ technical and resource capacity.[20] The merged dataset follows the WHO’s definition of attacks on health care: “any act of verbal or physical violence, obstruction, or threat of violence that interferes with the availability of, access to, and delivery of curative and/or preventive health services.” [21]
Map
Accompanying the release of this report is the launch (in English and Ukrainian) of an online, interactive map – located at www.attacksonhealthukraine.org – of documented attacks on health care perpetrated in Ukraine since the onset of the February 24 invasion. Whereas this report reflects data current as of December 31, 2022, the map and dataset will be continuously updated into the future. The map complements the report, however, as it provides a visual depiction of the scale and widespread nature of the attacks on Ukraine’s health care system described herein; it also highlights apparent patterns in the types of attacks and where they were committed relative to the broader history of Russia’s invasion. All of the case studies detailed herein are included on the map, as are the overall numbers of attacks discussed in the following section. The map also includes additional information on other conflict-related incidents that affected Ukraine’s health care system (e.g., the death of health care personnel by attacks perpetrated outside the course of their professional duties), but which are not further discussed here.
The images for the accompanying map were captured by or shared with UHC (with the informed consent of the individual who took the picture) or provided using the eyeWitness to Atrocities app, which has been actively used in Ukraine since 2017. To date, users of the app have captured and uploaded to the eyeWitness server more than 30,000 photos, videos, and audio recordings from across Ukraine. The app enables users to capture material and uses the device sensors to record metadata (such as GPS, nearby cell towers, and/or nearby Wi-Fi networks) that helps to authenticate the date, time, and location of the images and sound.[22] All users of the eyeWitness app have granted consent for the use of photographs contained in this report and the accompanying map.
Limitations
The report focuses on traceable evidence connecting attacks on Ukraine’s health care infrastructure to Russian forces. The numbers shown on the map and presented in the dataset provide a minimum estimate of the conflict damage to the health care system in Ukraine in 2022; however, they are likely an undercount. Like any other incident data collection, this dataset suffers from selective reporting, insofar as it depends on those who first reported an attack. Events may be captured or ignored for a range of reasons, including lack of access, lack of knowledge, disruption of Internet connection, or simple errors of omission. Specifically, incidents that occurred in territories directly or previously occupied by Russia are infrequently or rarely reported, resulting in an underrepresentation of the scale of violence in some of the Russian-occupied areas of Donetska and Luhanska oblasts and other, adjacent territories. There is also a possibility of bias in the reports as a result of mistaken perceptions and/or partiality toward Ukraine that could lead to exaggeration or inferences that might not be warranted by the evidence. It is possible that information about Ukrainian attacks on health facilities will come to light in the future, but no such information was available during the period of data collection.
The dataset therefore likely covers incidents in certain locations – and certain types of incidents – more systematically than others. The authors have relied on multiple sources whenever possible to address this potential bias. However, the authors were not able to obtain some underlying incident data that has been collected by others. The WHO has released the total number of attacks on health care in Ukraine it has collected and published information on aggregated number of attacks by oblast, but it does not publicly share information about particular incidents beyond the date, victims, and whether explosive weapons were used.[23] Without this information, it was not possible to determine whether the WHO had evidence of attacks beyond those in the database, nor to learn the nature and location of incidents it found.[24]
In addition to these monitoring limitations, situational constraints also posed limits to the ability to conduct physical documentation of attacks on the ground. For this reason, while research teams were able to speak with health personnel who had escaped occupied territories or travel to some regions that had been previously occupied by Russian forces later in 2022 to provide corroboration or confirmation of incidents, they were unable to access regions that remain occupied or where active conflict is ongoing.
Overview and Impact of Attacks on Ukraine’s Health Care System
From February 24 to December 31, 2022, partner organizations documented a total of 707 attacks on Ukraine’s health care system. These include:
- 292 attacks on health facilities (hospitals and clinics), which damaged 186 facilities and destroyed 32. Of the 218 facilities that were damaged or destroyed, 48 were affected by attacks more than once. Assaults were particularly intense in February and March; in the first two weeks of the full-scale invasion, an average of four to five hospitals and clinics were attacked daily.
- There were 65 documented attacks on ambulances, in which 40 ambulances were damaged.
- There were 181 documented attacks on other health infrastructure (e.g., pharmacies, blood centers, dental clinics, research centers, etc.).[25]
- 86 attacks on health care workers, which killed 62 and injured 52. Many attacks impacted more than one health care worker.

The 707 total also includes a range of additional incidents which meet the World Health Organization’s (WHO) definition of attacks on health, including looting, denial of access to health care, disruption of access to utilities (water and electricity) and causing serious impacts on patients, such as having to move them out of formal care structures in order to protect them.
Attacks on health care were a daily feature during the first weeks of the Russian full-scale invasion. For 35 days, Ukraine’s health care infrastructure was damaged every single day; there were 235 attacks in March alone. Attacks continued throughout the year, with an average of 47 attacks documented each month between April and December 2022. Over the entire period studied in this report (February 24-December 31, 2022), there was an average of more than two attacks on health care each day.

Attacks on Hospitals
With 218 hospitals reported damaged or destroyed, one out of 10 of Ukraine’s hospitals have been directly damaged from attacks.[26] As the map below clearly shows, the destruction is most marked in the east of the country. In some cities and towns, nearly all the health facilities were affected in some way. According to the Ukrainian Healthcare Center (UHC), in Mariupol and the southern part of Donetska oblast, almost 8 out of 10 points of health care service provision – sites where medical assistance is provided – were either damaged or destroyed. The oblasts that experienced the most attacks on hospitals were Kharkivska, Donetska, Luhanska, Khersonska, and Kyivska.
Multiple Attacks on the Same Hospitals
In 10 oblasts, 48 hospitals were hit multiple times, underscoring not only the indiscriminate nature of attacks but also the possibility that they were deliberately targeted. For instance, the Severodonetsk Multiprofile Hospital in Luhanska oblast appears to have been hit 10 times between March and May 2022; a hospital in Kharkiv was hit five times, another, in Kharkivska oblast, was hit four times.

Attacks on Health Care Workers
In 2022, the course of the Russian invasion killed at least 62 health workers in Ukraine and injured least 52. While this is likely an undercount, it is an important indication of the scale of the impact on the health system. Moreover, at least eight health workers were injured from the conflict violence outside of work, highlighting the broader impact of the war on the Ukrainian health care system, even when not the result of direct attacks on health.
The conflict has also diminished Ukraine’s health care workforce. Mass displacement of specialist care professionals has resulted in severely understaffed facilities and a risk of burnout for the remaining staff. Communities have resorted to online consultations with doctors who fled to the western part of Ukraine or abroad.[27] Notwithstanding valiant efforts by the WHO, NGOs, Ukraine’s Ministry of Health (MoH), facility managers, and health care staff to maintain quality health care and service delivery, in some places it has suffered. A lack of running water and electricity in some facilities caused by conflict damage has compounded this problem.
Indirect Attacks on Ukraine’s Health Care System
Other attacks on Ukraine’s health system which are beyond the scope of this dataset include:
- Infrastructure damage has led to direct losses of raw materials for medicines, along with losses in manufacturing, storage, and distribution capacities, and delays in manufacturing and distribution.
- A large number of attacks on Ukraine’s energy infrastructure have affected the ability of health facilities – ranging from hospitals to retail pharmacies – to remain operational.
Estimated Damage and Loss
All of these attacks have caused widespread and costly damage. As of August 2022, according to the World Bank, the Ukrainian government, and the European Commission, the direct damage to Ukraine’s health sector was estimated at US$1.4 billion. [28] This represents the monetary estimate of the cost of destroyed and damaged health infrastructure included in the inventory of damage that Ukraine’s MoH compiles. It is likely that the actual level of damage is higher, however, given incomplete reports about damaged facilities located in territories temporarily not under Ukrainian government control and other private sector facilities. In addition:
- The estimated further losses from attacks on health are upwards of US$6 billion, which includes the removal of debris and demolition from destroyed health facilities, loss of income of private providers, losses from the financing of facilities that have not been fully operational during the war, and additional losses incurred by the population’s waning health.
- According to WHO, the European Union Delegation to Ukraine, the U.S. Agency for International Development (USAID) Mission in Ukraine, and the World Bank, the overall needs of Ukraine’s health sector are estimated to be US$15.1 billion (equivalent to almost three times the annual public spending on health) in order to cover accumulated infrastructure damage as well as the need to rapidly scale up critical health services.[29] This amount includes the cost of building new infrastructure using a “building back better” approach and the immediate recovery of facilities that were partially damaged. It also includes a significant expansion of rehabilitation and mental health services in Ukraine, which, as discussed below, will need to be scaled up to address the impacts of the war.
Explosive Weapons
Explosive weapons were reported in 89 percent of all incidents of damaged and destroyed health infrastructure (414 of 464).[30] The majority of health care objects appear to have been damaged through ground-launched explosives (including sea-launched missiles and mortars), such as shelling by conventional artillery, Multiple Launch Rocket Systems or mortars, rather than missiles, piloted-aircraft drop bombs, or those launched/dropped from drones. In total, 257 events causing damage to health infrastructure were attributed to ground-launched explosives in 14 oblasts. As a result, 120 hospitals and clinics were damaged and 25 were destroyed.
Ground-launched attacks on hospitals occurred in situations where tanks and other vehicle systems were used to shoot at health facilities from a relatively short distance. In these instances, the soldiers firing these weapon systems would have clearly seen the building they were targeting. If hospitals and other health facilities were clearly marked, they would have been aware that they were targeting a hospital. While it cannot be excluded that some health infrastructure, in particular warehouses or administrative buildings, may not have been clearly identifiable as such (and that Ukrainian forces may have been inside or nearby some health facilities that came under attack), the extent of damage they sustained through short distance ground-launched weapons systems strongly suggests that these attacks were intentional.
Air, sea, and ground-launched long-distance missiles and rockets have damaged health care infrastructure across a wide expanse of Ukrainian territory. These weapon systems have often been fired over several hundred kilometers. Both the weapon systems and the long distance over which they were fired makes it highly unlikely that the weapon systems were capable of accurately targeting and of avoiding wide-area effects around any potentially intended target. Such weaponry thus caused widespread indiscriminate effects in densely populated areas and among vital civilian infrastructure. Indeed, many incidents of reported damage to health facilities were due to the wide area effects of the explosive weapons, rather than from direct hits. To that end, the extent to which long-range ground missiles have been fired at cities and towns suggests that the Russian command pursued a military strategy of targeting civilians and civilian infrastructure, including health care. Indeed, Russian President Vladimir Putin explicitly admitted that Russia was targeting civilian infrastructure in a December 8, 2022 speech.[31]
In addition to ground-launched explosives, the dataset includes 35 incidents (out of the total of 464) where Russian airstrikes apparently used piloted airplanes in attacks that damaged or destroyed health infrastructure in 10 oblasts. Piloted air strikes were common during the initial weeks of the full-scale invasion in March, during which time 21 of these 34 recorded piloted air strikes took place. Air strikes continued to occur around contested cities, such as on December 21, 2022, in the Zaporizka oblast.
Air dropped bombs were recorded from Chernihivska, Donetska, Kharkivska, Kyivska, Luhanska, Mykolaivska, Sumska, Vinnytska, Zaporizka, and Zhytomyrska oblasts. In some instances, more than one hospital was hit during a single attack (see map above).
When aircraft pilots carry out air strikes, they would normally be able to identify larger and clearly marked hospitals, allowing them to distinguish between military and civilian health infrastructure if using so-called “precision guided” weapons. However, the majority of piloted Russian airstrikes have used so-called “dumb” or “iron” bombs that are released by the pilot after reference to a visual cue on the ground seen through a sight mounted in the cockpit. These bombs cannot be controlled once released and do not allow for variations or errors in altitude, airspeed, atmospheric pressure, temperature, precipitation, humidity, or wind – all of which can affect the trajectory of a bomb once released.[32]
While genuine mistakes cannot be excluded and some health facilities may not have been easily identifiable – and pilots will have been under high levels of stress, potentially causing them to target incorrectly – the extent to which Ukraine’s health facilities were damaged through air-dropped bombs suggests that pilots had likely been instructed to hit civilian infrastructure without regard for the fact that there may have been protected facilities in the areas being targeted.
Patterns of Attacks in Previous Conflicts
The patterns of Russia’s attacks on health care facilities in Ukraine are consistent with historical patterns as well. For instance, Physicians for Human Rights (PHR) documented how the Russian military attacked health facilities and workers in Chechnya as part of a relentless crackdown on the civilian population over the course of 2000 during the longstanding conflict there.[33] Similar reports later surfaced during the Russian-Georgian war in 2008, where medical facilities and personnel also came under attack. In a 2008 statement, the Georgian Medical Association reported that Russian armed forces had attacked an emergency hospital in Gori, severely injuring a doctor who was providing medical assistance at the time. Levan Labauri, the association’s then-secretary general, said that doctors had been “working under the permanent air attacks of Russian jets, even in the capital city Tbilisi. Some of our physicians [have been] killed and severely injured and hospitals destroyed. It is a really catastrophic situation.”[34]
In Syria, PHR has extensively documented at least 601 attacks on 400 health care facilities since the Syrian conflict began in March 2011.[35] In total, Syria and its Russian allies, who entered the conflict in 2015, have carried out 90 percent of all attacks on health targets (542 attacks), including the killing of 831 health workers.[36]Notably, the rate of attacks on hospitals increased by 62 percent between 2015 and 2016, following Russia’s entry into the conflict, compared to the period between 2012 and 2014. Indeed, in 2015 and 2016, PHR recorded the highest number of annual attacks on health care attributed to the Syrian government and Russia.[37]
The apparent existence of Russia’s policy to attack the Ukrainian health care system as a means of attacking the civilian population cannot be viewed in isolation from its pre-2022 conduct – even in Ukraine. From 2014, Ukrainian citizens living in Crimea without residency permits or Russian passports lost access to public health care,[38] and, since the onset of the full-scale invasion, the Crimean local population is reportedly being denied access to hospitals, which are reserved for wounded Russian soldiers.[39] Similarly, between 2014 and 2017, damage to health care facilities in the Donbas region has been described as “devastating beyond what was generally known.”[40] Researchers, for instance, determined that “over one-third (102) of the hospitals and clinics were damaged or destroyed [during that period], with over three-quarters of those attacks occurring during the period of heaviest fighting” between mid-2014 and early 2015.[41] The widespread use of largely indiscriminate weaponry was likewise noted as a contributor to the scale of damage during this period. A 2017 report of the Safeguarding Health in Conflict Coalition further found “that checkpoints and roadblocks, or conflict lines, impede[d] access to health care for one-third of households in conflict-affected areas in the east of [Ukraine], with dire implications for the 50 percent of families in the region that have members suffering from chronic diseases.”[42]
Impacts of Attacks on the Health of Ukraine’s Civilian Population
The health care facilities and infrastructure detailed above are all critical to ensuring the sustainable functioning of a complex health system. Beyond the direct damage and destruction perpetrated on the health care system, however, there is the broader impact that these attacks have on the right to health. Indeed, notwithstanding the resilience of Ukraine’s entire health care sector and the significant international support that has been provided, the scale of these attacks underscores the broader destabilizing effects they have on the country’s population, from reduced access to critical medications to severely restricted access to health care and vastly diminished vaccine rates. Some of these early indications since the onset of the February 24 invasion are highlighted below:
Diminished Access to Care. Damaged or destroyed health care infrastructure have left entire communities in Ukraine without access to essential services.
- In Mariupol, about 80 percent of health care infrastructure has been destroyed. In small and medium size communities – Izium (Kharkivska oblast), Balakliia (Kharkivska oblast), Makariv (Kyivska oblast) – hospitals are able to provide only a small segment of essential care, forcing patients to travel long distances to get it or to refuse to seek care at all. These communities are discussed further in the case studies below.
- An International Organization for Migration survey found that, as of the beginning of December 2022, one in every three Ukrainians was experiencing the lack of medical services. Most of the affected populations are concentrated in the southern part of the country.
Moreover, residents from areas not under Ukrainian government control or regions still experiencing active hostilities were significantly less likely (38 percent) to seek health care for a chronic disease than residents of Ukraine’s other regions (53–56 percent). In addition, there have been numerous reports from temporarily occupied areas about hospitals being used to treat Russian soldiers, while Ukraine’s civilian population is denied care.[43]
Reduced Vaccination Rates. Ukraine’s MoH reported a dramatic drop in routine vaccination rates since the onset of the full-scale Russian invasion, as health facilities struggle to meet pre-2022 rates. Lower vaccination rates create the risk of potential outbreaks of polio, measles, diphtheria, and other vaccine-controlled diseases.
- The Public Health Center (PHC) of the MoH reports that at the midyear, of all children under one year of age, only 29.7 percent received shots against tuberculosis; 23.1 percent against viral hepatitis B; 33.9 percent against diphtheria, tetanus, and pertussis; and 33.3 percent received polio vaccination doses. The PHC predicted that Ukraine would reach only about 60 percent coverage by the end of 2022, which is far less than what is needed for effective population protection.[44]
- Ukraine experienced a polio outbreak in the fall of 2021: 22 cases of polio were registered and a national polio control plan was enforced in February 2022 with the aim to boost vaccination in regions at risk. However, the Russian full-scale invasion halted the campaign and now, the possible repercussions of the continued outbreak are unclear.[45]
- The overall COVID-19 vaccine coverage has remained almost unchanged compared to the pre-war level of about 37 percent of the fully vaccinated population. Over the course of 10 months (from February 22, 2022 to January 9, 2023), only 522,339 first doses of COVID-19 were administered in Ukraine: this comprises about one percent of the population. Only 0.5 percent of Ukraine’s general population has received the second dose of the vaccine (237,551 doses administered). In total, since February 24, 2022, approximately five percent of Ukraine’s population has received a booster shot.[46]
Diminished Ability to Manage Chronic Disease. According to the International Organization for Migration, internally displaced persons in Ukraine most often reported they had stopped taking medication for high blood pressure and cardiovascular diseases. The WHO has reported that the types of medicines most frequently cited by respondents as difficult to obtain were medication for high blood pressure and for heart conditions (49 percent each).
Based on UHC’s independent analysis of Ukrainian government-funded prescriptions in 2022, there was a significant drop in the intake of the top three government-reimbursed medications in the first quarter of 2022. The top cardiovascular conditions’ drug (Bisoprolol) intake dropped by 34 percent compared to the similar period the previous year, the main type 2 diabetes medication (Metformin) dropped 27 percent, and the main asthma drug (Salbutamol) fell by 57 percent.
Growing Financial Barriers. Ukraine’s dramatic gross domestic product decline (about 30 percent in 2022) and high inflation suggest a looming health-related financial burden and threaten to impoverish a significant share of Ukraine’s population.
- Out-of-pocket health spending is high in Ukraine (about 51 percent of total health spending in 2019), meaning that there is a high risk of reduced affordability of health care, especially for essential medicines.
- According to a WHO survey, the main barrier (53 percent) to accessing health services reported by respondents’ households was the cost of medicines/treatments.[47]
- As of early December 2022, almost one-fifth of Ukraine’s population (17 percent) reported insufficient access to health care services and medication. The most common barrier for both was lack of funds to buy medicines or cover services needed.[48]
Worsening Mental Health. Russia’s invasion has caused a substantial increase in psychological harm and distress for all segments of Ukraine’s population. Mental health disorders, including a high prevalence of depression, alcohol use disorder, and suicide, were already the second leading cause of disability in the country, affecting up to 30 percent of the population.[49]
- Now, almost 10 million people could be potentially at risk of mental disorders such as acute stress, anxiety, depression, substance use, or post-traumatic stress disorder.[50]
- Notably, this figure excludes Ukraine’s growing veteran population: as of May 2022, the future number of veterans was estimated at five million, a more than five-fold increase from pre-war levels.[51] Veterans experience mental health disorders, post-traumatic stress, and other metal health issues at vastly disproportionate rates compared to the civilian population.

Case Studies of Attacks on Ukrainian Health Care
The 10 case studies below detail alleged attacks by Russian forces on Ukraine’s health care facilities, infrastructure, and workers in the conduct of the full-scale invasion of Ukraine. Several of these attacks were perpetrated in February and March 2022, as Russian forces encircled or occupied cities like Izium, Chernihiv, Trostianets, and Mariupol as part of the first phase of its full-scale invasion.
1. Attacks on Health Care Facilities
Siege warfare, bombardment, and the use of indiscriminate weapons have characterized Russian offensives in Ukraine, particularly urban areas with high civilian populations. Attacks on hospitals have appeared, in many cases, to be the result of widespread attacks on civilian areas, in which health care facilities – like other civilian objects, such as schools, residential dwellings, and places of worship – were part of a broader disregard for certain core international humanitarian law (IHL) principles relating to civilian protection: distinction, the prohibition on indiscriminate attacks, proportionality, and precaution. In addition, evidence suggests that some attacks are also part of a deliberate effort to attack health care facilities, meaning that the intention of Russian forces has been to target these facilities.
Case Study #1
Izium Central City Hospital (Kharkivska oblast)
Izium is a town of about 50,000 inhabitants split into two by the Siverskyi Donets River and connected by three bridges. The town center is located on the southern bank, hosting essential infrastructure such as administrative buildings and educational and medical facilities. On the northern bank are blocks of private residential buildings. The town’s location is strategic:[52] it stands on the M03/E40 highway connecting Kharkiv and the Sloviansk-Kramatorsk agglomeration (the administrative center of the Ukraine-controlled portion of the Donetska oblast) and on the P-79 road to Kupiansk in the north (another important transport hub) and Dnipropetrovska oblast in the southwest.
Following the capture of Kupiansk (on February 27, 2022) and Balakliia (on March 2, 2022; see Case Study #7) by Russian forces, Izium experienced heavy bombardments and was cut off from electricity, water, and mobile communications.[53] On April 1, 2022, Russian forces managed to occupy the town.[54] Izium remained under occupation until its liberation by Ukrainian forces on September 10, 2022.[55] Atrocities committed during the occupation have since come to light, including extensive destruction of civilian infrastructure and mass killings.[56]
The Izium Central City Hospital, located south of the river in the town’s city center, is a public, nonprofit hospital founded in 1822. Situated on the highway connecting Kyiv-Kharkiv-Dovzhanskyi, it had been designated as a roadside hospital to provide emergency care.[57] Prior to February 24, 2022, the hospital provided inpatient care in surgical, internal medicine, trauma, pediatric, infectious, and gynecological departments.[58] The hospital contained 220 beds, with the outpatient department additionally able to treat over 450 patients per shift.[59] In 2021, a CT scanner was installed, allowing tests to be conducted every day, at all hours.[60]
The Izium Central City Hospital was damaged on several occasions and struck directly at least once in March 2022. On the night of March 2 to March 3, an airstrike attributed to Russian forces by the Izium District Prosecutor[61] hit a high-rise building and a private house,[62] killing at least eight people, including two children,[63] and inflicting severe damage to the city center where the hospital is located.[64] The police department of the National Security Service of Ukraine – which is located less than 250 meters away from the Izium Central City Hospital – was reportedly the target of the strike.[65]
Dr. Bohdan Berezhnyi, a surgeon and medical director of the Izium Central City Hospital who lived at the hospital from February 25 until March 12, 2022, told UHC:
“[There was a] roaring sound and [distant] explosions…. Everyone asked me what to do, whether to go to the basement…. I opened the window, the entire sky was roaring, something flew away … and then I saw a bright explosion, a fireball in front of me. I crouched behind the windowsill, and the door behind me had been blown away.”[66]

On March 6, 2022, Ukraine’s Ministry of Defense reported that two of Russia’s battalion tactical groups failed to seize the town of Izium, instead firing on the city center with artillery systems and carrying out air raids.[67] Russian forces failed at another reported attempt to seize Izium on March 7 and continued to shell the civilian homes and infrastructure.[68] Dr. Berezhnyi also recalled that “[s]ometime on the 6th or 7th, the ‘Grads’ … flew over us. Of course, we immediately hid in the basement. On the 7th, aviation also was flying during the day, and it did also so very low, it was foggy.”[69] That day, Volodymyr Matsokin, deputy mayor of Izium, reported the “most extensive destruction since the Second World War.… Schools and hospitals were damaged.”[70]
As Russian forces retreated on or around March 7,[71] Ukrainian forces preventively blew up all bridges connecting the north of Izium, occupied by Russian forces, and the south of the town, “controlled by the Armed Forces of Ukraine and the Territorial Defense Forces of Izium.”[72] The bridges would have been considered strategically important both for Russian and Ukrainian forces: they were a key crossing for Russian forces to move to the southern bank and occupy the city center of Izium, and were also important for Ukrainian defensive efforts, particularly to move forces, equipment, and ammunitions.[73]
According to Dr. Berezhnyi, on March 7, 2022, the only time Ukrainian forces came to the hospital was after blowing up the bridges: “We gave them tea and coffee, they stayed with us for two hours, and then they left. That’s all. After this, the connection with the military was that they brought their wounded from time to time.”[74] He added, however, that Ukrainian forces were based in a building nearby – perhaps the city council (located about 500 meters away from the hospital) – and that a Ukrainian armed personnel carrier often transited on a road nearby after the bridges were blown up.[75]
On March 8, 2022, the deputy mayor of Izium and the media reported on a strike that directly hit the hospital.[76] According to local authorities, the hospital was hit by Russian shells.[77] Part of the main building was destroyed, including the intensive care unit, the entrance to the emergency department, and the operating block,[78] and the heat, water, and electricity supplies were cut off as a result.[79] Volodymyr Matsokin described patients climbing out “from under the rubble as they could.”[80]

Dr. Berezhnyi recounted:
“[On] maybe the 7th or 8th [of March], there was an incoming at this annex.… It hit the corner in the operating room and broke the wall; we understood we needed to evacuate everything, evacuate the equipment into the basement, [we] brought what we could to the basement, and discharged patients.… And then, on [March] 8th or 9th … it came at the main building; it had been blown apart by the explosion… It hit in the night on the fourth floor, and everyone in the basement … we got scared because the elevator collapsed from the fourth floor right into the basement…. So, in general, we lost the operating room and the intensive care. And we understood that in case something happens, we can do nothing.… We understood it will flood with patients, wounded … and what [can we do]?[81]
In the days that followed, town residents were evacuated en masse through “green corridors” under shelling.[82] Dr. Berezhnyi managed to leave the town on the evening of March 12, 2022.[83]
Satellite imagery dated March 12[84] and March 24[85] depict severe damage to the hospital’s main entrance as well as the destruction of most infrastructure around the hospital, including the Lyceum #4 building about 200 meters away, a large crater in a sport field 170 meters away, and a destroyed bridge less than 300 meters away from the hospital. The hospital also showed signs of other types of damage, including limited traces of shrapnel damage on the hospital façade.[86] According to a weapons analyst, the extent of the damage makes it likely that large conventional artillery rounds or unguided aerial bombs damaged the hospital and that the traces on the hospital façade were caused by debris projected by the initial blast.[87]
On January 31, 2023, Human Rights Watch released a report calling for Ukraine to “investigate its military’s apparent use of thousands of rocket-fired antipersonnel landmines in and around the eastern city of Izium” during the occupation of the town by Russian forces.[88] Some of the reported incidents concern the Izium Central City Hospital, which had reportedly become a military base for Russian forces while also continuing to function as a health care facility.[89] Indeed, the hospital remained (and continues to be) operational even as it came under attack; however, it can only work at 10 percent of its capacity due to the extensive damage it suffered.[90] At the time of the Ukrainian Healthcare Center’s (UHC) visit to the hospital site in November 2022, the non-acute services and trauma department had been relocated to the first floor of the hospital. However, the intensive care unit and operating block could not be similarly relocated. Both remain out of commission due to the extent of the building’s destruction and the loss of medical equipment.
Case Study #2
Makariv Multiprofile Intensive Care Hospital, Makariv Primary Care Clinic, Adonis Medical Center (Kyivska oblast)
Makariv is a town located 30 kilometers west of Kyiv, with a population of almost 15,000.[91] The location of the town is strategic: it sits in proximity to a significant junction on the E40 highway, which connects Kyiv with the western part of Ukraine, making it a crucial gateway for Russian forces to surround and seize the capital. On February 28, 2022, Russian troops advanced on Makariv from the north, armed with tanks and armored personnel carriers,[92] with the aim of cutting off the E40 highway. Members of Ukraine’s Territorial Defense Forces (UTDF) managed to repel the offensive. However, the town remained under shelling, resulting in severe damage to civilian infrastructure[93] and the death of many civilians.[94] While the town was never occupied, Russian troops held the northeastern outskirts until April 1, 2022. It continues to be a contested frontline vulnerable to Russian aerial attack.
The Multiprofile Intensive Care Hospital and the Primary Care Clinic are located on the same campus in the northwestern part of Makariv. The Multiprofile Intensive Care Hospital consists of several buildings, including the main hospital building, the administrative building, the emergency care station, and several minor buildings and provides inpatient care in six departments (surgical, internal medicine, neurology, infectious diseases, pediatrics, and anesthesiology) with intensive care beds. Before the full-scale invasion, the hospital had more than 400 employees, including 78 doctors, and 170 available beds.[95] The Primary Care Clinic was a brand-new, well-equipped facility which began operating in December 2020 as the first clinic dedicated to primary care in Makariv.[96] The clinic offered primary care services for around 16,000 people, including 4,000 children, as well as COVID-19 vaccination.[97]
Dr. Serhiy Solomenko was the director of the Primary Care Clinic and worked as an anesthesiologist at the Multiprofile Intensive Care Hospital until March 7, 2022, when the UTDF evacuated all remaining patients and doctors from the facility.[98] With the advance of Russian forces, the evacuation of the clinic had gradually begun on February 25 with the UTDF’s help through corridors established by the Kyivska Oblast Military Administration.[99]
According to Dr. Solomenko, “Before the evacuation, everything was done to the maximum so that our Territorial Defense and the Armed Forces of Ukraine were not on the hospital’s territory, in order not to give the aggressor a reason to shell.”[100] After the March 7 evacuation, however, Ukraine’s armed forces reportedly established a base at the hospital,[101] where there was a large basement, a generator, and a nearby water tower.[102] Dr. Solomenko added that they [the UTDF and Armed Forces of Ukraine] would hide in the hospital rather than the clinic, as they knew the clinic was not safe: “it was made of wood … there was no basement.”[103]
Between February 26 and his evacuation on March 7, Dr. Solomenko witnessed several attacks that damaged both the hospital and the clinic. At the time, he reported that Russian forces had placed their vehicles and other equipment “at a distance of 100-300 meters from the hospital territory … they fired from tanks, grads, mortars.”[104] He recalled:
“The first shelling was on February 26, when a machine gun was fired at the [Multiprofile Intensive Care] hospital. Then, there was a mine explosion which shattered almost 50 windows of the hospital.… The [Primary Care] clinic was damaged by bullets when the fighting was going on, and for example, when there was active mortar shelling on the territory of the [Intensive Care] hospital, the clinic’s facade and roof were damaged.… The town’s water tower was also damaged.[105]”
During a site visit in May 2022, UHC detected “four funnels from mortar strikes near the [Primary Care Clinic] located along one line at a distance of approximately 10 [meters] from one another” and two other holes in the rubble of the facility, suggesting that “the mortar fire was corrected stepwise until the target was finally hit.”[106] They also analyzed the traces of explosion left on the ground to determine the direction from which the mortar had been fired.[107] Their findings as to the probable firing location coincide with statements made by Makariv residents as to the position of Russian forces at the time.[108]


Following the March 7, 2022 evacuation, more attacks ensued. On March 22, 2022, all of the Multiprofile Intensive Care Hospital’s ambulances were destroyed in reported shelling.[109] On March 28, according to a member of the UTDF who spoke with Dr. Solomenko, the hospital was shelled again and a projectile flew from a multiple launch rocket system, causing the Primary Care Clinic to catch fire.[110] The entire facility, equipment, vaccines, and documents burned down;[111] they no longer exist.[112] Despite the absence of clear imagery of munitions fragments, a weapons analyst assessed that the type and extent of the destruction suffered by the clinic are consistent with that of a BM-21 Grad MLRS.[113]


The Multiprofile Intensive Care Hospital partly reopened on April 5, 2022, providing care to around 200 patients daily while the reconstruction work is ongoing. In May 2022, a fundraising campaign was announced to restore the facility.[114] In July 2022, a mobile hospital was opened in the hospital’s territory.[115] By September 2022, most of the windows that had been broken were replaced, and the roof and facade were repaired.[116] As of January 2023, the hospital operates at 50 percent of its prewar capacity, with only 50 beds available for inpatient treatment.[117]
The Adonis Medical Center was located near the Makariv town center, surrounded by residential buildings, shops, and the city council building. The area was strategically important due to its proximity to the bridge over the Zdvyzh River, crucial to control access for refugees, reinforcements, and supplies, as well as to prevent Russian forces’ advancement from the north. Opened in January 2019, the Adonis Medical Center was a multidisciplinary private hospital providing a wide range of services, including pediatrics, surgery, neurology, physiotherapy, dental care, and orthodontics.[118] The hospital halted its functions on February 25, 2022 as a result of the Russian invasion.
While the exact date of the attack on the Adonis Center is unknown, CNN published an article on March 12, 2022 reporting a series of “apparent Russian airstrikes” that devastated several buildings in the area.[119] Based on its geolocation and verification of the authenticity of photos posted on social media, CNN concluded that many of the buildings, including the Adonis Medical Center, “sustained damage on their northern facades, evidence that points to military strikes that hit them being Russian.”[120] The facility was entirely destroyed and all its equipment was lost. There is no information as to whether or when it will be restored.

Disruptions to Community Health Care
The scale of damage to the health care system in the Makariv municipality – with three health facilities and 30 pharmacies damaged or destroyed to different extents[121] – has led to severe disruption of health services and infrastructure in the area, further limiting the right to adequate health care. The town also suffered repeated disruptions to the supply of electricity, water, and gas; access to the Internet and mobile communications were also precarious.
Case Study #3
Chernihiv Regional Children’s Hospital (Chernihivska oblast)
Chernihiv, a city of 280,000 inhabitants in the north of Ukraine, is historically known as a fortress city. In February 2022, it literally became one as it was set upon and encircled by Russian forces. As Russia’s offensive moved southward towards Kyiv, its armed forces initially attempted to enter Chernihiv on February 24 but were forced to retreat after facing fierce battles at the outskirts of the city.[122] Failing to take the city itself, Russian forces began subjecting it to continuous fire, terrorizing its population[123] and destroying civilian infrastructure. By the middle of March, Chernihiv had “been under effective blockade for more than two weeks, with most buildings left without electricity, heat, or water.… All the while, the Russian military pummeled Chernihiv with bombing raids and missile fire, turning a locked-in city into an urban death trap.”[124] In February and March 2022, numerous health care facilities were hit during attacks on the city and its surrounding areas,[125] including hospitals in the city center and two primary health care facilities in the nearby village of Kyinka.[126]
The Regional Children’s Hospital, located in the city center of Chernihiv and surrounded by residential buildings, provided care to children from both the city and the broader oblast of Chernihivska. Approximately 700 medical personnel worked there prior to the February 2022 Russian invasion, with the capacity to treat nearly 500 children at any given time.[127] The hospital offered a wide range of pediatric services, including intensive care for newborns and premature babies, infectious diseases, neonatal pathology, and surgery. It also exclusively provided around-the-clock comprehensive inpatient and consultative care for children with disabilities with the most complex pathologies, all of which require intensive therapy.[128]
Following the 2022 invasion, the hospital started treating both adults and children.[129] It also became a de facto shelter for many civilians who sought safety from explosions in their neighborhoods.[130] The Chernihiv Regional Tuberculosis Clinic was also transferred there because the hospital had an infectious disease ward.[131]
Over the course of Chernihiv’s encirclement, there was a steep increase in patients brought to the Regional Children’s Hospital for care; the largest influx took place on March 3. That day, heavy unguided aerial bombs with explosive warheads – likely FAB-250 or FAB-500 bombs dropped from a Su-34 or a Su-35 Russian fighter aircraft[132] – destroyed apartment buildings on Chornovola and Bohuna streets, inflicted heavy damage on the Regional Cardiac Center, and blew out the frames of the Regional Children’s Hospital located nearby.[133] Following the influx of patients, personnel of the Regional Children Hospital were forced to use medical triage: There were “37 injured adults [rushed to the hospital] within an hour.… There was medical sorting: the 200s [military term for the deceased] there, the children here, those who could be saved were saved.”[134] Among the injured brought immediately after the March 3 strike were children with fragments and metal shards in their faces.[135] One boy and an adult died at the hospital that day.[136]

After the March 3, 2022 strike, Dr. Mykola Liutkevych, the head of the Regional Children’s Hospital trauma department, who was on duty at the time, and his colleagues created a group in a messenger app to engage and organize doctors at the Regional Children’s Hospital.[137] When Dr. Liutkevych received a phone call about a boy with multiple fractures who was undergoing surgery in another hospital across town, he knew he had to go, even under shelling. But with no normal heating or electricity, the boy’s injuries were too severe. He died two days later.[138]
Two weeks later, attacks damaged two hospitals in Chernihiv.[139] On March 16 or March 17, 2022, City Hospital #2, located in a medical complex in the northeastern part of Chernihiv, was struck.[140] In the morning of March 17, civilian areas in the city center of Chernihiv, where the Regional Children’s Hospital and City Hospital #1 are located, were shelled.[141]
The Regional Children’s Hospital suffered significant damage: 238 windows from the first to the fifth floors, doors, and the roof were damaged,[142] while the hospital’s oxygen station posed a high risk of explosion.[143] The attack also killed at least 14 people and injured at least 26 others.[144] Wounded civilians were brought to the hospital from the surrounding area: at least three heavily injured children were admitted immediately after the shelling; shrapnel was removed from several patients’ bodies, including children.[145]

According to Dr. Liutkevych, the attack came without a prior air raid alarm.[146] In an interview with UHC, he also stated that the hospital’s management ensured that military vehicles were not parked in the surrounding area at any time; they knew they could be attacked if there were weapons around.[147] At some point, the hospital was guarded “because we were scared that Russian sabotage and reconnaissance groups might come in at night as patients, say they’re sick, take hostages and attack from within.”[148] An investigation conducted by Human Rights Watch (HRW) also found “no indications that Ukrainian forces were in the vicinity at the time” and “no obituaries … of Ukrainian armed force members who died there that day.”[149]

The attack that damaged the Regional Children’s Hospital was likely launched from a BM-27 Uragan multiple launch rocket system (MLRS) – a system whose accuracy is significantly limited compared to modern guided systems – with warheads carrying cluster munitions.[150] A HRW on-site investigation into the attack revealed at least five splatter patterns consistent with the detonation of cluster munition shelling near the hospital.[151] Munition fragments and debris of cluster munition rockets were found along both sides of the hospital, on its premises, and in its rooms, as well as in the surrounding area.[152] During a site visit in July 2022, UHC captured photographs of the hospital’s façade, revealing traces of cluster munition shelling. An emergency responder also confirmed that his team found four unexploded 9N210 submunitions from a BM-27 Uragan, including one in the grounds of the hospital, as well as the empty cargo section of the MLRS only 20 meters away from the hospital’s main building.[153]
According to Andriy Prosnyak, chief investigator of the Security Service of Ukraine, “by the direction of the shelling, it is theoretically possible to determine where it came from.”[154] This, in turn, could help identify those responsible for launching the attack. During a site visit in July 2022, UHC calculated, based on the traces of explosion on the ground, that the attack that damaged the Regional Children Hospital had been launched from the south, directed approximately 45-49 degrees northeast, along the line between Shevchenka and Novoselivka and in the direction of Terekhivka.[155] The range of the BM-27 Uragan from which the attack was likely launched – up to 34 kilometers[156] – along with Russian forces’ close to full encirclement of Chernihiv at the time, including from the south,[157] suggest that the launch took place from areas they controlled.
March 2022: Ukraine’s Hospitals in the Dark
At the Regional Children’s Hospital, there was not enough food, medicine, and water, and there was only one power generator. Doctors had to manually resuscitate six premature babies who would usually require special life support equipment. At times, there were only two surgeons performing surgeries, and surgical supplies were particularly scarce after the bridge to Chernihiv was blown up at the end March.[158]
Case Study #4
Bashtanka Multiprofile Hospital (Mykolaivska oblast)
In late February 2022, Russian armed forces advanced into the Mykolaivska oblast, occupying towns and cities. By mid-March, the frontlines reached the city of Bashtanka, located roughly 30 kilometers from the Bashtanka Multiprofile Hospital, with Russian forces occupying several towns in the city’s vicinity. Ukrainian forces defended the city, with reports of a Russian convoy being ambushed and destroyed on or around March 1, 2022.[159] Throughout March and April, 2022, Russian forces repeatedly bombed the city with Grad rocket launchers, warplanes, and Tochka-U missiles.[160]
The Bashtanka Multiprofile Hospital is a public nonprofit hospital, renovated in 2004 to expand its overall capacity and improve services,[161] that, before the full-scale Russian invasion, provided care to more than 144,000 patients.[162] The hospital offered a wide range of services, including a childbirth department, ambulatory outpatient polyclinic, inpatient care, same-day surgery, and an infectious disease department.[163] Alongside two other hospital campuses owned by the two other major hospitals in the city, the Bashtanka Multiprofile Hospital is located on the northwestern edge of the city, in a remote area just off the H11 main road that connects the cities of Kryvyi Rih and Mykolaiv, the oblast’s administrative center. The hospital’s buildings are the highest in the area; as such, they could provide a vantage point to overlook Russian forces’ advance from the south.[164]
According to local officials, there was no military presence “anywhere near the hospital”[165] except for the treatment of wounded members of the armed forces.[166]
On April 19, around 5:20 p.m., the Bashtanka Multiprofile Hospital was struck by a missile.[167] A weapons analyst’s review of a video released by Sky News showing the missile remains at the hospital reveals what appears to be a Russian cruise missile, likely a 3M-54 Kalibr.[168] The missile was possibly launched from the Black Sea, which would likely make it an anti-ship Kalibr missile used against a land target.[169] When used against land targets, sea-launched precision-guided missiles may struggle to reach the intended target and, instead, strike the highest buildings in the area.[170] However, these types of precision-guided weapons are very expensive, fairly scarce, and require a high level of clearance.[171] According to a weapons analyst, they are commonly used to strike previously identified, high-priority targets.[172] Based on its relatively isolated but strategic location, due both to its proximity to the H11 road and the vantage point provided by its tall buildings, it is possible that the Bashtanka Multiprofile Hospital was the intended target of the attack.
Although the staff received no warning of the impending attack, there were fortunately no casualties among the patients and medical personnel because the missile hit the hospital’s outpatient polyclinic[173] and primary care center after reception hours.[174] Still, at the time of the strike, doctors were in the midst of performing surgery in another department and three women were in labor in the maternity ward.[175] Moreover, as a result of the missile attack, the institution’s security personnel were injured.[176]
The facility, like other hospitals in the region, had been marked with a Red Cross painted on a white canvas placed on the roof.[177] According to Dr. Alla Barsehian, the hospital director, drones flew over the facility, “They saw very well, they knew that this was a medical institution.”[178] In her words, “We hoped this would somehow save us. But it turns out there is nothing sacred in this war.”[179] In an interview with UHC, Dr. Barsehian clarified that she was not at the hospital when the missile struck, but returned immediately when she heard the explosion. Her colleagues who were at the hospital told her that:
“It was the sound of a whistle and an explosion. […] It was the sound of broken glass, dust rising. But it was for a few seconds. Everything fell and everyone began to realize what had happened. Literally seconds.”[180]


Following the strike, the hospital’s evacuation team, which also included three military doctors who lived in the premises, immediately moved 60 staff and 90 patients, including children, to the attached bomb shelter in preparation for a second potential attack.[181] The evacuation team contacted a nearby medical facility and transported patients there within an hour.[182] Hospital guards conducted patrols of the property together with a unit of the Ukrainian Territorial Defense and moved all remaining medical materials from the hospital warehouses to safer locations.[183]

The missile attack reportedly destroyed around 30-40 percent of the hospital’s premises,[184] completely decimating the outpatient polyclinic and adjacent infectious disease department, as well as the dialysis department, two gas boilers, and a range of medical equipment.[185] Shelling also destroyed two on-site drug depots, rendering the facility without medicine until materials could be supplied from another location.[186] Hospital staff counted at least 330 shattered windows, while several doors were blown off their hinges.[187] The overall damage caused by the strike is estimated at more than one million euros.[188] The hospital’s main building retained its structural integrity, however, despite heavy damage. [189]
Efforts were also made to quickly restore operations, with repairs starting on April 20, 2022 and the hospital opening to the public on the following day.[190] In the words of the hospital director, “We understood that it is necessary to restore the work of the facility as soon as possible. Therefore, a decision was made: we moved medical inpatients, quickly restored the polyclinic department.”[191]
After a gradual reconstruction process, the hospital is once again fully operational, with some remaining disruptions, particularly for the childbirth services.[192] Staff noted that the demand for services in the neurology, infectious disease, and ambulatory departments have greatly increased in order to treat the wounded and accommodate the influx of patients from newly liberated areas.[193]
Case Study #5
Trostianets City Hospital (Sumska oblast)
Trostianets, a town of nearly 20,000 inhabitants close to the Russian border, was occupied by Russian forces from February 24 to March 26, 2022.[194] After the first few days of the occupation, Russian forces cut the cellular network and electricity, isolating residents from the outside world.[195] During the occupation, residents alleged brutal, inhumane treatment by Russian forces, low food supplies, and limited access to heat.[196] Fighting in Trostianets was heavy, with city Mayor Yuriy Bova stating that “traces of bullets and shrapnel remained on almost every building.”[197]
The Trostianets City Hospital is located in a forested area in the city’s outskirts; it is a “standalone complex of buildings accompanied by several residential houses.”[198] The hospital was marked with a large hospital sign and a white flag bearing a red cross.[199]
Prior to being attacked, the hospital had been operational throughout the occupation, providing care to everyone, including Russian soldiers.[200] Speaking to UHC in August 2022 on the condition of anonymity, a doctor who worked at the Trostianets City Hospital stated that the polyclinic closed on February 25, 2022, but that the hospital continued to accept patients in the emergency and surgical departments, with general practitioners, surgeons, gynecologists, anesthesiologists, and pediatricians providing care.[201]
The doctor reported that, until March 18, there were no military forces or equipment nearby. On March 18, however, several Ukrainian soldiers were spotted near the hospital: according to the doctor, a witness stated that they were in the forested area close to the hospital, while another stated that they were providing humanitarian aid at the hospital.[202] On the same day, a Russian officer visited the doctor at his house, possibly looking for Ukrainian partisans.[203] Later that day, around 5:00 pm, a tank drove down the street and shot two blank projectiles at the hospital’s building.[204]
A day later, a Russian officer[205] came armed to the hospital, searched it, and after first talking to the staff, shot randomly on the first floor.[206] The officer said he had mined the territory of the hospital and warned the doctor not to walk there.[207] Russian soldiers then set up two roadblocks, behind and in front of the hospital.[208]

In the following days, the doctor witnessed what he called “mutual altercations” between Russian forces and Ukrainian partisans across the street from the hospital.[209] Dr. Tetiana Sydorenko, the head of the hospital’s maternity ward, also reported incessant attacks on the facility: “It’s hard to explain, the explosions. It was in your head. It was above your head. It was exploding inside of you. It was hell.”[210] According to Dr. Anna Shevtsova, the hospital’s medical director, the hospital then came under persistent, repeated assault, with attacks also reported on March 20, 23, 24, and 25.[211]
The worst strike reportedly occurred on March 23, when at least one Russian tank[212] fired directly at the hospital[213] and hit the second and fifth floors of the inpatient building.[214] The infectious diseases department, located in a separate building, was also apparently hit in the attack by an object described by the doctor who spoke to UHC as a “mine.”[215] A tank was reportedly “blown up as it bombarded [the] hospital” and was left behind at the site of the attack, with “its gun still pointing directly at the hospital.”[216] Ukrainian investigators later identified the commander alleged to have given the order to fire at the hospital, reportedly with a T-80 tank.[217] They also identified two other Russian servicemen – a T-72 tank commander and his assistant – alleged to have encircled the hospital and fired a 125-mm high-explosive fragmentation shell with a tank on an unspecified date in March.[218]


The doctor who spoke to UHC described the difficult conditions he and his team had to work under: there was no power for more than a week, no heating, and almost no water.[219] Under shelling, the medical personnel was forced to get a generator at a gas station.[220] The doctor managed to escape from Trostianets with his family on March 24, just two days before the town was liberated.[221]
As a result of the repeated attacks, the hospital’s operating room was burned, the gynecology, maternity, and surgical wards were damaged, the roof of the infectious disease department was fully destroyed, and exterior walls of the hospital were marred by shelling impact.[222] Evidence gathered by UHC after the shelling also shows a destroyed ambulance, damage caused by multiple shells, and destroyed oxygen tanks.[223] A video of the aftermath of the shelling posted by the Head of the Sumska Oblast Military Administration additionally depicts what appears to be a severely damaged pharmacy.[224]
The severity of the damage sustained by Trostianets City Hospital means that it was no longer functional in the aftermath of the occupation, with patients in need of medical care being treated at facilities located 45-50 kilometers away.[225] Yuri Bova, the mayor of Trostianets, stated:
“We used to have almost 400 staffers there before the war, but only 20 people are left. We can’t actually provide care with that small a staff, so doctors from other cities have to travel to help us, which firstly isn’t safe enough and secondly doesn’t solve the need for daily service. We believe our staff will feel safe enough to return once we have repaired the windows, restored heating, and provided treatment for the most urgent cases.”[226]
The cost of rebuilding the facility is estimated at approximately 116 million Ukrainian hryvnias (nearly US$4 million).[227] Nevertheless, while the hospital is still in need of repair, patient care has resumed.[228] International aid has helped to set up a field hospital where surgeries can resume, and donated medical equipment, medicines, and five ambulances to replace those that were destroyed.[229] A temporary “mobile hospital” serves the local community until Trostianets City Hospital is fully repaired, a project that will take years.[230]
2. Attacks on Ambulances
Ambulances have a critical role to play in armed conflict by evacuating the wounded, providing life-sustaining treatment, and transporting patients to seek necessary medical care. These vehicles are protected under international humanitarian law: the Geneva Conventions explicitly provide that “[c]onvoys of vehicles or hospital trains on land or specially provided vessels on sea, conveying wounded and sick civilians, the infirm and maternity cases, shall be respected and protected in the same manner as … hospitals”[231] and Additional Protocol I provides that “[m]edical vehicles shall be respected and protected in the same way as mobile medical units.”[232]
Alongside attacks on hospitals, attacks on ambulances have become another distinctive feature of the war in Ukraine. Since February 2022, documented attacks on ambulances have ranged upwards of 66. Some of the attacks happened at the premises of hospitals, while others occurred as ambulances were on call. Illustrative, non-exhaustive examples of attacks include:
- February 26, Khersonska oblast: On a highway in the Khersonska oblast, Russian forces reportedly shot at an ambulance carrying a wounded Ukrainian soldier from Tyahynka of Beryslav district to a hospital in Kherson, killing the driver and the patient and injuring a paramedic.[233] The ambulance caught fire.[234]
- February 27, Poltavaska oblast: Ihor Lidovy, the head of the Serhiivska community, reported that an ambulance was shot by a “sabotage and reconnaissance group of the enemy” while responding to an emergency call between the city of Hadiach and the village of Serhiivska.[235] At that time, in the north, near the city of Hadiach, Russian forces were advancing on the oblast.[236] The ambulance was riddled with 17 bullet holes and both the driver and a nurse were wounded.[237]
- March 4, Sumska oblast: Russian forces reportedly shot at an ambulance with small arms on the Sumy-Kyiv highway.[238] There were no casualties,[239] but Dmytro Zhyvytskyi, head of the Sumy Regional State Administration, reported that “shelling of civilian vehicles and civilians in the region continues.”[240]
- March 12, Sumska oblast: Yuriy Bova, the mayor of Trostianets, reported that Russians soldiers destroyed the Trostianets emergency ambulance station, stole three ambulances, and seized emergency medical supplies as people were leaving the city through the designated “green corridor” (a ceasefire on specific routes to evacuate civilians).[241] A week before, Russian forces had reportedly captured the city’s ambulance station, threatening to shoot medics attempting to leave the premises except for pediatric emergencies.[242]
- December 13, Kharkivska Oblast: The Office of the Prosecutor General of Ukraine reported that, around 4:30 a.m., the Russian military launched a S-300 type of missile on Kupiansk.[243] The blast wave broke the glass of an ambulance en route to Kupiansk and a paramedic was injured.[244]

There are other examples of incidents that resulted in the damage or destruction of ambulances, for which the alleged perpetrators were not named:
- March 12, Kharkivska oblast: The Kharkiv Center for Emergency Medical Aid and Disaster Medicine reported that their ambulance brigade came under fire after responding to a call in one of the Kharkiv neighborhoods.[245] The vehicle was hit by debris and the paramedic was wounded.[246]
- On or after March 23, Chernihivska oblast: In an interview with UHC, Dr. Mykola Liutkevych, the head of the Regional Children’s Hospital trauma department in Chernihiv, reported that after the siege of the city began and the main bridge was destroyed,[247] an ambulance was shelled, apparently with mortars, as it attempted to cross the river via a pedestrian bridge to retrieve a power generator.[248]
- October 3, Kharkivska oblast: An ambulance was blown up by a mine on its way to Balakliia.[249] A paramedic was injured, the driver died at the scene, and the ambulance burned down.[250]
Similarly, all of the Trostianets City Hospital’s ambulances sustained severe damage as a result of shelling in March 2022. A doctor who worked there and spoke to UHC on the condition of anonymity said that their ambulance was destroyed by a mine.[251] A sanitary medical aid car stored near the hospital was also shelled towards the end of the occupation.[252] The only remaining ambulance was taken by Russian forces, leaving medical personnel unable to provide care outside of the hospital.[253] As a result, pregnant women had to be transported to the hospital in wheelchairs with flags marked with crosses because there were no ambulances left.[254]
Case Study #6
Ambulance Attack in Lyman (Donetska oblast)
Situated in Donetska oblast, near the Russian border, Lyman is an important town on the frontline of the war. Between the start of the hostilities in the region in 2014 and the full-scale Russian invasion of Ukraine in 2022, Lyman’s ambulance station was largely unaffected.[255] In February 2022, however, almost all doctors fled Lyman for safer territory. Only four doctors and medical personnel remained.
On April 18, 2022, Serhii Haidai, the head of the Luhanska Oblast Military-Civilian Administration, reported that the Russian military had entered the city of Kreminna (Luhanska oblast) and that the Ukrainian army had left.[256] On the same day, around 12:00 p.m., an ambulance operator called the Lyman station and reported a call from an injured man close to the village of Torske (Donetska oblast) on the highway connecting the village to Kreminna.[257] The man was reportedly injured when his car was “shelled from large-caliber machine guns mounted on the turrets of tanks, as well as from assault rifles” as he and his family rushed to escape the Russian forces advance into Kreminna; his wife, mother-in-law, and dog all died in the attack.[258] According to an investigation conducted by the Media Initiative for Human Rights (MIHR), the man’s car was almost certainly fired at by Russian forces.[259]
A paramedic and a doctor, along with the ambulance’s driver, went to the man’s aid. The paramedic on duty at the time spoke with MIHR on the condition of anonymity:
“We passed through four [Ukrainian] checkpoints, they let us through, said it was safe, said ‘Please, go ahead.’ When we had passed all the checkpoints, about two kilometers, according to the driver, from the last checkpoint near the village of Torske, we came under fire.”[260]
The paramedic recalled:
“At first, I didn’t understand what was happening, it felt like stones were being thrown on metal, that was the sound. When the car caught fire, we realized that we were being fired at, we stopped. We fell into a ditch. When everything was calm, the shooting stopped, we took the things that could be carried on our shoulders and carefully walked in the opposite direction. Making a call was very scary because we didn’t know what they could do to us.”[261]
According to the paramedic, the target of the shots was the ambulance. “When we were going in the direction of Kreminna, they were shooting from the right side. You could tell by the holes, because the car was shot from the right side, and the bullets remained on the left side of the [ambulance]. That is, the left side was not shot, there were no holes.”[262] The MIHR investigation makes no conclusion about the perpetrator of the attack on the ambulance. However, on the morning of April 18, 2022, a witness who fled from Kreminna to Torske through a road passing by Dibrova saw the bodies of Ukrainian soldiers and a convoy of vehicles with Russian flags, which began to shoot at his car.[263]
When the shooting stopped, the ambulance team fled in the direction of Torske on foot. The paramedic and the driver were picked up by Ukrainian soldiers in a car and taken from the village of Torske to the village of Zarichne and back to the Lyman ambulance station.[264] In Zarichne, they had to wait in the basement of the school because of the shelling of the villages of Torske and Zarichne. In the paramedic’s words, “The stress level was 100 percent.… I did not believe that I would return alive from the shelling.… Even now, I feel anxious.”[265]
As the ambulance team fled towards Torske, they lost sight of the doctor. He “had heart problems … the doctor must have stopped to rest and that’s how we lost him,” the paramedic said.[266] A Ukrainian soldier went back to get the doctor, but the paramedic does not know what happened to either of them.[267] A video was later released on a pro-separatist Telegram channel in which the doctor explained that he ended up in the occupied territories following the ambulance team’s escape from the scene of the attack.[268]
Following the attack, the paramedic and another colleague continued to work at the Lyman ambulance station on an outpatient basis; they no longer left for calls.[269] On April 23, 2022, the station stopped functioning entirely because the other colleague no longer came, and the paramedic could not work alone every day.[270] On April 30, 2022, the paramedic left Lyman and went to live in Odesa for a month, before moving to Cherkasy to work as a nurse until November 2022. Since then, the paramedic has returned to work at a different ambulance station in the Donetska oblast, ready to go on calls again if it is safe to do so.[271]
3. Theft and Destruction of Medical Equipment
Russian forces have also reportedly engaged in the theft and destruction of vital Ukranian medical equipment. Medical equipment and supplies are protected under international humanitarian law.[272]
Most verified cases of looting have been uncovered in recently liberated Ukrainian territories. In late October 2022, Ukraine’s President Volodymyr Zelensky stated that “Russian forces in the occupied Ukrainian region of Kherson are engaged in mass theft of medical equipment and ambulances in a bid to make the area uninhabitable.”[273] The scale of these acts began to come into focus when the right bank of the Kherson region was liberated on November 11, 2022.
Instances of medical equipment theft reported in open sources include:
- The hospital director of the Adonis Medical Center in Bucha (Kyivska oblast) reported that, in March 2022, medical equipment was stolen; some of it was taken along with the electrical sockets.[274]
- Russian forces reportedly took valuable medical equipment away, including computers, patient monitors, a mobile X-ray machine, a generator, equipment from the intensive care unit, and almost 100 oxygen concentrators used to treat COVID-19 patients, as well as blankets and pillows from the Izium Central City Hospital.[275]
- On April 29, 2022, the Mariupol City Council reported that around 60 ventilators had been stolen from city hospitals and transported to Russia.[276]
- On May 1, 2022, Ukraine’s military intelligence service reported that all equipment provided under programs from international donors and the Ukrainian government since 2014 had been taken away from the infectious diseases department of the Starobilsk Multiprofile Hospital (Luhanska oblast).[277]
- In mid-May 2022, Serhiy Haidai, head of the Luhanska Oblast Military Administration, reported that Russian forces had begun dismantling medical equipment from a hospital in Kreminna (Luhanska oblast) and transporting it to occupied Luhansk or Russia.[278]
Multiple cases of looting of medical equipment, medicines, furniture, and cars and of damaging facility premises were also reported by the hospital personnel of the Kyiv Regional Mental Health Center in Vorzel (Kyivska oblast).[279]
Case Study #7
Balakliia Clinical Multiprofile Intensive Care Hospital (Kharkivska oblast)
Balakliia is a town of 27,000 located in the east of Ukraine. It was occupied by Russian forces in early March 2022[280] and remained under occupation until September 8, 2022.[281] The Balakliia Clinical Multiprofile Intensive Care Hospital was not occupied until early April 2022. Located in an isolated forest area on the outskirts of the town, the hospital was initially situated beyond the control of Russian military checkpoints.
The Balakliia Clinical Multiprofile Intensive Care Hospital is a public non-profit hospital that served more than 80,000 residents of the Balakliia and neighboring districts.[282] The facility was equipped with modern, high-tech equipment[283] and provided inpatient care in infectious, therapeutic, neurology, maternity, and pediatric departments with more than 350 inpatient beds.[284] Around 14,000 patients were treated annually in inpatient departments.[285]
Until early April 2022, the hospital was fully operational, despite the occupation of the nearby town by Russian forces; it provided care to patients and sheltered civilians from nearby areas.[286] On April 2, 2022, the hospital was hit, reportedly by a tank.[287] According to Dr. Maryna Rudenko, the hospital’s director, “all the windowpanes were immediately smashed, there were shards in all the offices” and one patient was injured by shards.[288]
Dr. Rudenko lived inside the facility until she evacuated on April 4, 2022. In an interview with UHC, she recounted the events that unfolded between the day it was hit and April 4, 2022, when Russian forces reportedly seized the hospital:
“On April 2, they set up a tank somewhere behind the forest and shot the hospital, just like that, from the tank – six shells – five of them hit our buildings. .… They interrupted our heat supply and water system, and we realized on the 3rd of April that the hospital could not work here. On [that day], we discharged as many patients as possible and everyone else who was [sheltering] in the basement.
“The FSB [Russia’s Federal Security Services] came to us on April 3 in the evening. They gathered all the medical staff … and said, ‘Don’t even think about going anywhere, you have to live here, you have to work here. We need to establish communication with the local population, so we will not let the doctors leave the city. You will not leave here. You were shelled by Ukraine, don’t even doubt it.’

“The Russians came on the night between the 3rd and the 4th of April with assault rifles. They threatened us, shot in the air and all over the building in the darkness.… They hit our acute care department chief on the head with a rifle butt .… They [ordered] our male doctors to lay on the floor faces down and started to shoot at the floor.… The bullets rebounded and could hit anyone.… Then, they let us out and left. But they had put the ultimatum: until morning, none of us could stay here [in the hospital].”[289]
On April 4, 2022, Dr. Rudenko evacuated the hospital, only to return five months later after the liberation of Balakliia by Ukrainian forces. Much like reports of widespread looting in other hospitals that were allegedly occupied by Russian forces in the Kharkivska oblast,[290] the “occupiers completely plundered” the Balakliia Clinical Multiprofile Intensive Care Hospital, and “what they could not steal was broken and mutilated.”[291] In an interview with UHC, Dr. Rudenko described:
“Almost everything was stolen. They took away everything that could be taken away. They couldn’t move the CT scanner, so they looted the electronics from it. .… We had two surgical stands.… We hid them in the basement, but they found them and stole them. All the tools were stolen. The diagnostic department: there is nothing at all, everything was stolen; they lived there. That is, all ultrasound machines, cardiographs, encephalographs; nothing. They took it out.… We also had a generator for 100 kilowatts: disappeared. Out of 15 [ambulance] cars, 14 disappeared with them. Telephones, 37 washing machines, microwave ovens…”[292]
Dr. Rudenko also told UHC that hospital property, such as beds, was found across the town or in nearby villages, while other property, not belonging to the hospital, was found on the premises.[293]



Upon her return, Dr. Rudenko also found evidence that Russian forces had established their base in the hospital and left hastily, leaving behind cans of food, scores of ammunition in the basement, and grenades attached to stretchers.[294] The hospital was more damaged than when she evacuated in April 2022, with the children’s department blown out, the roof seriously damaged, and the ceiling of the second floor collapsed. “It could have happened during the liberation, or maybe at another time,” she says.[295]
During a site visit in November 2022, UHC found broken walls, windows, and traces of fire in the conjunction corridor connecting the two hospital buildings.
Even as the town was liberated, the hospital could not reopen immediately, as sappers worked to demine the facility.[296] Due to the extensive damage suffered and the looting of equipment, the hospital referred patients to its polyclinic department located in the city center.[297] On January 3, 2023, the hospital finally reopened.[298]
4. Attacks on Health Care Workers
Health systems depend on their health work force. Violence against health personnel reduces the number of health workers and affects the quality of care that surviving doctors and nurses are able to provide. Death and injuries of colleagues not only reduce the workforce but add strain on those who stay. Witnessing the violent death of a colleague also frequently traumatizes health care staff, making it harder for them to care for others.
As in many conflicts, health care workers in Ukraine are on the front lines, providing lifesaving care to civilian communities, while facing attacks themselves. The narratives of three doctors below highlight the harrowing situation many Ukrainian health care professionals faced while also striving to provide care in the face of unsanitary, inhumane conditions.
Case Study #8
Providing Health Care under Occupation: Kherson Regional Clinical Hospital (Khersonska oblast)
The occupation of Khersonska oblast began on February 24, 2022[299] and extended into the health care system that summer. On the condition of anonymity, a doctor at Kherson Regional Clinical Hospital,[300] located in one of the residential areas of the city of Kherson, spoke to MIHR researchers on several occasions.[301] The doctor provided the following testimony about what he personally witnessed and what medical colleagues communicated to him after he escaped Kherson on July 7, 2022. The doctor had been one of the last specialists in his field who remained in the city, until he fled disguised as a student. His testimonies have been translated, edited, and condensed for clarity.
At the beginning of the spring of 2022, the occupation authorities banned the import of medicines into Kherson; this spurred an “underground” trade in medicines throughout the city. From the start of the occupation, Russian “entrepreneurs” appropriated Ukrainian pharmacies and started selling Russian medicines. They were of much lower quality than Ukrainian and European ones.
Until the beginning of the summer, Russians were present in hospitals [of the Khersonska oblast], but they did not try to influence the work of the hospital. As long as there was a Ukrainian cellphone connection on the territory of the city, doctors could write electronic prescriptions for patients in the oblast. Despite the shelling, volunteers delivered medical supplies to the sick. However, every month it became more and more difficult to work.
In the summer of 2022, hospital management was summoned to talks with the occupation administration. Ukrainian doctors were offered to cooperate with the administration at special meetings held in the occupied Department of Health Protection of the Kherson State Regional Government.[302] I was forced to attend these meetings twice.
At the first meeting in June 2022, the new occupation authorities demanded access to the electronic database of patients, “e-Health,” from Ukrainian doctors; they asked which of my patients receive insulin and how much it costs. The database stores confidential information, accessible only to the doctor. In addition to home addresses and phone numbers, it stores passport data and contact information. Special population groups are also indicated, including veterans of [Ukraine’s] Anti-Terrorist Operation [which ended in 2018].[303] I was worried, because the week before, I had received a patient from the occupied city of Mykolaiv oblast; he was a former member of the Anti-Terrorist Operation suffering from diabetes. The Russians found out about his illness, arrested him, and waited for him to die slowly without insulin. The man somehow managed to escape. I gave him the contacts of acquaintances who sheltered him.
At the second meeting, Russian forces announced the mandatory “retraining” of Ukrainian doctors and an obligation to work according to the laws of the Russian Federation.[304] They emphasized that doctors should register as Russian specialists and therefore suggested that they go to Russia to take courses and requalify as doctors. This meeting was guarded by two people armed with machine guns who did not have any distinguishing markings but wore flags of the Russian Federation on their chevrons.
On July 1, 2022, representatives of the Federal Security Service of Russia came to the Regional Clinic Hospital; they detained the director of medical affairs and the head of the hospital’s personnel department. In order to contain the doctors’ discontent, the Federal Security Service took some of the Ukrainian doctors away for “a conversation” or summoned them to the occupied Department of Health [to limit the spread of rebellion].
It was dangerous for Ukrainian doctors to work under occupation, especially in small settlements, as they could become victims of kidnappings. First, there are fewer witnesses to kidnappings in towns and villages; second, it is easier to pressure and force cooperation. The reason for the abduction could be the refusal to take Russian salaries or social assistance, or the compulsion to travel for retraining, which had been announced in June 2022. Many Kherson doctors left, but specialists who could provide emergency care remained in the city. Several private clinics also operate in Kherson, but due to the lack of specialists in narrow fields and the lack of specific equipment, their treatment options were limited.
Shortly after [I left on July 7, 2022], Russian forces drew up lists of people who were not allowed to leave, including Kherson’s health sector management. The new management of the hospital[305] told the nurses and orderlies to help them in everyday life, including by cleaning after them and washing their clothes. Doctors were forced to switch to a Russian cellphone connection.
Case Study #9
Providing Health Care under Bombardment: Mariupol Regional Intensive Care Hospital (Donetska oblast)
Dr. Oksana Kyrsanova, an anesthesiologist at the Regional Intensive Care Hospital in the city of Mariupol, spoke to MIHR researchers[306] about the occupation of the hospital by Russian forces on March 12, 2022, how doctors provided care during its occupation, and the conditions under which staff worked.[307] As a multidisciplinary medical and preventive institution, the Intensive Care Hospital was designed to provide inpatient and outpatient polyclinic care to Tsentralny, Mariupol’s largest district.
Dr. Kyrsanova personally witnessed these events or heard them from colleagues contemporaneously as she worked at the hospital from February 24 until March 15, 2022, when she escaped. She had worked part-time at the hospital since 2020. Her main place of work was the Maternity City Hospital on the left bank of the Kalmius River; however, at the end of February 2022, with Russia’s offensive already underway, she could no longer access the hospital and switched to working full time at the Regional Intensive Care Hospital. Dr. Kyrsanova’s testimony has been translated, edited, and condensed for clarity.
On February 24, 2022, around 11:00 a.m., a lot of patients started coming in, many wounded, mostly Ukrainian military personnel. The wounded were admitted almost in a coma with a lot of blood loss, in a state of shock. The doctors could not even collect medical history, find out surnames and ages. In order to keep documentation, a description of the wounded person was made on an A3 sheet, and then, if they learned the last name, they added it. On the first day, the department received 16 wounded at once, among them were two to three civilians, one of them was a young girl with very serious injuries. All operating rooms were functional. There were more doctors than usual, considering the circumstances, but still not enough. Later, the wounded soldiers were taken to the military hospital. Special aviation transported all military personnel who were stabilized to the hospital in Dnipro. The civilian population was treated at the Regional Hospital.
The hospital had a generator powering the first two floors. On the first floor, there was a reception room; on the second floor, there was an operating unit. In the first days, medics covered the generator with sandbags so that it would not be damaged, because it powered ventilators. Medics also cooked food and made hot tea from the generator to feed the patients.
On February 28, 2022, a missile hit the hospital yard.[308] It was the intensive care unit that was affected. All the windows were smashed there. The hospital lost its electricity first, then its water supply and Internet connection. Next, the mobile connection disappeared, and the hospital was cut off from the outside world. After some time, the gas went out in Mariupol, and people started cooking outside.
After February 28, very busy days began. There were many surgeries. The wounded came with various injuries: explosive, shrapnel, bullet injuries; there were children, adults, and then pregnant women. It was very difficult because there was not enough medicine. Patients needed special nutrition, antibacterial therapy, and special antibiotics that doctors could not provide. Instruments were sterilized, but it was relative sterility.
There were no windows [left] in the hospital, and the temperature was below zero outside. It was necessary to create a thermal regime so that there would be no hypothermia after operations on patients. There were also pregnant women in the hospital, so the doctors brought them a heater. The doctors stayed with the pregnant women so that the surgeons could attend the births. Every day at five or six in the morning there were air raids, air strikes, and everyone woke up from this.
Starting from March 8, 2022, doctors remained at the hospital permanently. There were a lot of sick people, civilians, and especially children in critical condition. On March 9, 2022, around 4:00 p.m., there was an airstrike on the Women’s and Children’s Health Territorial Medical Association in Mariupol. It was destroyed, and pregnant women were brought to the Regional Hospital for intensive treatment [about 3.5 kms away]. They brought six women. One pregnant woman was brought in in a very serious condition. She had a completely shattered pelvis and a torn hip. Surgeons urgently performed a caesarean section, but the child was dead. The woman had injuries incompatible with life. It was not possible to resuscitate her; she died.[309] Another pregnant woman was admitted to the operating room. Half of her foot was amputated.
By March 10 or 11, 2022, another missile had hit the hospital.[310] There was a big hole in the wall. It was between the sixth and seventh floors. The impact caused one floor to fall on top of the other. Neurosurgery was on the sixth floor and there were patients who were crushed by the slab. Doctors tried to pull them out, but it was very difficult because the ceiling had fallen.
On March 12, 2022, Russian military occupied the hospital. Their target was the hospital itself, because they could shoot from it and knew that [the Ukrainian military] would not fire back. The hospital became a human shield.
On the day of capture, I remember doctors were in the operating room, performing a caesarean section. Colleagues entered and said not to leave the room, because there were Russian soldiers in the corridor. The military did not have any chevrons or insignia, only white bandages and green uniforms. From their pronunciation it was possible to understand that they were soldiers from the “Donetsk People’s Republic,” Russians and Chechens. The most important one was from Ossetia.
The Russian military went around all the floors, making doctors and medical personnel face the wall. The men were stripped to the waist while Russians searched them for military symbols, gunpowder stains on their fingers, and imprints from the use of weapons on their shoulders. The military broke down all the doors of rooms and warehouses that were not used by doctors to check that no one was hiding there. They made our hospital their headquarters. They had a rotation, first there were some, then others came. They occupied the entire building, completely surrounded and controlled the hospital, all entrances, exits, and stairs. They were on the roof of our hospital. We had a very big building, and they had a view of everything.
And indeed, we saw it all, they [Russian forces] set up their equipment and shot from the hospital buildings. Military equipment was placed around the perimeter of the hospital. Armored personnel carriers stood on all sides of the hospital. There were snipers on the roof and top floors. There were probably four soldiers on each floor. There were a lot downstairs, probably 10 [soldiers] and three armored personnel carriers. The soldiers would rotate; the armored personnel carriers hid, for example, between two houses right in front of the windows.
The military emphasized that those who tried to leave the hospital could be shot. Doctors, medical personnel, and those who were in the hospital became hostages of the Russian military. Doctors were threatened with deportation to Russia.
The Russian military began to bring people from nearby residential buildings to the hospital. In the 17th and 23rd districts of the city, all residential buildings were completely destroyed. Soldiers approached the residents and said that it was dangerous in the city and offered to take them to a bomb shelter in the hospital. Every day, they brought 200 people to the hospital. Five floors out of eight were filled even before the hospital was taken over. All other floors and corridors were filled with civilians – children, elderly people, animals. There was no water, so it quickly became completely unsanitary … and there was no food at all. There was broken glass in the corridors, there was dried blood on the floor, scattered clothes, broken stretchers, everything was dirty. Civilians sat in such conditions. There was a terrible smell. Medicines and other materials were [also] running out. It was impossible to transport the sick to the hospital. Cars got shot from the roof of the hospital in front of the doctors … so the wounded were carried on blankets, in [people’s] arms … The dead bodies were first taken to the morgue located in the basement. Then they were taken to the mass grave.
We understood that staying in the hospital was dangerous. On March 15, 2022, when water was brought to the hospital and people began to line up, we changed into civilian clothes and went out into the yard. The military’s attention was focused on the water distribution point, so I was able to leave the hospital along with at least five other people. I ran 20 kilometers to the highway under constant shelling and explosions. On the road, I was offered a seat in a car by residents who were evacuating from Mariupol. After passing 20 Russian checkpoints, I entered the territory controlled by Ukraine.

Case Study #10
Providing Health Care in Captivity: Garrison Hospital No. 555 (Donetska oblast)
In an interview with MIHR researchers, Dr. Y,[311] a military doctor from Dnipro, recounted his living and working conditions in Mariupol. He also spoke about his captivity at several correctional colonies (Russian-operated prisons), where he provided medical care to wounded prisoners following his capture by Russian forces.[312]
In late March 2022, Dr. Y agreed to go to Mariupol to provide medical assistance, including providing support to Garrison Hospital No. 555.[313] The hospital – located in Mariupol’s Kalmius district, near the Ilyich Metallurgical Plant (Plant) – was immediately on the front line after the full-scale Russian invasion began and remained operational while most other medical facilities in Mariupol stopped functioning throughout the siege of the city. As such, wounded people were brought in from all over the city.[314]
Due to heavy bombardment, Hospital No. 555 was already non-functional by the time of Dr. Y’s arrival. Its operations had been relocated to the Plant, which is where medical personnel, including Dr. Y, sought shelter. While sheltering, the doctor treated wounded Ukrainian soldiers from the 36th Marine Brigade (under whose command he was) and other divisions, as well as civilians. On April 12, 2022, Russian forces captured all those who were sheltering at the Plant. Dr. Y was initially taken to the village of Sartana, a filtration point for correctional colonies,[315] and later transferred to the Olenivka Correctional Colony No. 120 in Volnovakha. Having survived an attack on the Olenivka Correctional Colony No. 120 on the night between July 28 and 29, 2022,[316] the doctor was eventually transferred to the Kalinin Correctional Colony No. 27 in Horlivka in late September 2022. On November 3, 2022, he was released as part of an exchange of prisoners. Dr. Y’s testimony has been translated, edited, and condensed for clarity.
Ilyich Metallurgical Plant
There were at least 300 wounded at the Plant, though the highest figure I heard was 980. These numbers were recorded by a doctor who is still in captivity. Doctors worked every day, at all hours. The large basement was completely filled with wounded civilians and soldiers. One child was present at the Plant, a 10-year-old boy who had a shrapnel injury to his face. He was with a woman; I don’t know who she was – whether she was his mother or a neighbor. There was no time to ask people who they were. The main thing for me was that he was alive and healthy. We crossed paths with them once more during the period in captivity while in Sartana, but I do not know their fate.
During the entire period of stay at the Plant, in addition to providing support to the units, medics dealt with logistics, fed, transported, and generally took care of the wounded. We could not simply surrender, as we were a support unit, working for the brigade, and could thus not operate separately from the main military unit. If there were no medicines available, the commander would go outside to get it. We don’t know how he did it, but we always had everything we needed. We worked as part of the medical and nursing team at the Plant until April 12, 2022. On that day, we surrendered to the Russian military by order of the commander of the 36th Brigade.
Sartana
In Sartana, we were received by people without identification marks or chevrons, it was not clear who they were. We could only understand they were not “our people” by listening to their accents. We would immediately hear if someone was from the “Donetsk People’s Republic” and “Luhansk People’s Republic.”
During the first night in captivity, we were not sorted, we were all taken in a row to the barracks. Later, women were separated, they were taken somewhere [else]. All our things were taken away from us, including medicines and things to keep warm. One of our doctors had to hand his sleeping bag: he threw it on the ground, together with his badge. The guards witnessed the scene, called him up, and after asking who he was, they separated the medics, who were ordered to treat the prisoners.
There were many wounded, and something had to be done with them. A separate barrack was set aside for captured medics to treat the less severe injuries. We were reminded that we should be grateful to be alive, that we were not killed. In essence, it was “be happy we did not kill you.”
We treated the wounded and did everything we could as we used to do in Mariupol, but the working conditions were much worse. They did not give us anything except one bag filled with individual bandage packages and some medicines. It was some of the medicines that they took from us when we were taken prisoner. The way we were forced to treat people is not medical care. There was no access to adequate facilities and supplies to provide appropriate care. What kind of medical care is this? We need to treat people in a hospital, not just keep them in a barrack and be happy to have a bag of first-aid kit bandages.
There was not enough drinking water for the number of people in the barracks and we were given some kind of bread and one can of food to share with several people. There were so many wounded prisoners to be cared for that we prioritized resting rather than eating or drinking. Whenever possible, we leaned against each other on the concrete floor to sleep.
We were in Sartana for three or four days. The medics and the wounded were the last ones to leave. Only the persons with the most serious injuries were sent to hospital; there were 28 of them. The rest all went with us to Olenivka.
Olenivka Correctional Colony No. 120
Upon arriving at the colony, we underwent an “admission” procedure. As soon as we got off the bus, the jailers identified and continued to beat us: while we were saying our names, then again along a corridor they formed, and finally after they forced us to squat down. There was constant physical violence. They could have let this bus in without this “ritual,” everyone knew the bus was carrying wounded people and doctors. But the wounded were not spared. There was a guy with a crutch; they took the crutch from him and beat him with it, even as he fell to the ground. A wounded prisoner of war, who survived two airstrikes and had facial burns, was beaten to death. The head of the colony approached, and this is how I understood that there was some kind of ban on such a severe beating. I was in line after him; if it was not for his death, I would have been beaten just as hard.
The medics and the wounded were all placed in the same barrack and were forced to sleep on the floor. Several wounded had broken and torn limbs, some were paralyzed, they were in pain, but they were forced to live in such conditions. Initially, all the wounded – including those who were unable to walk due to their injuries – were forced to line up and walk 50 meters to the canteen. Food was eventually allowed to be brought to the barracks for the wounded, but this was subject to sudden change, depending on guards’ shifts. Physical force at that point was only used in the disciplinary isolation ward as a punishment for violating rules. But we were under constant moral pressure. We were forced to sing both the [Russian national] anthem and other songs.
“Admission” procedure at the Olenivka Correctional Colony No.120 – a MIHR investigation[317]
Detainees stayed in transit camps for up to a week before being transferred to Olenivka Correctional Colony No. 120. “We stood on our knees. Some people were beaten very hard. When we looked around, we realized that it was a former [temporary detention facility]. There were about 30-40 people in the cell,” a detainee who was released told MIHR regarding conditions in one of the transit camps.
Upon transfer to Olenivka, detainees were forced to sit for hours in “slav squat,” a position requiring them to lock their hands behind their neck and squat, heels to the ground. Those who moved were beaten with clubs and rubber batons or kicked. Detained soldiers were also stripped naked.
Before being transferred to barracks, where detainees were forced to work, most were sent to a “punitive segregation unit” comprised of 15-square-meter cells in which up to 55 people were kept at the same time. There, meals consisted of a loaf of bread for eight prisoners per day and 200 ml of water per person per day.
There were 2,000 people in the colony, but not enough medicine to treat all the injured. From April to October 2022, no official medicines were delivered from Russia or the Red Cross in the colony. Everything the medics managed to obtain in this period was thanks to the diplomacy of one captured doctor. These medicines were the same [ones] that were confiscated upon the medics’ arrival into the colony. It was only in October 2022 that Russians brought medicines to the colony for the first time. They were not interested in providing medical care but only in avoiding deaths.
All assistance was based on human relations with the administration. When there were strokes, heart attacks, the senior medic could turn to the colony management and ask to send the patient to the hospital. But, if the chief was not in the mood, then the wounded prisoners would die. There were also women in captivity, one of them was pregnant. A senior medic contacted her. When the story of the pregnant woman became public, she was provided with vitamins, but was not released from captivity. She was later transferred to the hospital [in Sartana].
On the night of July 28-29, 2022, we heard cries in the colony. One of the leaders of the colony came and informed us that help was needed quickly. At the time when we got there, the entire road was covered with bodies. We were told that 47 persons died on the spot as a result of the explosion, and 116 were wounded. Representatives of the administration did not organize the evacuation, they watched us rescue the wounded all night. All they did to help was to provide some torn rags to be used as bandage material. Those who were less severely wounded were left at the colony, in a disciplinary isolation ward, with 20 injured people stuffed into four-bed wards. Five of them died during the night. Four had a combat craniocerebral injury, one had bleeding that could not be stopped. In general, the majority were craniocerebral injuries. If these people had been evacuated earlier, they might have survived.
Legal Framework and Analysis
This section explains the relevant rules and principles of international humanitarian law (IHL) that govern the conduct of parties in armed conflict, and the protected status of health facilities. The section then analyzes how the attacks detailed in the case studies above could give rise to criminal liability at both the international level under the Rome Statute of the International Criminal Court (ICC) and the domestic level under the Criminal Code of Ukraine (CCU) of 2001[318] and through the exercise of universal jurisdiction in other countries.[319] A special tribunal for aggression – another avenue relevant to Russia’s full-scale invasion of Ukraine – is currently being envisaged, but it is not examined here.[320]
International Humanitarian Law
IHL is the body of laws that applies to armed conflicts.[321] As parties to an international armed conflict,[322] Russia and Ukraine are equally bound to comply.[323] This body of law is enshrined in the four Geneva Conventions of 1949 and their Additional Protocol I of 1977, [324] and in the Hague Conventions of 1899 and 1907.[325] Collectively, these instruments seek to protect those who do not or are no longer participating in the hostilities and to restrict the means (i.e. weapons) and method (i.e. tactics) of warfare. Many of the rules contained in these instruments also have the status of customary international law, consisting in a general practice accepted as law by states.
At the heart of the IHL framework lie several interrelated principles and legal obligations, which together lay the basis for the protection of civilians generally and special protections for health care. In a comprehensive report covering the initial five weeks of the full-scale Russian invasion of Ukraine (First Report), the Organization for Security and Co-operation in Europe (OSCE) Moscow Mechanism[326] found “clear patterns of IHL violations by the Russian forces in their conduct of hostilities.” In particular, the Mechanism noted that “[i]f they had respected their IHL obligations in terms of distinction, proportionality and precautions in attack and concerning specially protected objects such as hospitals, the number of civilians killed or injured would have remained much lower.”[327] These obligations are detailed in turn below:
Distinction. Under the principle of distinction, parties to a conflict must always distinguish between civilians and civilian objects on the one hand[328] and combatants and military objects on the other.[329] The principle of distinction means that operations may be directed only against combatants and military objects, an obligation that translates into a prohibition of attacks against civilians and civilian objects,[330] unless the protections have been suspended due to the civilian directly participating in hostilities[331] or the civilian object is being used for military purposes.[332] In other words, “what counts for IHL is not what was destroyed or who was killed or injured but what and who was targeted.”[333] In its First Report, and with reference to the conduct of Russian forces, the OSCE Moscow Mechanism found that “it is highly implausible that so many civilian buildings, in particular, those situated far away from actual fighting between ground forces, had thus turned into military objectives or that so many of them were destroyed by mistake while a military objective was targeted.”[334]
Proportionality. Even where the principle of distinction is respected – and combatants or military objectives are targeted – an attack violates the principle of proportionality if the expected incidental death of, or injury to, civilians or the expected damage to civilian objects is excessive in relation to the anticipated military advantage.[335] Prior to targeting a military object, if damage to civilian objects or civilian death or injury is anticipated, an assessment must be undertaken in which the anticipated military advantage to be gained is weighed against the “collateral” damage to protected civilians or civilian objects that is anticipated. Thus, under IHL, not every attack that results in civilian death or injury, or the destruction of a civilian object, is prohibited. In its First Report, the OSCE Moscow Mechanism found it “highly implausible … that in each case in which civilians were killed, the military advantage sought was so important that it justified the impact on civilians which had to be expected in an urban area.”[336] The Mechanism further concluded that even where military objectives were targeted, Russia should not only have taken into account the incidental effects on civilians or civilian objects near the target, “but also reverberating effects” such as “interruptions of electricity, gas, heating and water supplies … including their impact on the health system.”[337]
Precaution. Parties to a conflict must also respect the principle of precaution and take constant care “to spare the civilian population, civilians and civilian objects” in order to minimize any incidental loss of civilian life, injury to civilians, and damage to civilian objects.[338] In particular, they must: (1) verify that the objectives to be attacked are neither civilians nor civilian objects and are not subject to special protection;[339] (2) give advance warning of attacks which may affect the civilian population, if possible;[340] (3) cancel or suspend an attack if it becomes apparent that the principles of distinction or proportionality may be violated;[341] and (4) chose means and methods of warfare to at least minimize incidental death of, or injury to, civilians and damage to civilian objects.[342] In its First Report, the OSCE Moscow Mechanism found it “particularly implausible” that Russia respected the principle of precaution or that it was not feasible “to choose weapons, ammunitions, tactics and timings other than those which it actually used” in densely populated areas.[343] The Mechanism further concluded that it is “highly implausible that the undisputed use of cluster munitions, munitions with a large blast radius, such as large bombs or missiles, unguided missiles, artillery and mortars, multiple launch rocket systems (MLRS) and dumb bombs released by aircraft … in densely populated areas, was in each case the only feasible choice for the Russian commander.”[344]
Medical Personnel, Units, and Vehicles. In addition to the general rule prohibiting attacks on civilians and civilian objects, IHL affords specific, enhanced protection to medical personnel,[345] medical units,[346] and medical vehicles.[347] This is due to “their primary importance during armed conflicts, both to maintain public health and to care for the wounded and sick caused by the armed conflict” and applies regardless of whether they are military or civilian.[348] They shall be respected and protected at all times by the parties to an armed conflict.[349]
Similarly, IHL and human rights law, along with medical ethics, frame the rights and responsibilities of health care professionals, which includes the principle of medical impartiality. Medical impartiality requires that medical personnel not be punished for acting in accordance with their ethics and to ensure the protection of medical personnel, patients, facilities, and transport from attack or interference.[350] For those delivering assistance to affected populations, the humanitarian principles of impartiality, neutrality, and independence are essential to facilitate access to those in need of aid, including support for the health system.
The prohibition on directing attacks is not absolute: medical personnel, units, and vehicles lose their protection where they are used, outside their humanitarian function, to commit acts harmful to the enemy.[351] Acts not considered “harmful to the enemy,” which therefore do not lead to a loss of protection include, for example: when a hospital is guarded by an escort made up of soldiers or uniformed police force[352] or when members of the armed forces are in the hospital or unit for medical reasons.[353] By contrast, hospitals and other medical units lose their protection when they are, for example, used as a shelter for able-bodied combatants, as an arms or ammunition dump, or as a military observation post.[354] In such case, the hospital becomes a legitimate military objective, but only “after a warning has been given setting, whenever appropriate, a reasonable time-limit, and after such warning has remained unheeded.”[355] However, even in the case of loss of special protection, the general protection afforded to civilians and civilian objects applies and a “proportionality evaluation has to be made between the military advantage of stopping the acts harmful for the attacker and the expected death and injury of the medical personnel and current and future patients.”[356]
In its First Report, the OSCE Moscow Mechanism found that the large number of affected health care facilities in Ukraine between February 24 and March 22, 2022 cannot be explained even “assuming that some attacks were directed against facilities engaged in acts harmful to the enemy or were incidentally harmed by attacks against legitimate targets.”[357] Additionally, even in the one instance in which Russia claimed to have issued the necessary warning, the Mechanism found that it had done so “without a time-limit and without any indication what had to be done to preserve the special protection.”[358] The Mechanism thus concluded that the special protection afforded to health care facilities had never been lost, rendering any of the intentional attacks directed against the structures war crimes.[359]
Certain violations of IHL may constitute war crimes and, if widespread or systematic, and committed pursuant to or in furtherance of a state or organizational policy, may also constitute crimes against humanity. Indeed:
The Geneva Conventions and Additional Protocol I establish that certain violations of IHL are to be considered “grave breaches”, and they must be prosecuted by High Contracting Parties, including on the basis of the principle of universal jurisdiction. Individual criminal responsibility for other serious violations of IHL is established by customary international law and by international criminal law treaties [such as the Rome Statute of the International Criminal Court]. Such serious violations of IHL, together with grave breaches, constitute war crimes.… Certain acts violating IHL, including war crimes, such as murder, extermination, or deportation may also constitute crimes against humanity, if they are committed “as part of a widespread or systematic attack directed against any civilian population, with knowledge of the attack”.[360]
Avenues for Accountability
Ukrainian courts have primary jurisdiction to adjudicate crimes committed within the country. However, in relation to international crimes, both the ICC and third countries can serve – with some limitations discussed below – as important additional avenues for accountability.
War crimes can be prosecuted under the Criminal Code of Ukraine (CCU), at the International Criminal Court (ICC), and by third countries pursuant to universal jurisdiction. Crimes against humanity can be prosecuted by third countries under both the principle of universal jurisdiction and at the ICC under the Rome Statute. The latter provides the most commonly accepted definition of crimes against humanity,[361] defining them as certain acts of violence – including what the Statute calls “other inhumane acts” – that are carried out as part of a widespread or systematic attack against a civilian population.[362] This definition is largely accepted by third countries exercising the principle of universal jurisdiction.[363] While the notion of crimes against humanity is currently absent from Ukrainian law, proposed amendments to Ukraine’s Criminal Code replicate the Rome Statute definition of the crime verbatim.[364]
Neither Ukraine nor Russia are state parties to the ICC. On January 20, 2000, the Ukrainian Parliament signed the Rome Statute but never ratified it.[365] However, in 2014 and 2015, Ukraine lodged two declarations pursuant to Article 12(3) of the Rome Statute, effectively accepting the ICC’s jurisdiction over alleged crimes committed on its territory. The first declaration granted the ICC jurisdiction over crimes allegedly committed from November 21, 2013 to February 22, 2014 in relation to the Maidan protests.[366] Accordingly, in April 2014, former ICC prosecutor Fatou Bensouda opened a preliminary examination of the situation in Ukraine limited to these events.[367] The second declaration covered crimes allegedly committed in Ukraine from February 20, 2014 onwards,[368] which prompted the ICC to extend its preliminary examination to include alleged crimes committed there.[369]
In December 2020, the Office of the Prosecutor concluded its preliminary examination and determined that there was reasonable basis to seek the opening of an investigation into the “Situation in Ukraine.”[370] In the meantime, Ukraine’s parliament also amended Article 124 of the Constitution to recognize the jurisdiction of the ICC, thus removing all legal obstacles to ratification of the Rome Statute.[371]
On March 2, 2022, following Russia’s full-scale invasion of Ukraine, ICC Prosecutor Karim A.A. Khan, KC opened an investigation into the “Situation in Ukraine” on the basis of an unprecedented joint referral by 43 state parties.[372] As such, even without Ukraine or Russia being state parties to the Rome Statute, and in absence of a referral from the United Nations Security Council, the ICC has jurisdiction to investigate and prosecute those who commit Rome Statute crimes in Ukraine, such as war crimes and crimes against humanity, including those at the highest level of the Russian military and its political apparatus. Importantly, the ICC is also mandated to investigate crimes committed by all parties to the conflict.
However, there are crimes particularly relevant to attacks on health care in Ukraine that the ICC cannot prosecute, such as the prohibition on the use of certain weapons which, despite being listed as a war crime under the Rome Statute, is not currently in force for lack of an annex listing the prohibited weapons,[373] or certain attacks against humanitarian corridors.[374] Nevertheless, certain countries that have adopted a wider definition of war crimes and who are able – under universal jurisdiction statutes – to prosecute such crimes may still be an available forum to do so. In addition, as a matter of policy, the ICC Prosecutor focuses its resources on “the investigation and prosecution of a limited number of mid- and high-level perpetrators,” while not precluding the prosecution of lower-level perpetrators “where their conduct has been particularly grave or notorious.”[375]
Gaps in the prosecution of certain crimes or certain perpetrators at the domestic and international levels can be filled by third countries exercising universal jurisdiction, which allows them to prosecute serious crimes under international law, like war crimes or crimes against humanity, regardless of where they were committed or of the nationality of the perpetrators and the victims. These countries incorporate the crimes listed in the international conventions they ratified, such as the Geneva Conventions, the Convention against Torture, and the Rome Statute. Since the beginning of the full-scale Russian invasion, several third countries have opened investigations into crimes allegedly committed in Ukraine.
This section analyzes attacks on health care in Ukraine in light of relevant war crimes under Article 8(2)(a) and (b) and crimes against humanity under Article 7 of the Rome Statute. As noted, analysis under the Rome Statute is relevant for both the ICC and other, domestic jurisdictions that may have implemented it into their penal code or, indeed, have criminalized provisions that the ICC cannot yet prosecute (e.g., the use of certain prohibited weapons). The analysis relies on the “reasonable basis” standard that the ICC Prosecutor must satisfy when seeking the opening of an investigation.[376] Under this standard, the information gathered is “not expected to be ‘comprehensive’ or ‘conclusive’”; rather, a “sensible or reasonable justification [must] exist for the belief that a crime falling with the jurisdiction of the Court ‘has been or is being committed.’”[377] However, the report does not identify individual suspected perpetrators responsible for the attacks outlined in the case studies above, but rather recommends the Office of the Prosecutor at the ICC to investigate cases of attacks on health care.
Under the Rome Statute, a single attack may amount to a war crime.[378] However, the Rome Statute also adds that the ICC has jurisdiction over war crimes “in particular when committed as part of a plan or policy or as part of a large-scale commission of such crimes.”[379] While this sentence should not be interpreted as limiting the jurisdiction of the ICC,[380] it gives the ICC “a particular guideline”[381] over war crime prosecutions. By contrast, to establish the existence of an attack as a crime against humanity, the Rome Statute requires a “course of conduct” involving the multiple commission of acts against a civilian population, “pursuant to or in furtherance of a state or organizational policy.”[382] Establishing the existence of a policy is therefore, at a minimum, relevant for assessing evidence of war crimes, but required for the prosecution of crimes against humanity before the ICC.[383]
A policy does not need to be clear from the outset but may crystalize over time “such that definition of the overall policy is possible only in retrospect, once the acts have been committed and in light of the overall operation or course of conduct pursued.”[384] Even if a policy is not explicitly defined, it can still be “surmised from the occurrence of a series of events.”[385]
ICC jurisprudence has adopted the factors set out by the International Criminal Tribunal for the former Yugoslavia (ICTY) to assess the existence of a policy.[386] These include, among others: (1) the “general historical circumstances and the overall political background against which the criminal acts are set”; (2) the “mobilization of armed forces”; (3) the “scale of the acts of violence perpetrated,” including “the destruction of non-military property”; and (4) the existence of “temporally and geographically repeated and coordinated military offensives.”[387] In most cases, a policy implies a regular pattern and can be inferred from “repeated actions according to the same sequence, or the existence of preparations or collective mobilization orchestrated and coordinated” by a state.[388]
War Crimes under the Rome Statute
A threshold question for war crimes analysis is whether an armed conflict exists.[389] The Rome Statute gives the ICC jurisdiction over alleged war crimes committed in international armed conflicts,[390] which the Russia-Ukraine war undoubtedly is, as well as non-international armed conflicts. Under this framework, war crimes require two contextual elements: (1) that the conduct “took place in the context of and was associated with” an international conflict and (2) that the perpetrator was aware of factual circumstances that established the existence of an armed conflict. In most cases, this can be shown by the perpetrator’s awareness of the link between their conduct and the conflict.[391]
Many of the incidents described in the case studies above may, in themselves, constitute war crimes. Their combination, along with all other reported incidents in the dataset, appears to indicate the existence of a plan or policy to attack Ukraine’s health care system or, at a minimum, the large-scale commission of these attacks. As noted, these are not a strict requirement for the exercise of the ICC’s jurisdiction over war crimes,[392] but serve as a “particular guideline for the Court.”[393] While all incidents demand further investigation by the ICC Prosecutor, key elements of these crimes and their application to the alleged role of the Russian forces in attacks on Ukraine’s health care system are described below:
Attacking Protected Objects (Article 8(2)(b)(ix)): The special protection afforded to protected objects is rooted in the IHL principle of distinction and the general prohibition against attacking civilian objects.[394] Under the Rome Statute, protected objects include hospitals and places where the sick and wounded are collected. ICC jurisprudence makes it clear that protected objects “deserve special protection because of the role [they] play in the daily life and welfare of the civilian population.”[395] This protection must be respected “[e]specially in times of armed conflict and during ongoing hostilities, when as a result of the fighting more persons become injured or wounded… Attacking such structures disrupts the ability of medical personnel to care for the sick and wounded.”[396]
To fall within the meaning of Article 8(2)(b)(ix) of the Rome Statute, the perpetrator must not only have intended to launch an attack, but also have been aware of the target’s protected status – for example, if it was known to be a medical facility or was indicated by the emblems of the Geneva Conventions or other distinctive signs[397] – andintended it to be the object of the attack.[398] These requirements mean that hospitals, as protected objects, must be the primary object of the attack.[399] The attack itself, however, does not require a particular result; in other words, it does not matter if a hospital did not suffer damage as a result of the attack.[400]
Hospitals are protected objects unless and for so long as they are military objectives, i.e., used to commit acts harmful to the enemy outside their humanitarian function.[401] For instance, the presence of armed forces in a hospital for medical reasons is not an act harmful to the enemy and does not deprive a hospital of its protected status.[402] Further, even if a hospital might become a military objective, its special protection against attacks ceases only after a warning has been given and such warning is ignored.[403]
There is a reasonable basis to believe that Russian forces intentionally attacked hospitals, as protected objects, on several occasions following the onset of the invasion. By targeting functioning hospitals, Russian forces not only severely endangered the welfare and lives of patients receiving care as well as medical personnel, but also further disrupted future medical care for those in need.
The April 19, 2022 strike on the Bashtanka Multiprofile Hospital is illustrative (case study #4). There are reasonable indications that Russian forces were aware that it was a medical facility: according to the hospital director, drones flew over the hospital and “saw very well” the Red Cross painted on a white canvas placed on the roof of the facility.[404] A cursory online search also reveals the hospital’s geo-coordinates and its location on the edge of the city alongside two other hospital campuses. The hospital had retained its status as a protected object: Ukrainian forces were not stationed there, there does not appear to have been prior or contemporaneous reports of military activities in or around the hospital, and the hospital’s staff was in the midst of providing care to patients at the time of the attack. Its relatively isolated position on the edge of the city,
its potential strategic importance to observe the advance of Russian troops towards the city of Mykolaiv, and the use of a precision-guided missile – which the Russian media claimed in 2017 had an accuracy of within 30 meters[405] and whose launch requires high-level clearance due to its high cost and low availability[406] – are indications that Russian forces may have intended to strike the hospital. The attack resulted in the destruction of 30-40 percent of the hospital’s premises.


Other examples include the series of attacks directly aimed at the Trostianets City Hospital between March 18 and March 25, 2022 (case study #5). Like the Bashtanka Multiprofile Hospital, the Trostianets City Hospital was marked with the emblem of the Red Cross. At the time of the attacks, Ukrainian forces were fighting to liberate the city of Trostianets from Russian occupation.[407] While Ukrainian forces may have been in the vicinity of the hospital or on the grounds of the hospital on one occasion and fighting ensued between Ukrainian and Russian forces across the street, the hospital’s location near legitimate military targets alone did not deprive it of its protected status. In fact, the hospital continued to operate exclusively as a medical facility, albeit at reduced capacity, by providing care to incoming patients. Despite its protected status, Russian forces allegedly set up two military posts behind and in front of the hospital, mined the area around it, and used tanks to repeatedly shell the hospital.[408] On March 19, 2022, an armed Russian soldier also reportedly entered the building and fired inside the premises. The series of attacks resulted in the destruction of the Trostianets City Hospital’s gynecology, maternity, and surgical wards, infectious diseases department, and overall structure.
Other incidents falling into this category of war crimes possibly include attacks on three health care facilities which, while located near the fighting line, do not appear to have become legitimate military objectives. These are:
- The February 26, 2022 attack by machine gun on the Makariv Multiprofile Intensive Care Hospital (case study #2);
- The attack on the Makariv Primary Care Clinic, if it was prior to the March 7 evacuation, reportedly carried out by successive, adjusted mortar strikes until the facility was hit (case study #2); and
- The April 2, 2022 shelling of the Balakliia Clinical Multiprofile Intensive Care Hospital prior to its seizure by Russian forces a day later (case study #7).
Excessive incidental death, injury, or damage (Article 8(2)(b)(iv)): This provision reflects, as the International Committee of the Red Cross has noted, the IHL prohibition on indiscriminate attacks.[409] It criminalizes attacks launched against a military target[410] that would result in death, injury, or damage that is clearly excessive in relation to the “concrete and overall military advantage anticipated.”[411] This assessment must be made before launching the attack.[412] Crucially, however, the attack itself does not require a particular result: as one commentator notes, “the crime would be committed even if, for example, an attack was launched against a military objective, but due to the failure of the weapon system, the expected excessive incidental damage did not occur.”[413]
There is a reasonable basis to believe that Russian forces engaged in attacks that may have resulted in excessive damage to civilian areas, including health care facilities. In the examples below, the assessment of whether the damage was excessive in relation to the military advantage gained in the attacks – and therefore whether the attacks fall under Article 8(2)(b)(iv) – would presuppose knowledge of what advantage Russian forces where seeking; a task that lies with investigators. At a minimum, there is a reasonable basis to believe an investigation into these incidents is warranted.
One such example can be found in the attacks that resulted in the damage of the Izium Central City Hospital,[414] including at least one attack that struck the facility directly, reportedly launched with the use of wide-area effect weapons such as large conventional artillery rounds or unguided air bombs (case study #1). The hospital had not lost its special protection: the fact that the hospital cared for wounded soldiers[415] or that Ukrainian soldiers had possibly established a base in a building nearby did not make it a military objective. Nor does it seem that any of the attacks were specifically directed at the facility. Rather, it appears that the hospital was hit in attempts to strike Ukrainian forces possibly positioned in the area or in wider operations targeting the whole city center of Izium. Even if Russian forces targeted legitimate military objectives near the hospital, the type of weapons employed – which were specifically designed to be inaccurate so that a barrage of rockets covers a wide area – resulted in the severe damage of parts of the hospital, including the complete destruction of the intensive care unit and operating block, and most buildings located within 500 meters.
Russian forces appear to have engaged in similar tactics in civilian areas of Chernihiv, including where hospitals are concentrated. The Chernihiv Regional Children’s Hospital was struck in one such attack (case study #3). On March 17, 2022, a BM-27 Uragan MLRS with warheads containing cluster munitions was reportedly launched from Russian-controlled areas towards the city center of Chernihiv. The hospital had not become a military objective: at the time of the attack, civilians were sheltering inside the facility while patients were receiving medical care. The fact that the hospital was at some point guarded did not make it a military objective.[416] Even if there had been military targets in the area, Russian forces not only used a type of weapon incapable of destroying only these objectives, but also appear to have failed to assess whether launching the attack in a densely populated area would result in excessive casualties or damage in relation to the military advantage anticipated. As established, the number of casualties – with at least 14 killed and 26 injured – and the damage caused to the hospital were significant.
Similarly, on or around March 12, 2022, the Adonis Medical Center in Makariv was struck in a series of airstrikes reportedly launched by Russian forces that caused significant damage to several other civilian objects – including apartment buildings and schools – in the city center of Makariv (case study #2). While the city was under heavy fighting between Ukrainian and Russian forces at the time, the widespread destruction of the area suggests the Russian forces’ disregard for the incidental damage caused to civilian objects around.
Attacking Objects Using the Emblems of the Geneva Conventions (Article 8(2)(b)(xxiv)): Recognized emblems of the Geneva Conventions are those of the Red Cross, the Red Crescent, the Red Lion and the Sun, the Red Crystal and any “other method of identification indicating protection under the Geneva Conventions” such as light signals, radio signals, or electronic identification. This provision expands on the war crime of attacking protected objects criminalized under Article 8(2)(b)(ix) of the Rome Statute in that it also covers, among others, attacks on medical units or transports. Identical to the war crime of attacking protected objects, the war crime of attacking objects using the emblems of the Geneva Conventions does not require that the object was destroyed or damaged as a result of the attack.[417]
The attacks on the Bashtanka Multiprofile Hospital and the Trostianets City Hospital (cases study #4 and #5, respectively), both of which were reportedly marked with a Red Cross, and the March 12 destruction, reportedly by Russian forces, of an ambulance station in Trostianets (see “Attacks on Ambulances”) may fall under this category of war crimes.
There is also a reasonable basis to believe that ambulances using distinctive signals identifying them as medical transport have been routinely and intentionally struck by Russian forces. For example, on April 18, the ambulance in Lyman was shot several times, causing it to fall into a ditch, while responding to an emergency call (case study #6). The dozen bullets shot towards the moving vehicle suggests that the attack was deliberate. The paramedic who was in the ambulance at the time also had the impression that the “target of the shots was the ambulance.” There are other examples of apparent intentional attacks on ambulances marked with emblems of the Geneva Conventions, several of which led to the injury or death of medical personnel and patients:
- On February 26, 2022, Russian forces reportedly shot at an ambulance transporting a wounded soldier in Khersonska oblast;
- On February 27, 2022, a presumed Russian group shot at an ambulance 17 times in Poltavska oblast; and
- On March 4, 2022, Russian forces reportedly shot at an ambulance with small arms in Sumska oblast.
Pillaging (Article 8(2)(b)(xvi)): The Rome Statute prohibits “all forms of appropriation, public or private, including organized and systematic appropriation, as well as acts of appropriation committed by combatants in their own interest.”[418] As such, the provision requires the perpetrator to appropriate certain property[419] without the consent of the owner,[420] for private or personal use.[421] By contrast, seizing the enemy’s property (Article 8(2)(b)(xiii)) only covers property protected from seizure under IHL.[422] Aside from the nature of the property, the perpetrator’s intent to obtain the property for private or personal use is the main distinctive element between pillage and seizure of the enemy’s property, where such requirement does not need to be met.[423] Under both provisions, however, appropriations of property justified by military necessity do not constitute war crimes.[424]
There is a reasonable basis to believe that, on several occasions, Russian forces and individuals appropriated medical supplies, equipment, and transport belonging to Ukraine, that were protected from seizure under IHL. In the examples below, the assessment of whether such appropriations were justified based on military necessity and whether they intended to appropriate them for private or personal use may only be conducted based on additional investigations into each separate incident. For example, from March 2022, Russian “entrepreneurs” allegedly seized several Ukrainian pharmacies to sell Russian medicine in the Khersonska oblast (case study #8). Between April and September 2022, Russian forces reportedly stole most of the equipment they could carry from the Balakliia Clinical Multiprofile Intensive Care Hospital (case study #7), where they had established a base, including ultrasound machines, cardiographs, encephalography machines, the CT scanner’s electronics, and surgical stands. Similarly, following the series of attacks on Trostianets City Hospital between March 18 and March 25, 2022, Russian forces allegedly stole the only undamaged ambulance left, leaving medical personnel unable to provide care outside of the hospital (see “Attacks on Ambulances”).
The case studies in this report highlight a number of other war crimes likely committed by Russian forces in Ukraine:[425]
Using Protected Persons as Shields (Article 8(2)(b)(xxiii): The prohibition against moving or otherwise taking advantage of the location of civilians, prisoners of war, or medical personnel with the specific intent to protect military objectives, or to aid or prevent a military operation, is rooted in the IHL principle of distinction. The provision is violated regardless of whether the human shields were actually attacked or harmed: indeed, the prohibition is designed to protect civilians and other protected persons from being exposed to the risk of harm, and not only to the harm itself.[426] For example, there is a reasonable basis to believe that Russian forces and allies seized the Regional Intensive Care Hospital in Mariupol and effectively compelled medical personnel to remain in the premises (case study #9). Whether this was in an effort to shield their forces from attacks depends on further investigations by relevant authorities. The following facts are relevant to this assessment: following missile strikes on the hospital between February 28 and March 12, 2022, Russian forces and allies reportedly began occupying the hospital: they placed armed personnel carriers around the premises, stationed soldiers on each floor and snipers on the roof, threatened to shoot anyone attempting to venture outside, and brought in up to 200 civilians, including children and the elderly, per day.
Unlawful Confinement (Article 8(2)(a)(vii)-2): While the movement of protected persons during armed conflicts may be restricted, or even temporarily suppressed, the justification for their confinement must be limited to valid needs and follow procedural requirements, such as an opportunity to contest their confinement.[427] In addition to the unlawful confinement of medical personnel at the Mariupol Regional Intensive Care Hospital (case study #9), several other incidents discussed above provide a reasonable basis to believe that Russian forces unlawfully confined medical personnel and other protected persons elsewhere in the oblast. For instance, Dr. Y and his colleagues were captured on April 12, 2022 and successively transferred to several correctional colonies controlled by Russian forces (case study #10). There, the medics were held in poor conditions, given insufficient supplies to treat the wounded, and witnessed prisoners being beaten or left to die.
Torture (Article 8(2)(a)(ii)-1)) and Inhuman Treatment (Article 8(2)(a)(ii)-2)): Torture is the intentional infliction of severe pain or suffering, whether physical or mental, upon a protected person for the purpose of, among others, obtaining information, punishment, intimidation, or coercion.[428] Inhuman treatment does not require such purpose.[429] Between August and October 2022, the United Nations Human Rights Monitoring Mission in Ukraine “documented widespread practices of torture and ill-treatment in places of internment in the Russian Federation and in Ukrainian territory it occupies.”[430] This is consistent with doctors held in captivity at the Russian-controlled correctional colonies of Olenivka and Horlivka (Donetska oblast) (case study #10). There, doctors, like other prisoners, underwent the so-called “admission procedure” and were beaten by guards, but also witnessed guards denying care to injured prisoners and intentionally inflicting pain and suffering on the detainees. Witnessing this treatment likely caused severe mental suffering, which was worsened by doctors’ inability to provide proper medical care to wounded prisoners, due to the unavailability of adequate medicines and facilities. Further, the conditions in which they were held – including overcrowding, lack of beds, and inadequate access to food and water – fell short of the minimum standard of humane detention, which may, at the very least, qualify as inhuman treatment.[431]
Wilful killing (Article 8(2)(a)(i)): Wilful killing occurs when the conduct of the perpetrator was the substantial cause for the death[432] of a protected person.[433] A striking example can be found in the reported shooting by Russian troops ofan ambulance that was transporting a wounded soldier to a hospital in Kherson. As a result, the ambulance caught fire, causing the death of both the driver and the patient, as well as the injury of a paramedic (p. X). Another example includes the treatment of prisoners in the Russian-controlled correctional colonies of Olenivka and Horlivka (Donetsk oblast), where medical personnel witnessed many people dying as a result of insufficient medical supplies, lack of sanitary conditions, refusal to evacuate patients to the hospital, and extreme beatings (case study #10). According to one of the medics who was held captive, wounded prisoners would be left to die “if the chief was not in the mood” to evacuate them. On another occasion, a wounded man was beaten to death at Olenivka.
Crimes Against Humanity under the Rome Statute
Between February 24 and December 31, 2022, partner organizations have documented 292 incidents that resulted in damage or destruction of hospitals and clinics, 65 incidents that resulted in the damage or destruction of ambulances, and 86 incidents, including detention and inhumane treatment, as well as injury and death, that affected health care workers.[434] The case studies above provide detailed information into some of these incidents. While each incident requires further investigation by relevant authorities, the volume of information appears sufficient to, at a minimum, warrant an investigation into whether attacks on Ukraine’s health care system are constitutive of crimes against humanity.
Crimes against humanity are specific acts, such as murder, imprisonment, torture, and, importantly, other inhumane acts, listed in Article 7(1) of the Rome Statute, “committed as part of a widespread or systematic attack directed against any civilian population, with knowledge of the attack.” For a specific act to fall under the definition of crimes against humanity, the ICC identifies “chapeau elements,” namely: (1) that an attack is directed against a civilian population; (2) that the attack is widespread or systematic; (3) that there is a link between the individual act and the attack; and (4) that the perpetrator knew their act to be part of the attack.[435]
As noted, the existence of a state or organizational policy is a pre-requisite to establish the existence of an attack as a crime against humanity.[436] Taking into account relevant factors set out by the ICTY[437] – and adopted by the ICC,[438] – some elements that need to be considered include:
The general historical circumstances and political background: Russia’s “thorough aspiration to dominate Ukraine politically, militarily, and economically” predates the 2022 invasion of Ukraine.[439] It stretches back to at least 2014, when Russian President Vladimir Putin moved to illegally occupy Crimea and supported pro-Russia separatists in the Donbas region[440] – which he continues to date. On February 21, 2022, only days before launching the full-scale invasion of Ukraine, President Putin made a speech denying the existence of Ukrainian statehood.[441] On September 30, 2022, he moved to illegally annex Donetska, Khersonska, Luhanska, and Zaporizka oblasts[442] and, in December 2022, the State Duma (the lower house of the Federal Assembly of Russia) adopted Bill no. 246425-8 in the first reading – a bill which proposes to remove criminal liability for crimes committed in the four oblasts before their annexation provided they were “aimed at protecting the interests of the Russian Federation” or the territories.[443] It is against this background that attacks on health care have been taking place throughout the conflict in Ukraine.
The mobilization of Russia’s armed forces: The movement of Russian armed forces was reported on or near the Ukrainian border as early as mid-October 2021.[444] On February 24, 2022,President Putin launched a coordinated, full-scale land, sea, and air invasion of Ukraine through three entry points: the north from Belarus, the south through Russian-occupied Crimea, and the east through Russia.[445] Up to 200,000 Russian troops are estimated to have been deployed in the first few days of the invasion.[446] Six months later, President Putin signed a decree increasing the size of Russia’s armed forces[447] and, shortly after, declared the partial mobilization of military reservists.[448] In December 2022, a second wave of mobilization was reported.[449]
The scale of the acts of violence: The case studies, together with the dataset, reveal the frequency and intensity with which Ukraine’s health care system has been disrupted through attacks that resulted in the damage, destruction, and looting of health care facilities and transport, as well as attacks on health care workers. As noted by the OSCE Moscow Mechanism in its Second Report covering the period between April 1 and June 25, 2022 “[t]he war has increased the demand for healthcare services while reducing the system’s ability to provide them, particularly in areas of active conflict.… These attacks against health facilities, transportation, personnel, patients, supplies, and warehouses, put healthcare workers in danger, deny patients access to desperately needed care, and damage the health system. The number is increasing.”[450] While requiring further investigation by relevant authorities to ascertain the circumstances in which attacks have occurred, including the perpetrators, this suggests that attacks on civilians and civilian objects generally, and on Ukraine’s health care system specifically, were pursued pursuant to a policy, rather than as a mere accumulation of spontaneous or isolated acts.
The repeated and coordinated military offensives: Russian forces reportedly played an active role in each of the attacks detailed in the case studies above. Military offensives on Ukraine’s health care system seem to have largely followed Russia’s invasion pattern, for example: the first attacks on ambulances in Khersonska oblast and on health care facilities in the city of Chernihiv reported in February 2022; targeted attacks on a hospital in the outskirts of Trostianets in March 2022 as Russian troops occupied the town; the capture and mistreatment of health care workers in Mariupol in March 2022 as the city was under siege; the carpet bombing of Izium resulting in severe damage to a hospital prior to the town’s occupation from April to September 2022; and the attack on an ambulance in Lyman as Russian troops entered the nearby town of Kreminna in April 2022.
The attack against the civilian population, including through the health care system, appears to have been both widespread and systematic.[451] The term “widespread” refers to the large-scale nature of the attack in that it “should be massive, frequent, carried out collectively with considerable seriousness and directed against a multiplicity of victims.”[452] The assessment is “neither exclusively quantitative nor geographical, but must be carried out on the basis of the individual facts,” meaning “a widespread attack may be the cumulative effect of a series of inhumane acts or the singular effect of an inhumane act of extraordinary magnitude.”[453] The term “systematic” refers to “the organised nature of the acts of violence and the improbability of their random occurrence.”[454] Much like the existence of a policy, the systematic nature of an attack is assessed through “patterns of crimes, in the sense of non-accidental repetition of similar criminal conduct on a regular basis.”[455]
An analysis of the “widespread” or “systematic” nature of the attack would therefore necessarily rely on much of the same factors reviewed above. The number of attacks against Ukraine’s health care system – including facilities, vehicles, and personnel – throughout several oblasts that span a broad expanse of Ukraine’s territory and the multiplicity of victims among both health care professionals and patients, as well as the associated consequences of the disruption of future care on the general population, suggest that the attack on the civilian population may be widespread in nature. It is also possibly systematic as the acts of violence appear to be neither spontaneous nor isolated. They share a number of similarities consistent with a “course of conduct”: they followed similar temporal and geographical patterns as Russia’s full-scale invasion unfolded, attacks detailed in the case studies involved the presence of mobilized Russian forces, and almost consistently resulted in severe damage to health care facilities, destruction or loss of medical equipment and vehicles, and violence against medical personnel and patients alike, including serious injury and loss of life.[456]
On the basis of the above, the information provided appears sufficient to warrant an investigation into whether Russia’s armed forces have, at a minimum, engaged in the crime against humanity of “other inhumane acts” (Article 7(1)(k)). Other inhumane acts are “serious violations of international customary law and the basic rights pertaining to human beings, drawn from the norms of international human rights law,” that cause great suffering, or serious injury to body or mental or physical health to the victims.[457]
International courts and tribunals have, in the past, made findings on crimes against humanity involving, among others, the perpetrators’ deliberate deprivation of medical care to civilians under their control.[458] These acts likely apply directly in the context of, for example, the treatment of patients and health care professionals in the Russian-controlled correctional colonies of Olenivka and Horlivka, where prisoners were routinely denied proper medical care by guards (case study #10).[459] The overall disruption and destruction of Ukraine’s health care system, as demonstrated by the case studies and the dataset, could similarly constitute a deliberate deprivation of medical care. As noted by the OSCE Moscow Mechanism, “by causing a high level of destruction and by interfering with the provision of vital services (education, healthcare), the conflict started by the unlawful attack by Russia has made it very difficult for Ukraine to effectively respect, protect and fulfil the human rights of its inhabitants.”[460] A full investigation into the context and circumstances of attacks on Ukraine’s health care system may uncover what appears to be a more generalized deprivation of access to health – of the right to health – as a method of war, carried out as a part of a deliberate effort to cause civilian mental and physical suffering.
Ukrainian Criminal Law
As noted, Ukrainian courts will serve as the primary seat to adjudicate crimes occurring on Ukrainian territory. As of January 2023, the office of the prosecutor general (OPG) of Ukraine has already registered more than 63,000 instances of alleged war crimes since the beginning of the full-scale invasion of Ukraine.[461] Relying on the standard prosecutors must satisfy when opening an investigation – circumstances “likely to indicate” that a criminal offence has been committed[462] – this section analyzes attacks on health care in Ukraine in light of relevant provisions of the CCU.[463]
Despite its broad title, the current wording of Section XX of the CCU (“criminal offenses against peace, security of mankind and international order”)[464] makes no reference to crimes against humanity and lacks specificity in its approach to the criminalization of IHL violations.[465] In order to bring Ukraine in conformity with the international legal framework on war crimes and crimes against humanity, two draft laws have been submitted to the Verkhovna Rada (Ukraine’s parliament) to date: Bill no. 2689[466] and Bill no. 7290.[467] The former includes provisions on war crimes and crimes against humanity, including on command responsibility, consistent with the Rome Statute.[468] It was adopted by the Verkhovna Rada in May 2021, but was not signed into law by the president.[469] On April 15, 2022, the cabinet of ministers registered another draft law for consideration – Bill no. 7290.[470] While this draft law has been criticized for restricting the application of command responsibility and lacking a provision instituting universal jurisdiction in Ukraine,[471] the list of criminalized acts – war crimes and crimes against humanity – is the same as that of Bill no. 2689 and would therefore constitute a step forward in the prosecution of these crimes under the CCU.
As such, Section XX of the CCU, in its current version, is the governing law in the context of domestic prosecutions of alleged war crimes, including attacks against Ukraine’s health care system by Russia’s armed forces.[472] These include, chiefly:
Violations of the Laws and Customs of War (Article 438 CCU): Article 438 of the CCU lists several relevant, conflict-related crimes; some of which are currently being investigated or have already been adjudicated since the beginning of the full-scale invasion.[473] For instance, three Russian service members – two tank commanders and one assistant – were charged in absentia for their alleged role in firing at the Trostianets City Hospital with T-80 and T-72 tanks in March 2022.[474] Article 438 CCU includes a non-exhaustive list of conduct that gives rise to criminal liability, including the “use of means of warfare prohibited by international law” and “any other violations of rules of the warfare” recognized by international treaties ratified by Ukraine. An analysis of the provision by Global Rights Compliance[475] reveals that:
While Article 438 generally criminalizes the use of means of warfare through reference to any prohibition contained in international law (thereby encompassing both international treaties and customary international law), it takes a narrower approach to the other violations of the “laws and customs of war,” in other words, violations of methods of warfare. In the case of violations of methods of warfare, only those contained in international treaties ratified by Ukraine are included, and not those that are recognized by customary international law.
A literal reading of Article 438 suggests that it is not intended to incorporate all crimes or violations of the methods of warfare that are part of customary IHL, instead limiting itself to those enumerated in the treaties ratified by Ukraine, such as the Geneva Conventions and Additional Protocols, as well as other violations enforced by other treaties ratified by Ukraine.[476]
Nonetheless, the case studies above point to the likely commission of the following crimes enumerated in the Geneva Conventions and Additional Protocol I, allowing the application of Article 438 of the CCU:
- Indiscriminate attacks resulting in loss of life or injury to civilians or damage to civilian objects;[477]
- Disproportionate attacks;[478]
- Making medical objects or personnel the objects of attack;[479]
- Pillage and extensive destruction or appropriation of property;[480]
- Using human shields;[481]
- Unlawful confinement;[482]
- Willful killing;[483] and
- Torture or inhuman treatment.[484]
These IHL violations overlap, in broad terms, with war crimes under the Rome Statute examined above.[485] As such, the case studies and their analysis under the Rome Statute discussed above fall under the respective categories of IHL violations, as transposed into Ukrainian criminal law by Article 438 CCU.
Ordinary crimes under Ukrainian law: There are no legal barriers to prosecuting the alleged crimes outlined in the report as ordinary crimes under Ukrainian law, such as crimes against property,[486] crimes against the life and health of persons,[487] and crimes against the liberty, honor, and dignity of persons.[488] However, prosecutions under Article 438 of the CCU should be prioritized – whenever possible – to appropriately capture the specific and international character of the offences. Given the international character of the armed conflict, the categories of ordinary crimes listed above fall under the scope of Article 438 CCU when committed within context of the armed conflict and should thus be prosecuted accordingly.
Universal jurisdiction allows third countries to prosecute serious crimes under international law – such as war crimes and crimes against humanity – regardless of where they were committed or of the nationality of the perpetrators and the victims.[489] It was first codified in the Geneva Conventions,[490] expanded in Additional Protocol I,[491] and further reinforced in other international conventions.[492] An increasing number of countries worldwide and member states of the ICC recognize the principle of universal jurisdiction[493] in an effort to manifest solidarity with the victims and survivors of such crimes.[494]
These countries have adopted domestic legislation to incorporate the crimes listed in the international conventions they ratified, such as the Geneva Conventions,[495] the Convention against Torture,[496] and the Rome Statute.[497]
As of October 2022, at least 12 third countries had opened investigations into alleged war crimes and crimes against humanity committed in Ukraine since the beginning of the full-scale invasion.[498] Considering the thousands of instances of war crimes registered by the OPG since the beginning of the full-scale invasion, the gaps in Ukrainian law concerning crimes against humanity, the absence of certain war crimes contained in the Geneva Conventions from the Rome Statute, and the finite resources Ukrainian courts and the ICC have, the exercise of universal jurisdiction can be a powerful tool to ensure that serious crimes committed in Ukraine do not remain unpunished.
In the context of Ukraine, most of the obstacles that usually present a challenge in the exercise of universal jurisdiction – such as access to the victims, witnesses, and crime sites or the lack of political will to pursue cases against citizens of foreign countries – are easily surmountable.[499]
Conclusion and Recommendations
The case studies and dataset highlighted in this report describe the staggering toll that Russia’s war of aggression has had on Ukraine’s health care system. From repeated attacks on health care facilities and ambulances, theft and destruction of critical infrastructure and supplies, and evidence of assaults and ill-treatment of Ukrainian health workers, the devastation wrought since Russia’s full-scale invasion is clear. The true scale and impact that it is having on access to health care – and on the right to health of Ukraine’s people – will not be known for years to come.
Protecting health care, including access to and delivery of health care services, is a shared responsibility of all parties to an armed conflict. This duty extends to Russia and Ukraine equally under international humanitarian law (IHL).
Beyond protection, however, there is a pressing need to ensure accountability. For too long, violations of IHL with respect to health care have been ignored by the international community.[500] It was not until 2016, following building momentum, that the United Nations Security Council finally achieved a political breakthrough: it adopted Resolution 2286, which condemns attacks against health and commits to their prevention and to holding perpetrators to account domestically and internationally. Despite this, hospital attacks and other crimes against health care have only rarely been prosecuted.[501]
This report is a call to investigators and prosecutors – in Ukraine, at the International Criminal Court, and in third states that may also have jurisdiction – to prioritize prosecution for such attacks and affirm that the laws protecting medical facilities and personnel be respected and enforced.
Based on the evidence presented here, there is a reasonable basis to believe that attacks on Ukraine’s health care system constitute war crimes and comprise a course of conduct that could potentially constitute crimes against humanity as well. At a minimum, this evidence warrants immediate investigation by prosecutorial authorities.
The Russian Federation’s continued aggression – leading to both targeted and indiscriminate attacks on Ukraine’s health care facilities, amongst other civilian infrastructure – constitutes a gross violation of international law. It must cease these attacks and end its aggression. Russia is also obligated to make reparations for its breaches of international law, including compensating the Ukrainian state and individual Ukrainians – and other killed or injured nationals – for devastating loss of life and injury, extensive destruction, and the enormous costs of reconstruction resulting from its attacks on the health care system.
To other engaged actors, the report makes the following recommendations:
To the International Criminal Court’s Office of the Prosecutor, the Prosecutor General of Ukraine, the Independent International Commission of Inquiry on Ukraine, and other National Prosecutors:
- Prioritize investigation of attacks on health care facilities and health care workers as both war crimes and crimes against humanity.
- Build cases specifically focused on crimes concerning attacks on Ukraine’s health care facilities and health care personnel, ensuring adequate resource allocation and training to do so effectively.
- Ensure continued strong cooperation and coordination among prosecutorial offices and bodies at the national and international level, in order to maximize information sharing and efficiency.
To the Diplomatic Community, including Member States of the European Union, the United Nations (UN) Security Council, and the Organization for Security and Co-operation in Europe:
- Publicly condemn attacks on health care personnel and facilities in Ukraine, and urge compliance with the Geneva Conventions, Additional Protocol I, and UN Security Council Resolution 2286, including rules on medical impartiality.
- Continue to exert all available political, economic, and diplomatic pressure on the Russian Federation to immediately cease both indiscriminate and targeted attacks on civilians and civilian infrastructure, including on health care workers, facilities, and vehicles, as well as to withdraw from Ukrainian territory.
- Call for the immediate release of detained health care professionals and the humane treatment of all detainees in compliance with international humanitarian law.
- Convene an Arria-Formula Meeting of the UN Security Council to address widespread and systematic attacks on Ukraine’s health care system and reinforce the need to ensure criminal accountability.
- Commit adequate and long-term funding and other resources to justice and accountability mechanisms working to document international crimes and other gross human rights violations in Ukraine, including violations of the right to receive and access health care.
- Support and cooperate with international and Ukrainian non-governmental organizations (NGOs) to assist in gathering, coordinating, and disseminating data on attacks on health care.
To the Government of Ukraine:
- Ratify the Rome Statute of the International Criminal Court.
- Adopt domestic implementing legislation that sufficiently captures the substantive crimes and modes of liability provided for under the Rome Statute, including crimes against humanity and command responsibility, as well as other relevant offenses under international humanitarian law.
To the UN Human Rights Council and its Member States:
- Renew the mandate of the UN Independent International Commission of Inquiry on Ukraine on an open-ended basis and ensure robust funding and support for its continued functioning.
- Convene a thematic debate to address widespread and systematic attacks on Ukraine’s health care system and the need to ensure criminal accountability.
- Consider expanding the mandate of the inaugural Special Rapporteur on the “Situation of Human Rights in the Russian Federation” to encompass violations related to the 2022 full-scale invasion, including the rights of Ukrainian civilians currently being held on Russian territory.
To the UN Secretary-General:
- Promote further coordination and cooperation among the Secretary-General’s Office and with other relevant UN agencies, investigative mechanisms, and non-governmental organizations (NGOs) to share their methods, data, reporting capacities, and roles on attacks on health care.
- Appoint a Special Representative on Violence Against Health Care to address attacks on Ukraine’s health care system and in other conflicts.
To the World Health Organization (WHO) and its Member States:
- Proactively work with NGOs and UN agencies to expand data collection and, where appropriate, public disclosure in Ukraine and elsewhere.
- Adopt a resolution by the World Health Assembly to address ongoing concerns in structure, oversight, and operation of the Surveillance System for Attacks on Health Care, including a review of WHO’s Framework of Engagement with Non-State Actors that would allow for mutual data sharing with UN agencies and NGOs, in both Ukraine and other countries.
- Acting under Article 7 of the WHO Constitution, suspend voting rights of the Russian Federation and remove representatives of the Russian Federation from executive positions.
Acknowledgements
This report is a joint product of eyeWitness to Atrocities (eyeWitness), Insecurity Insight, the Media Initiative for Human Rights (MIHR), Physicians for Human Rights (PHR), and the Ukrainian Healthcare Center (UHC).
The report was researched and written by Christian De Vos, MSc, JD, PhD, PHR director of research and investigations; Anna Gallina, LLM, advanced LLM, eyeWitness associate legal advisor; Pavlo Kovtoniuk, MPh, UHC co-founder; the MIHR team; Uliana Poltavets, MSc, PHR Ukraine emergency response coordinator; Julianne Romy, MA, MA, LLM, eyeWitness legal advisor; Diana Rusnak, MPh, UHC research analyst; and Christina Wille, MPhil, Insecurity Insight director. Will Jaffe, PHR research fellow, also contributed to the drafting of the report.
The report was reviewed by eyeWitness staff members Wendy Betts, MA, JD, director, and Alla Malomuzh, LLM, PhD, legal specialist (Ukraine); the MIHR team; and PHR staff members Erika Dailey, MPhil, director of advocacy and policy; Michele Heisler, MD, MPA, medical director; Karen Naimer, MA, JD, LLM, director of programs; Catherine Pilishvili, international advocacy officer; Kevin Short, deputy director, media and communications; and Gerson Smoger, JD, PhD, interim executive director.
Interviewing, data collection, and verification was carried out by UHC staff members Tetiana Korchak, LLM, lawyer; Mariia Kravchenko, head of communication projects; Volodymyr Lotushko, MSc, MD, research analyst; Mariia Lypovchenko, project manager; and Olena Sinitsyna, MPh, consultant. Interviews were also conducted by the MIHR team.
Insecurity Insight’s team of 10 people delivered the large-scale exercise in open-source monitoring and data processing required for this study. Insecurity Insight jointly developed the interactive map with DrivenData and was responsible for data analysis and editorial comments on the report. The report was further supported by data from the International NGO Safety Organisations’ (INSO) Conflict and Humanitarian Data Centre (CHDC).
The report received external review from Leonard S. Rubenstein, JD, LLM, professor of the practice at Johns Hopkins Bloomberg School of Public Health and chair of the Safeguarding Health in Conflict Coalition, who provided invaluable advice and support. In addition, we gratefully acknowledge the assistance of the following staff members of Global Rights Compliance, all of whom are also members of the mobile justice team supporting the Office of the Prosecutor General of Ukraine: Julian Elderfield, LLM, international legal advisor; Wayne Jordash, QC, managing partner; and Anna Mykytenko, LLM, senior legal adviser. Our organizations also acknowledge the assistance of a weapons analyst with years of experience working in support of international criminal investigations and as NATO weapons inspector, with whom we consulted. The expert’s comments provided invaluable detail to the report’s case studies and are referenced accordingly in the report.
The report was reviewed, edited, and prepared for publication by PHR’s senior publications consultant, with assistance from Samantha Peck, PHR program and executive associate.
PHR research and investigations interns Erica Berry and Kseniia Michkodan also supported the project.
Endnotes
[1] “Ukraine War: Hospital destroyed by Russian missile in southern Ukraine,” Sky News, April 22, 2022, https://www.youtube.com/watch?v=ff1eF2JSfnE.
[2] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[3] “Ukraine War: Hospital destroyed by Russian missile in southern Ukraine,” Sky News, April 22, 2022, https://www.youtube.com/watch?v=ff1eF2JSfnE.
[4] For an in-depth analysis of Russia’s involvement in Crimea and Donbas between December 2013 and February 13, 2022, see Global Rights Compliance, “International Law and Defining Russia’s Involvement in Crimea and Donbas,” February 13, 2022, https://globalrightscompliance.com/wp-content/uploads/2022/05/International-Law-and-Russia-Involvement-in-Crimea-and-Donbas-1.pdf. See also Marieke de Hoon, “Dutch Court, in Life Sentences: Russia Had ‘Overall Control of Forces in Eastern Ukraine Downing of Flight MH17,” JustSecurity.org, December 19, 2002, https://www.justsecurity.org/84456/dutch-court-in-life-sentences-russia-had-overall-control-of-forces-in-eastern-ukraine-downing-of-flight-mh17/; Ukraine and the Netherlands v. Russia, No. 8019/16, 43800/14, 28525/20, ECHR (Grand Chamber), January 25, 2023 (finding that Russia exercised “effective control” on account of its military presence in eastern Ukraine and the decisive degree of influence it enjoyed over these areas as a result of its military, political and economic support to the “DPR” and the “LPR”).
[5] See Cynthia J. Buckley, Ralph S. Clem, and Erik Herron, “Attacks on Healthcare Infrastructure in the Donbas: Implications for Ukrainian State Legitimacy,” PONARS Eurasia (January 11, 2019), https://www.ponarseurasia.org/attacks-on-healthcare-infrastructure-in-the-donbas-implications-for-ukrainian-state-legitimacy/.
[6] Because Insecurity Insight does not a have a specific mandate for or expertise in criminal accountability, it did not contribute to – and does not take a view on – the portion of the report that legally analyzes alleged IHL violations under international criminal law and Ukrainian domestic law.
[7] World Health Organization, “Accessing health care in Ukraine after 8 months of war: The health system remains resilient, but key health services and medicine are increasingly unaffordable,” October 24, 2022, https://www.who.int/europe/news/item/24-10-2022-accessing-health-care-in-ukraine-after-8-months-of-war–the-health-system-remains-resilient–but-key-health-services-and-medicine-are-increasingly-unaffordable.
[8] United Nations Human Rights – Office of the High Commissioner, “Update on the Human Rights Situation in Ukraine”, August 1 – October 31, 2022, p. 2, https://www.ohchr.org/en/documents/country-reports/hrmmu-update-human-rights-situation-ukraine-1-august-31-october-2022.
[9] As detailed further below, this map includes incidents between February 24 and December 31, 2022; however, it will also serve as an ongoing record of documented attacks, beyond the time period this report covers. See www.attacksonhealthukraine.org.
[10] See, e.g., “Ukraine: Ukrainian fighting tactics endanger civilians,” Amnesty International, August 4, 2022, https://www.amnesty.org/en/latest/news/2022/08/ukraine-ukrainian-fighting-tactics-endanger-civilians/; Human Rights Watch, “Russian, Ukrainian Bases Endangering Civilians: Basing Forces in Populated Areas Creates Unnecessary Risk,” Human Rights Watch, July 21, 2022, https://www.hrw.org/news/2022/07/21/russian-ukrainian-bases-endangering-civilians; “Ukraine: Banned Landmines Harm Civilians” Human Rights Watch, January 31, 2023, https://www.hrw.org/news/2023/01/31/ukraine-banned-landmines-harm-civilians. For a helpful corrective to Amnesty’s claims, see Michael N. Schmitt, “Ukraine Symposium – Amnesty International’s Allegations of Ukrainian IHL Violations,” August 8, 2022, https://lieber.westpoint.edu/amnesty-allegations-ukrainian-ihl-violations/.
[11] In Case Study #2 detailed herein (Makariv Multiprofile Intensive Care Hospital and Makariv Primary Care Clinic), there is evidence that Ukraine’s armed forces reportedly established a base at the hospital as of March 7, 2022, thus depriving it of its protected status under IHL; however, this was after all remaining patients and doctors had been evacuated from the facility.
[12] A note on spelling: in accordance with the 10th United Nations Conference on the Standardization of Geographical Names this report uses the “Romanization system” as the international system for the transliteration of Ukrainian geographical names. See, e.g., https://mfa.gov.ua/storage/app/sites/1/e-conf101-84-roman-system-ukraine-eng.pdf.
[13] PHR’s Ethics Review Board provided guidance and approved this study based on regulations outlined in Title 45 CFR Part 46, which are used by academic Institutional Review Boards in the United States. All of PHR’s research and investigations involving human subjects are conducted in accordance with the Declaration of Helsinki 2000, a statement of ethical principles for medical research involving human subjects, including research on identifiable human material and data.
[14] See “Timeline of Attacks on Health Care in Ukraine,” https://insecurityinsight.org/country-pages/ukraine.
[15] For more information on the Insecurity Insight’s SIND database used for the Safeguarding Health in Conflict Coalition see SHCC methodology, https://shcc.pub/2021Methodology.
[16] See The Humanitarian Data Exchange, “Ukraine: Attacks on Aid Operations, Education, Health and Conflict-related Sexual Violence (CRSV),” https://data.humdata.org/dataset/ukraine-data-on-attacks-on-aid-operations-education-health-and-protection.
[17] See https://humanrights.berkeley.edu/berkeley-protocol-digital-open-source-investigations. If UHC obtained only one type of evidence to confirm an incident, it was coded as a first level verification; if UHC obtained two or more types of evidence, an incident received a higher, second level verification.
[18] Sources’ reliability was based on four principal criteria: their credibility, based on the online presence and posting history of sources; independence and impartiality; specificity, i.e., the extent to which a source can reveal more details of the occurrence; and attenuation. For the latter, reports and text drafted contemporaneously with the events that they reference tend to be viewed as more reliable than those produced after the events have occurred.
[19] The data is stored in a secure online database that follows Insecurity Insight’s standard event-based coding and data protection procedures.
[20] Digital forensic examination was excluded from the verification protocol as that is not within any of the research partners’ capacities.
[21] See https://www.who.int/activities/stopping-attacks-on-health-care. Examples of types of attacks on health can include: violence with individual weapons or heavy weapons, psychological violence/threat of violence/intimidation, obstruction to delivery of care, assault without weapons, sexual assault, denial of access to services, armed or violent search of health resources, removal of health care assets, setting fire to health resources, and militarization of health care facilities. Notably, incidents were only included that could be considered directly relevant to the Russia-Ukraine War because the violence was perpetrated by conflict actors; violence by private individuals (e.g., patients) is not included. The database also does not include counts of the reported deaths of patients as the impact of attacks on patients is much wider in ways that are not possible to capture through incident-based monitoring. For more information on methodologies to document the impact of attacks on health care for patients, see https://riah.manchester.ac.uk/.
[22] The app is designed so that neither the footage nor its associated metadata can be tampered with by the user or third parties. In conjunction with transmission protocols, eyeWitness’ server creates a chain of custody with embedded information for the footage from the point of capture to its receipt by the server. eyeWitness seeks consent before sharing footage captured by non-anonymous users with third parties. Users provided consent to share the photos they captured with the app and uploaded to eyeWitness’ server for the purpose of this report and associated map. For more information about the App and resources, see eyeWitness to Atrocities, “Resources,” accessed February 3, 2023, https://www.eyewitness.global/resources.
[23] See Rohini Haar and Susannah Sirkin, “Strengthening Data to Protect Healthcare in Conflict Zones,” International Peace Institute, November 2022, https://www.ipinst.org/2022/11/strengthening-data-to-protect-healthcare-in-conflict-zones.
[24] Notably, previous work has shown that there was “minimal overlap” between Insecurity Insight’s database and the WHO’s, suggesting “significant underreporting of attacks on health care.” For similar reasons, the number of reported incidents in Ukraine is likely an undercount as well. See Vanessa Parada, Larissa Fast, Carolyn Briody, Christia Wille and Rudi Coninx, “Underestimating attacks: Comparing two sources of publicly available data about attacks on health care in 2017,” Conflict and Health 17 (2023), https://conflictandhealth.biomedcentral.com/articles/10.1186/s13031-023-00498-w.
[25] WHO definition of “health care infrastructure”: “Any infrastructure necessary to provide health care, including but not limited to laboratories, pharmacies, medical warehouses, ambulances, ambulance stations and/or garages, administrative buildings used to administer health care and to provide medical education, or any other health care facility not named here.”
[26] Across all of Ukraine there are approximately 2,500 hospitals (https://reliefweb.int/report/ukraine/attacks-ukraine-s-hospitals-will-cause-long-term-harm-health ), of which some 300 are in zones of active fighting while some 1,000 are in areas that have seen changes in territorial control. (WHO Ukraine crisis strategic response plan for June December, July 2022) With 218 hospitals reported damaged or destroyed, nearly nine percent of the country’s hospitals have been directly affected by conflict damage.
[27] “Area-based assessment in conflict-affected area of Ukraine – Briefing note: Basic service provision for women and children in Kharkiv city, Ukraine (November 2022),” Reach, November 2022, https://reliefweb.int/report/ukraine/area-based-assessment-conflict-affected-area-ukraine-briefing-note-basic-service-provision-women-and-children-kharkiv-city-ukraine-november-2022.
[28] “War in Ukraine: situation report from WHO Ukraine country office. Issue No. 31, 9 October 2022,” WHO Ukraine country office, No. 31, October 9, 2022, https://reliefweb.int/report/ukraine/war-ukraine-situation-report-who-ukraine-country-office-issue-no-31-9-october-2022.
[29] “Priorities for health system recovery in Ukraine – joint discussion paper,” Ukraine, WHO Health Emergencies Programme, December 28, 2022, https://www.who.int/europe/publications/m/item/priorities-for-health-system-recovery-in-ukraine-joint-discussion-paper.
[30] This does not mean that explosive weapons were only used in 89 percent of cases, but rather that those who provided the event description mentioned a specific weapon category. The absence of information on specific weapons system is likely more due to lack of knowledge and awareness by the event describer than whether a weapons system was actually engaged.
[31] “Putin Admits Attacks on Ukraine Infrastructure, Asking, ‘Who Started It?,’” Washington Post, December 8, 2022, https://www.washingtonpost.com/world/2022/12/08/russia-attacks-ukraine-infrastructure-putin/.
[32] Correspondence with weapons analyst (on file).
[33] See “Endless Brutality: War Crimes in Chechnya,” Physicians for Human Rights, May 2001, https://phr.org/wp-content/uploads/2001/05/chechnya-endless-brutality-report2001.pdf.
[34] Peter Moszynski, “Health facilities in Georgia have been attacked,” BMJ, August 19, 2008 (Vol. 337), https://www.bmj.com/content/337/bmj.a1357.
[35] “Medical Personnel Are Targeted in Syria,” Physicians for Human Rights (accessed January 6, 2023), https://phr.org/our-work/resources/medical-personnel-are-targeted-in-syria/.
[36] Dr. Houssam al-Nahhas, “As Putin bombs hospitals in Ukraine, I hear echoes from Syria,” The New Humanitarian, April 13, 2022, https://www.thenewhumanitarian.org/opinion/first-person/2022/04/13/putin-bombs-hospitals-ukraine-i-hear-echoes-syria; see also Annie Sparrow, “Russia is waging war on Ukrainian healthcare,” Financial Times, July 5, 2022, https://www.ft.com/content/87c0e3c4-8e4b-4c85-b5b3-ef5c180369e3.
[37] “Anatomy of a Crisis: A Map of Attacks on Health Care in Syria,” Physicians for Human Rights, December 2017, https://s3.amazonaws.com/PHR_syria_map/findings.pdf.
[38] Organization for Security and Co-operation in Europe, “Report of the Human Rights Assessment Mission on Crimea (6-18 July 2015),” September 17, 2015, paras. 43, 204-13, https://www.osce.org/files/f/documents/0/2/180596.pdf.
[39] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 72, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[40] Cynthia J. Buckley, Ralph S. Clem and Erik Herron, “Attacks on Healthcare Infrastructure in the Donbas: Implications for Ukrainian State Legitimacy,” PONARS Eurasia (January 11, 2019), https://www.ponarseurasia.org/attacks-on-healthcare-infrastructure-in-the-donbas-implications-for-ukrainian-state-legitimacy/.
[41] Cynthia J. Buckley, Ralph S. Clem and Erik Herron, “Attacks on Healthcare Infrastructure in the Donbas: Implications for Ukrainian State Legitimacy,” PONARS Eurasia (January 11, 2019), https://www.ponarseurasia.org/attacks-on-healthcare-infrastructure-in-the-donbas-implications-for-ukrainian-state-legitimacy/.
[42] “Impunity Must End: Attacks on Health in 23 Countries in Conflict in 2016,” Safeguarding Health in Conflict Coalition, 2017, p. 11, https://www.safeguardinghealth.org/sites/shcc/files/SHCC2017final.pdf.
[43] Events 35991, 35723, 35826. According to reports from Ukrainian military intelligence,patients from the regional tuberculosis hospital in Vovchansk (Kharkivska oblast) have been turned out and buildings have instead been filled with wounded Russian soldiers, with the medical personnel forced to care for them (https://t.me/DIUkraine/433). Ukrainian medical personnel from the Central District Hospital in Polohy (Zaporizka oblast) have been prevented from treating civilians while Russian forces instead use the hospital premises as a warehouse for ammunition (https://t.me/DIUkraine/433). According to the Luhansk Regional Military Administration, at least three hospitals in Luhanska oblast are being used to treat Russian soldiers (https://t.me/luhanskaVTSA/7961). Media reports suggest the civilian population in Mariupol is being denied care. https://suspilne.media/355930-v-mariupoli-zrosla-zahvoruvanist-likarni-perepovneni-andrusenko/.
[44] Public Health Center of the Ministry of Health of Ukraine, https://apps.who.int/iris/bitstream/handle/10665/365564/WHO-EURO-2023-6904-46670-67870-eng.pdf?sequence=1&isAllowed=y.
[45] See “Catch-up polio immunization campaign to begin in Ukraine,” WHO Europe, January 27, 2002, https://www.who.int/europe/news/item/27-01-2022-catch-up-polio-immunization-campaign-to-begin-in-ukraine.
[46] Analysis conducted by UHC (on-file).
[47] “Health needs assessment of the adult population in Ukraine: Survey report,” World Health Organization – European region, September 2022, p. 20, https://apps.who.int/iris/bitstream/handle/10665/365564/WHO-EURO-2023-6904-46670-67870-eng.pdf?sequence=1&isAllowed=y.
[48] “Ukraine Internal Displacement Report—General Population Survey Round 11,” International Organization for Migration (25 November-5 December 2022), p. 11, https://dtm.iom.int/reports/ukraine-internal-displacement-report-general-population-survey-round-11-25-november-5.
[49] Oleksii Sukhovii, Olga Khan, Olena Doroshenko, and Vrishali Shekhar, “The Cost of Mental Health in Ukraine: The Review of Privately and Publicly Procured Medicines and Dietary Supplements (2015-2019),” World Bank (2022), https://openknowledge.worldbank.org/handle/10986/38122.
[50] “Ukraine’s mental health crisis could impact generations to come. Here’s how the country is responding,” World Economic Forum, October 9, 2022, https://www.weforum.org/agenda/2022/10/ukraine-mental-health-crisis-world-mental-health-day/.
[51] Yurii Korogodskyi, “The number of veterans may increase to 5 million people,” May 8, 2022, https://lb.ua/society/2022/05/08/516086_kilkist_veteraniv_mozhe.html.
[52] See for instance Lorenzo Tondo, “‘Very similar’: fears gateway city to Donbas will become another Bucha,” The Guardian, April 18, 2022, https://www.theguardian.com/world/2022/apr/18/bucha-izyum-fears-gateway-city-donbas-russia-ukraine; Thomas Gibbons-Neff and Marc Santora, “Ukrainian Offensive Seen as Reshaping the War’s Contours,” The New York Times, September 10, 2022, https://www.nytimes.com/2022/09/10/world/europe/ukraine-offensive-izium-donbas.html.
[53] Pavlo Bakhura, “No safe way out of Izyum: ‘I Can’t Imagine How it Will End’,” The Guardian, April 4, 2022, https://www.theguardian.com/world/2022/apr/04/izyum-ukraine-shelling-russian-soldiers; Maksym Strelnyk, Facebook, March 8, 2022, https://www.facebook.com/max.strel.9/posts/1712768382263714.
[54] Pavlo Bakhura, “No safe way out of Izyum: ‘I can’t imagine how it will end’,” The Guardian, April 4, 2022.
[55] Thomas Gibbons-Neff and Marc Santora, “Ukrainian Offensive Seen as Reshaping the War’s Contours,” The New York Times, September 10, 2022, https://www.nytimes.com/2022/09/10/world/europe/ukraine-offensive-izium-donbas.html; “Izium and Balakliia after liberation from Russian occupation – in pictures,” The Guardian, September 21, 2022, https://www.theguardian.com/world/gallery/2022/sep/21/ukraine-izium-and-balakliia-after-liberation-from-russian-occupation-in-pictures.
[56] Dan Bilefsky and Edward Wong, “Izium Discoveries Renew Focus on Holding Russia Accountable for Civilian Toll,” New York Times, September 17, 2022, https://www.nytimes.com/2022/09/17/world/europe/izium-graves-russia-war-crimes.html. See also Pavlo Bakhura, “No safe way out of Izyum: ‘I can’t imagine how it will end’,” The Guardian, April 4, 2022, https://www.theguardian.com/world/2022/apr/04/izyum-ukraine-shelling-russian-soldiers.
[57] Sasha Solovei, “History of the Pishchanska Bohomatir Izium Central City Hospital,” Izium Informatsiinyi, December 27, 2022, https://city-izyum.pp.ua/history-of-the-izyum-central-city-hos/.
[58] Sasha Solovei, “History of the Pishchanska Bohomatir Izium Central City Hospital,” Izium Informatsiinyi, December 27, 2022, https://city-izyum.pp.ua/history-of-the-izyum-central-city-hos/.
[59] Sasha Solovei, “History of the Pishchanska Bohomatir Izium Central City Hospital,” Izium Informatsiinyi, December 27, 2022, https://city-izyum.pp.ua/history-of-the-izyum-central-city-hos/.
[60] “The Emergency Department is Being Renovated at the Izium Central City Hospital,” Kharkiv Region Military Administration, February 11, 2021, https://kharkivoda.gov.ua/news/107072; “New CT scanner delivered to Izyum Central City Hospital,” Izium Informatsiiny, April 4, 2021, https://city-izyum.pp.ua/a-new-computed-tomograph-was-brought-to-the-izyum-central-city-hospital101/.
[61] Office of the Prosecutor General, Telegram, March 3, 2022, https://t.me/pgo_gov_ua/3025.
[62] Suspilne Kharkiv, Telegram, March 2, 2022, https://t.me/suspilnekharkiv/8594; Suspilne Kharkiv, Telegram, March 2, 2022, https://t.me/suspilnekharkiv/8597; Verkhovna Rada of Ukraine – Ukrainian Parliament, Twitter, March 3, 2022, https://twitter.com/ua_parliament/status/1499184974213357571?lang=en.
[63] “Number of Victims from Airstrike in Izyum Increases: Serious Damage in the City,” Pravda,March 3, 2022, https://www.pravda.com.ua/eng/news/2022/03/3/7327625/.
[64] Suspilne News, Twitter, March 3, 2022, https://twitter.com/suspilne_news/status/1499279121410662406.
[65] “Number of Victims from Airstrike in Izyum Increases: Serious Damage in the City,” Pravda,March 3, 2022, https://www.pravda.com.ua/eng/news/2022/03/3/7327625/; “Russia Launches an Airstrike on Izium at Night, Children among the Dead,” Rubryka, March 3, 2022, https://rubryka.com/en/2022/03/03/rosiya-vnochi-nanesla-aviaudar-po-izyumu-sered-zagyblyh-dity/. The police department caught fire, a school was damaged, and the city council’s windows were shattered. See Office of the Prosecutor General, Telegram, March 3, 2022, https://t.me/pgo_gov_ua/3025; Suspilne Kharkiv, Telegram, March 3, 2022, https://t.me/suspilnekharkiv/8608; Suspilne News, “Aerial Bombardment of Izyum in the Kharkiv Region: The Prosecutor’s Office has Started Criminal Proceedings, March 4, 2022, https://suspilne.media/213576-izum-m/.
[66] Interview with Dr. Bohdan Berezhnyi, UHC, November 18, 2022 (on-file).
[67] Suspilne Kharkiv, Telegram, March 6, 2022, https://t.me/suspilnekharkiv/8860. Lester W Grau and Charles K Bartles, “Getting to Know the Russian Battalion Tactical Group,” RUSI,April 14, 2022, https://rusi.org/explore-our-research/publications/commentary/getting-know-russian-battalion-tactical-group: A battalion tactical group is a “semi-permanent task force … capable of conducting deep raids, envelopment and flanking manoeuvres.” According to Nicolas J. Fiore, a captain in the US Army, “[w]hen possible, the BTG commander will employ his strike assets to cause casualties to pressure his opponent to negotiate a settlement … To preserve combat power, BTGs employ a force of local paramilitary units as proxy forces to secure terrain and guard the BTG from direct and indirect attack.” CPT Nicolas J. Fiore, “Defeating the Russian Battalion Tactical Group,” U.S. Army Fort Benning and the Maneuver Center of Excellence,2017, https://www.benning.army.mil/armor/earmor/content/issues/2017/spring/2Fiore17.pdf.
[68] Suspilne Kharkiv, Telegram, March 7, 2022, https://t.me/suspilnekharkiv/9019.
[69] Interview with Dr. Bohdan Berezhnyi, UHC, November 18, 2022 (on-file).
[70] Suspilne Kharkiv, Telegram, March 7, 2022, https://t.me/suspilnekharkiv/8944.
[71] Suspilne Kharkiv, Telegram, March 8, 2022, https://t.me/suspilnekharkiv/9030.
[72] Suspilne Kharkiv, Telegram, March 8, 2022, https://t.me/suspilnekharkiv/9077; Maksym Strelnyk, Facebook, March 8, 2022, https://www.facebook.com/max.strel.9/posts/1712768382263714.
[73] Information provided by weapons analyst (on-file).
[74] Interview with Dr. Bohdan Berezhnyi, UHC, November 18, 2022 (on-file).
[75] Interview with Dr. Bohdan Berezhnyi, UHC, November 18, 2022 (on-file).
[76] Volodymyr Matsokin, Facebook, March 8, 2022, https://www.facebook.com/volodymyr.matsokin/posts/7675042065901336. See also Suspilne Kharkiv, Telegram, March 8, https://t.me/suspilnekharkiv/9057; Russian Troops Destroy Central Hospital in Izyum, Kharkiv Oblast,” Kyiv Independent, March 8, 2022; https://kyivindependent.com/uncategorized/russian-troops-destroy-central-hospital-in-izyum-kharkiv-oblast.
[77] See Jim Reed, “Ukraine War: WHO says Attacks on Health Facilities are Rising Daily,” BBC News, March 26, 2022, https://www.bbc.co.uk/news/health-60866669.
[78] Interview with Dr. Berezhnyi, UHC, November 18, 2022 (on-file).
[79] Suspilne Kharkiv, Telegram, March 8, 2022, https://t.me/suspilnekharkiv/9076.
[80] Volodymyr Matsokin, Facebook, March 8, 2022, https://www.facebook.com/volodymyr.matsokin/posts/7675042065901336.
[81] Interview with Dr. Berezhnyi, UHC, November 18, 2022 (on-file). The dates mentioned by Dr. Berezhnyi in his interview with UHC do not always appear to be fully accurate. They were compared with other evidence collected by UHC during their site visit and open-source information.
[82] See e.g. Suspilne Kharkiv, Telegram, March 9, 2022, https://t.me/suspilnekharkiv/9135; Suspilne Kharkiv, Telegram, March 10, 2022, https://t.me/suspilnekharkiv/9216; Suspilne Kharkiv, Telegram, March 11, 2022, https://t.me/suspilnekharkiv/9259.
[83] Interview with Dr. Berezhnyi, UHC, November 18, 2022 (on-file).
[84] “Ukraine: Beleaguered town of Izium at breaking point after constant attack from Russian forces – new testimony,” Amnesty International, March 16, 2022, https://www.amnesty.org/en/latest/news/2022/03/ukraine-beleaguered-town-of-izium-at-breaking-point-after-constant-attack-from-russian-forces-new-testimony/.
[85] Centre for Information resilience, Twitter, March 25, 2022, https://twitter.com/Cen4infoRes/status/1507382359867465731/photo/1.
[86] Information provided by weapons analyst (on-file).
[87] Information provided by weapons analyst (on-file).
[88] “Ukraine: Banned Landmines Harm Civilians” Human Rights Watch, January 31, 2023, https://www.hrw.org/news/2023/01/31/ukraine-banned-landmines-harm-civilians. See also Truth Hounds, “On the use of anti-personnel mines,” February 2, 2023, https://truth-hounds.org/en/shchodo-vykorystanna-protypikhotnykh-min/.
[89] “Ukraine: Banned Landmines Harm Civilians” Human Rights Watch, January 31, 2023, https://www.hrw.org/news/2023/01/31/ukraine-banned-landmines-harm-civilians.
[90] Oleg Synyehubov, Facebook, December 15, 2022, https://www.facebook.com/synegubov.official/posts/pfbid0323NXrmX45AfY6rkCdWeT7nA6JRnGgQ5TgaexR8QHJhF95hbA8mG5gvcbo23FFpZ7l.
[91] Head of the Makariv City Council Vadym Tokar, “Let’s Rebuild Together!,” accessed January 25, 2023, https://new.makariv-rada.gov.ua/help/. From 15,000 residents living in the town, less than 1,000 left during the active phase of the Russian offensive. See “In Makariv near Kyiv, the occupiers shot 132 people – the village head,” New Voice of Ukraine, April 8, 2022, https://nv.ua/ukr/kyiv/makariv-rosiyski-okupanti-vbili-132-miscevih-zhitelya-novini-kiyeva-50232318.html.
[92] See Frederick W. Kagan et al., “Russian Offensive Campaign Assessment, March 1,” Institute for the Study of War,March 1, 2022, https://www.understandingwar.org/backgrounder/russian-offensive-campaign-assessment-march-1: “Social media users report Russian tanks present in Makariv, a town on that ring road approximately 30 miles west of the center of Kyiv. The presence of Russian mechanized forces at Makariv suggests that the Russians intend to conduct a relatively deep envelopment of Kyiv, possibly following roads south as far as Fastiv before turning east, although they could choose avenues of approach to the capital further east.” See also Igor Girkin, March 1, 2022, Twitter, https://twitter.com/GirkinGirkin/status/1498664725978173446 (showing tanks reportedly driving through Makariv on February 28, 2022).
[93] Police of the Kyiv Region, Facebook, March 12, 2022, https://www.facebook.com/pol.kyivregion/posts/333708318793491.
[94] “Air strike in Makariv, Kyiv region: 13 people were killed,” Radio Svoboda, March 7, 2022, https://www.radiosvoboda.org/a/news-aviaudar-makariv/31741485.html. Reports by local authorities also emerged suggesting that at least 132 civilians were shot by Russian troops. Evgenia Lutsenko, “132 shot dead civilians were found in Makarov, Kyiv region, the village head,” Hromadske, April 8, 2022, https://hromadske.ua/posts/u-makarovi-na-kiyivshini-znajshli-132-rozstrilyanih-civilnih-selishnij-golova.
[95] “Communal Non-Profit Enterprise ‘Makariv Multiprofile Intensive Care Hospital’ of the Makariv Settlement Council,” Makariv Settlement Council, accessed January 6, 2023, https://makariv-crl.itmed.org/.
[96] Serhiy Solomenko, “How the Makariv Dispensary, Destroyed by the Russians, gets a New Life,” UkrInform, October 7, 2022, https://www.ukrinform.ua/rubric-regions/3588113-ak-zrujnovana-rosianami-makarivska-ambulatoria-otrimue-nove-zitta.html.
[97] Serhiy Solomenko, “How the Makariv Dispensary, Destroyed by the Russians, gets a New Life,” UkrInform, October 7, 2022, https://www.ukrinform.ua/rubric-regions/3588113-ak-zrujnovana-rosianami-makarivska-ambulatoria-otrimue-nove-zitta.html.
[98] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[99] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[100] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[101] Sarah Rainsford, “When an Ambulance Drove Out… the Russians Shot Right at It,” BBC, May 5, 2022, https://www.bbc.co.uk/news/live/world-europe-61330132. Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file). Note that the special protection afforded to hospitals and other medical units ceases when they are, for example, used as a shelter for able-bodied combatants, as an arms or ammunition dump, or as a military observation post. See ICRC, Commentary of 1987 on Additional Protocol I, Art. 13, para. 551, https://ihl-databases.icrc.org/en/ihl-treaties/api-1977/article-13/commentary/1987?activeTab=undefined. In such case, the hospital becomes a legitimate military objective. However, Additional Protocol I, Art. 13 makes it clear that the loss of protection is not instantaneous; it may only cease “after a warning has been given setting, whenever appropriate, a reasonable time-limit, and after such warning has remained unheeded.”
[102] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[103] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[104] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[105] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[106] Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, p. 29, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[107] Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, p. 30, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[108] Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, p. 30, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[109] Makariv Multiprofile Intensive Care Hospital, Facebook, March 22, 2022, https://www.facebook.com/hospital.makariv.adm/posts/496469798729539.
[110] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file). Note that Dr. Solomenko had been evacuated at the time of the March 28, 2022 strike, and reported the incident based on a discussion he had with a member of Ukraine’s Territorial Defense Forces who witnessed the attack.
[111] The estimated cost of the Primary Care Clinic’s loss of equipment is around 2.5 million Ukrainian hryvnias (approximately 68,000 US dollars). Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[112] See Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, Facebook, May 15, 2022, https://www.facebook.com/watch/?v=559894918897841.
[113] Information provided by weapons analyst (on-file). The BM-21 Grad is a multi-launch rocket system designed to be inaccurate, firing a salvo of up to 40 rockets in less than 20 seconds to saturate an area and damage as many targets as possible. The BM-21 Grad is deployed at the lowest tactical levels of the Russian military. Orders to fire are normally given by officers at the level of Major and likely at the level of Captain. Information provided by weapons analyst (on-file). See also Joely Thomas and Chiara Torelli, “Russia’s Dirty Dozen: An Examination of Russian Explosive Weapons Used in Ukraine,” Action On Armed Violence, January 18, 2023, https://aoav.org.uk/2023/russias-dirty-dozen/.
[114] “KSE Foundation will restore a local hospital in Makariv (Kyiv region),” Kyiv School of Economics, May 30, 2022, https://kse.ua/about-the-school/news/kse-foundation-will-restore-a-local-hospital-in-makariv-kyiv-region/.
[115] Head of the Kyiv Regional Military Oleksyi Kuleba, Telegram, July 10, 2022, https://t.me/OleksiyKuleba/1953.
[116] Makariv Multiprofile Intensive Care Hospital, Facebook, September 29, 2022, https://www.facebook.com/hospital.makariv.adm/posts/pfbid02fNfLkEV1qBu6FNLbFaxaDMkBsGDa7ZhAWgLfnqxu5arSLECq8T5B915YwaQAZfFhl.
[117] Interview with a representative of the Makariv Multiprofile Intensive Care Hospital [anonymous], UHC, January 26, 2023, (on-file).
[118] “Summary,” Treatment and diagnostic center Adonis-Makariv, accessed January 6, 2023, https://adonismakariv.business.site/. The construction cost was almost 13 million UAH. The clinic was built according to high energy-effective and eco-friendly standards. Most of its walls were constructed from wood, which is one of the reasons that a massive fire broke out after the clinic was struck.
[119] Paul P. Murphy, “Significant Destruction Seen in Makariv, a Ukrainian Village 30 Miles West of Kyiv,” CNN, March 12, 2022, https://edition.cnn.com/europe/live-news/ukraine-russia-putin-news-03-12-22/h_2ee0ca37b6577f631528c18edcf80e6d.
[120] Paul P. Murphy, “Significant Destruction Seen in Makariv, a Ukrainian Village 30 Miles West of Kyiv,” CNN, March 12, 2022, https://edition.cnn.com/europe/live-news/ukraine-russia-putin-news-03-12-22/h_2ee0ca37b6577f631528c18edcf80e6d.
[121] Interview with Dr. Serhiy Solomenko, UHC, December 13, 2022 (on-file).
[122] Denys Shaposhnikov, “How did the first battles around Chernihiv take place and what significance did the city have for the Russians?,” Suspilne, December 5, 2022, https://suspilne.media/327410-ak-vidbuvalis-persi-boi-navkolo-cernigova-ta-ake-znacenna-malo-misto-dla-rosian/.
[123] Ashleigh Stewart, “The Siege of Chernihiv: Residents Recount Five Weeks of Horror under Russian Terror,” Global News, May 4, 2022, https://globalnews.ca/news/8808055/chernihiv-ukraine-war-aftermath/; General Staff of the Armed Forces of Ukraine, Facebook, March 18, 2022, https://www.facebook.com/GeneralStaff.ua/posts/275463534766732: “In the Chernihiv region, [R]ussian occupiers are intimidating locals to quell civilian resistance.”
[124] Joshua Yaffa, “The Siege of Chernihiv,” The New Yorker, April 15, 2022, https://www.newyorker.com/news/dispatch/the-siege-of-chernihiv.
[125] “Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch,June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv.
[126] Notes of site visit, UHC, July 14-15, 2022 (on-file); Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, p. 46, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[127] Oleksandra Balandyukh, “God, Don’t Let Anyone Experience This,” Zaxid, May 10, 2022, https://zaxid.net/ne_day_bozhe_nikomu_take_perezhiti_n1542483. See also “Operational information on the occupancy of beds in health care institutions of the Chernihiv oblast designated for hospitalization of patients with a confirmed case of COVID-19” (updated February 8, 2022), Chernihiv Oblast State Administration, accessed January 6, 2023, https://ssd.cg.gov.ua/index.php?id=31676&tp=1.
[128] “Comfortable Beds for Patients. Chernihiv Regional Children’s Hospital Received Help from Benefactors,” Chernihiv City, January 14, 2022, https://chernihiv.city/articles/189182/zruchni-lizhka-dlya-paciyentiv-chernigivska-oblasna-dityacha-likarnya-otrimala-dopomogu-vid-blagodijnikiv.
[129] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[130] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file). According to Dr. Liutkevych, there were 200 people sheltering in the hospital.
[131] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[132] “Ukraine: Russian Air-Dropped Bombs Hit Residential Area,” Human Rights Watch, March 10, 2022, https://www.hrw.org/news/2022/03/10/ukraine-russian-air-dropped-bombs-hit-residential-area; Joely Thomas and Chiara Torelli, “Russia’s Dirty Dozen: An Examination of Russian Explosive Weapons Used in Ukraine,” Action On Armed Violence, January 18, 2023, https://aoav.org.uk/2023/russias-dirty-dozen/.
[133] Notes of site visit, UHC, July 14-15, 2022 (on-file); Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, pp. 31-32, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[134] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[135] Human Rights Watch, “Ukraine: Russian Air-Dropped Bombs Hit Residential Area,” March 10, 2022, https://www.hrw.org/news/2022/03/10/ukraine-russian-air-dropped-bombs-hit-residential-area.
[136] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[137] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[138] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[139] “Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch,June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv.
[140] Reports differ as to the date of the strike on City Hospital #2. See e.g. Ari Daniel, “Doctors in Chernihiv Bear Witness to their Hospital’s Fate after Russian Shelling,” NPR, April 7, 2022, https://www.npr.org/sections/goatsandsoda/2022/04/07/1091333939/doctors-in-chernihiv-bear-witness-to-their-hospitals-fate-after-russian-shelling (reporting that the strike occurred on March 16, 2022);“Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch,June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv (reporting that the strike occurred on March 17, 2022).
[141] According to eyewitnesses, explosions occurred sometime between 9:00 and 11:00 am on March 17, 2022. See Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, pp. 44-45, https://uhc.org.ua/en/2022/09/15/report-by-uhc/. This information was also confirmed by Truth Hounds, a Ukrainian organization that documents war crimes and crimes against humanity in the war contexts since 2014, following a confidential investigation into the attack, including through interviews with eyewitnesses.
[142] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file); “Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch,June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv.
[143] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[144] These figures are confirmed by Truth Hounds, a Ukrainian organization that documents war crimes and crimes against humanity in the war contexts since 2014, following a confidential investigation into the attack, including through interviews with eyewitnesses. See also “Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch, June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv; also “End Cluster Munition Attacks in Ukraine,” Human Rights Watch, May 11, 2022, https://www.hrw.org/report/2022/05/11/intense-and-lasting-harm/cluster-munition-attacks-ukraine. A doctor who spoke with Human Rights Watch said that there were at least 20 patients inside the hospital at the time of the attack. See “Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch,June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv. Most patients had remained in the hospital’s shelter after the previous air raid siren. However, some people, largely from neighboring areas who were sheltering in the hospital, were outside seeking warmth from the sun. Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[145] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[146] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[147] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file): “[T]here was no military equipment anywhere. There’s a morgue not far from us. The military brought and took their dead from there. We told them that [we have] children [here], urging them to leave, and they said “yes, no problem”, but they didn’t stay, of course, they didn’t stay, nothing like this happened.
[148] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file). Note that the special protection afforded to hospitals and other medical units does not cease when it is guarded by pickets, sentries, or an escort made up of soldiers or civilian uniformed police force. The mere presence of guards shelters them from attacks as they have no offensive role to play and are only there to protect the sick and wounded. See ICRC, Commentary of 1987 on Additional Protocol I, Art. 13, paras 565-68, https://ihl-databases.icrc.org/en/ihl-treaties/api-1977/article-13/commentary/1987?activeTab=undefined.
[149] “Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch,June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv.
[150] Like the BM-21 Grad, the BM-27 Uragan is designed to be inaccurate. The BM-27 Uragan was designed to fire a heavier warhead than the older and smaller BM-21 Grad. The BM-27 Uragan can fire 16 220 mm rockets within a range of up to 35 kilometers. Six different warheads are available for its rockets including high explosive, incendiary, chemical, a variety of ‘cargo’ modules that carry anti-material cluster munitions as well as more conventional scatterable anti-personnel and anti-armor mines. Each cargo module can carry about 30 munitions. The BM-27 Uragan is normally deployed at the level of rocket artillery regiments. Orders to fire are generally only given by relatively senior commanders of Colonel level and above. Information provided by weapons analyst (on-file). See also Joely Thomas and Chiara Torelli, “Russia’s Dirty Dozen: An Examination of Russian Explosive Weapons Used in Ukraine,” Action On Armed Violence, January 18, 2023, https://aoav.org.uk/2023/russias-dirty-dozen/: BM-27 Uragan can launch 16 220 mm rockets, which have a range of 34 kilometers.
[151] “Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch, June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv.
[152] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[153] “Ukraine: Russian Strikes Killed Scored of Civilians in Chernihiv,” Human Rights Watch, June 10, 2022, https://www.hrw.org/news/2022/06/10/ukraine-russian-strikes-killed-scores-civilians-chernihiv. See also “End Cluster Munition Attacks in Ukraine,” Human Rights Watch, May 11, 2022, https://www.hrw.org/report/2022/05/11/intense-and-lasting-harm/cluster-munition-attacks-ukraine: “Clearance teams destroyed the remnants of an Uragan cluster munition rocket and four unexploded 9N210 submunitions remaining from the attack.”
[154] Victoria Zhuhan and Clair Pres, “‘Everything around began to explode.’ The BBC’s investigation into the cluster bombardment in Chernihiv,” BBC, June 27, 2022, https://www.bbc.com/ukrainian/features-61908780.
[155] Notes of site visit, UHC, July 14-15, 2022 (on-file).
[156] See Joely Thomas and Chiara Torelli, “Russia’s Dirty Dozen: An Examination of Russian Explosive Weapons Used in Ukraine,” Action On Armed Violence, January 18, 2023, https://aoav.org.uk/2023/russias-dirty-dozen/: BM-27 Uragan can launch 16 220 mm rockets, which have a range of 34 kilometers.
[157] Suspilne, Facebook, July 6, 2022, https://www.facebook.com/suspilne.chernihiv/photos/pcb.5020472224742229/5020470618075723 (map as of March 6-22) See also Hugo Bachega and Orysia Khimiak, “In Chernihiv, Civilians are Trapped as Hospitals and Schools Attacked,” BBC, March 28, 2022, https://www.bbc.co.uk/news/world-europe-60860197 (map as of March 26).
[158] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[159] Ukraine Weapons Tracker, Twitter, March 1, 2022, https://twitter.com/UAWeapons/status/1498757834087051270.
[160] Daniel McLaughlin, “’We hit them with everything we had’: Ukrainian town fights off the Russians,” The Irish Times, April 29, 2022, https://www.irishtimes.com/news/world/europe/we-hit-them-with-everything-we-had-ukrainian-town-fights-off-the-russians-1.4865429; “Russia Ukraine War Day 7 | Russian troops attack Bashtanka in Ukraine,” CNN News18, March 2, 2022, https://www.msn.com/en-in/video/news/russia-ukraine-war-day-7-russian-troops-attack-bashtanka-in-ukraine-cnn-news18-latest-news/vi-AAUuPoY; Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file). Tochka-U are ground-based ballistic missile system that can be fitted with conventional, chemical, nuclear or cluster munitions. “Tochka-U missiles, which are out of production, are not used as frequently due to their shorter range (120km), but they have had deadly consequences for parts of Ukraine neighbouring Russian-occupied regions. Able to stray 150m off target, these indiscriminate missiles also pose a real threat to civilians when fired at populated areas.” In this sense, see Joely Thomas and Chiara Torelli, “Russia’s Dirty Dozen: An Examination of Russian Explosive Weapons Used in Ukraine,” Action On Armed Violence, January 18, 2023, https://aoav.org.uk/2023/russias-dirty-dozen/.
[161] “KNP Bashtanka Multiprofile Hospital,” Bashtanka City Council, Mykolaiv oblast, accessed January 6, 2023, https://xn--80aaab1cr7azc.xn--k1ajr.xn--j1amh/vid-istorii-do-sohodennia/.
[162] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[163] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[164] Information provided by weapons analyst (on-file).
[165] Daniel McLaughlin, “‘We hit them with everything we had’: Ukrainian town fights off the Russians,” The Irish Times, April 29, 2022, https://www.irishtimes.com/news/world/europe/we-hit-them-with-everything-we-had-ukrainian-town-fights-off-the-russians-1.4865429.
[166] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file). The doctor explains that at the beginning of March, the hospital served as a “first-line” hospital due to its proximity to the frontline, but as the fighting progressed they became a “second-line” hospital. Ibid. Note that the special protection afforded to hospitals and other medical units does not cease when members of the armed forces are in the hospital or unit for medical reasons. See ICRC, Commentary of 1987 on Additional Protocol I, Art. 13, paras 571-74, https://ihl-databases.icrc.org/en/ihl-treaties/api-1977/article-13/commentary/1987?activeTab=undefined.
[167] “Ukraine War: Hospital destroyed by Russian missile in southern Ukraine,” Sky News, April 22, 2022, https://www.youtube.com/watch?v=ff1eF2JSfnE.
[168] Information provided by weapons analyst (on-file). The identification of the type of missile is based on the munition remains shown in the following video: “Ukraine War: Hospital destroyed by Russian missile in southern Ukraine,” Sky News, April 22, 2022, https://www.youtube.com/watch?v=ff1eF2JSfnE. According to Action On Armed Violence, an organization conducting research and advocacy on the incidence and impact of global armed violence, “[t]he Kalibr missile is Russia’s most advance cruise missile, and has ship-launched, submarine-launched, and air-launched versions.” Joely Thomas and Chiara Torelli, “Russia’s Dirty Dozen: An Examination of Russian Explosive Weapons Used in Ukraine,” Action On Armed Violence, January 18, 2023, https://aoav.org.uk/2023/russias-dirty-dozen/.
[169] Information provided by weapons analyst (on-file).
[170] Information provided by weapons analyst (on-file).
[171] Information provided by weapons analyst (on-file).
[172] Information provided by weaponsanalyst (on-file); Joely Thomas and Chiara Torelli, “Russia’s Dirty Dozen: An Examination of Russian Explosive Weapons Used in Ukraine,” Action On Armed Violence, January 18, 2023, https://aoav.org.uk/2023/russias-dirty-dozen/.
[173] A polyclinic is a clinic or health care facility that provides both general and specialist examinations and treatments for a wide variety of diseases and injuries to outpatients.
[174] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[175] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[176] Anastasiya Zubova, “Healthcare Under Fire: Russian Troops Destroy Medical Facilities in the Mykolaiv Region,” Bihus, July 11, 2022, https://bihus.info/healthcare_under_fire_russian_troops_destroy/.
[177] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[178] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[179] “Ukraine War: Hospital destroyed by Russian missile in southern Ukraine,” Sky News, April 22, 2022, https://www.youtube.com/watch?v=ff1eF2JSfnE.
[180] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[181] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[182] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[183] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[184] Anastsasiya Zubova, “Healthcare Under Fire: Russian Troops Destroy Medical Facilities in the Mykolaiv Region,” Bihus, July 11, 2022, https://bihus.info/healthcare_under_fire_russian_troops_destroy/.
[185] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file). See also TPYXA, Twitter, April 20, 2022, https://twitter.com/TpyxaNews/status/1516659728146857986?ref_src=twsrc%5Etfw%7Ctwcamp%5Etweetembed%7Ctwterm%5E1516659728146857986%7Ctwgr%5E840bccaf8182ea9931c9ebc8e09337d10045f9ec%7Ctwcon%5Es1_&ref_url=https%3A%2F%2Feyesonrussia.org%2Fevent%2Fevent_3199_1650409200000 (video verified by Bellingcat and reviewed by Center for Information Resilience, see https://eyesonrussia.org/).
[186] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[187] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[188] Daniel McLaughlin, “‘We hit them with everything we had’: Ukrainian town fights off the Russians,” The Irish Times, April 29, 2022, https://www.irishtimes.com/news/world/europe/we-hit-them-with-everything-we-had-ukrainian-town-fights-off-the-russians-1.4865429.
[189] Daniel McLaughlin, “‘We hit them with everything we had’: Ukrainian town fights off the Russians,” The Irish Times, April 29, 2022, https://www.irishtimes.com/news/world/europe/we-hit-them-with-everything-we-had-ukrainian-town-fights-off-the-russians-1.4865429.
[190] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[191] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[192] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[193] Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[194] Thomas Gibbons-Neff, Natalia Yermak, “This is True Barbarity: Life under Russian Occupation,” New York Times, April 3, 2022, https://www.nytimes.com/2022/04/03/world/europe/ukraine-war-russia-trostyanets.html.
[195] Christopher Reuter, “A Visit to Trostyanets After the End of the Occupation,” Der Spiegel, March 30, 2022, https://www.spiegel.de/international/europe/liberated-from-the-russians-a-visit-to-trostyanets-after-the-end-of-the-occupation-a-c088be53-5f6c-4059-8d46-68803276e473.
[196] Thomas Gibbons-Neff, Natalia Yermak, “This is True Barbarity: Life under Russian Occupation,” New York Times, April 3, 2022, https://www.nytimes.com/2022/04/03/world/europe/ukraine-war-russia-trostyanets.html. One resident, Dr. Volkova, reported that, “They would not give us any green corridors, they searched the apartments, took away the phones, abducted people — they took them away, mostly young men, and we still don’t know where these people are.” Ibid.
[197] Dmytro Synyak, “‘The Russians Turned the Whole City into an Entire Wound…’ Interview with the Mayor of Trostyanets,” Decentralization, June 27, 2022, https://decentralization.gov.ua/en/news/14726.
[198] Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, p. 25, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[199] “Russian Occupation Leaves Scars on Trostyanets,” Deutsche Welle, July 2, 2022, https://www.dw.com/en/russian-occupation-leaves-scars-on-trostyanet/video-62136969; Notes of site visit, UHC, August 11, 2022 (on-file).
[200] Thomas Gibbons-Neff, Natalia Yermak, “This is True Barbarity: Life under Russian Occupation,” New York Times, April 3, 2022, https://www.nytimes.com/2022/04/03/world/europe/ukraine-war-russia-trostyanets.html.
[201] Notes of site visit, UHC, August 11, 2022 (on-file).
[202] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[203] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[204] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file); Notes of site visit, UHC, August 11, 2022 (on-file). See also Dmytro Zhyvytskyi, Telegram, March 19, 2022, https://t.me/Zhyvytskyy/1260.
[205] The doctor identified the Russian officer by name. Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[206] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[207] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[208] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[209] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[210] Franco Ordoñez, Olena Lysenko, “Ukrainian Doctors Describe Delivering Babies as Russia Shelled the Hospital,” NPR, April 26, 2022, https://www.knkx.org/2022-04-26/ukrainian-doctors-describe-delivering-babies-as-russia-shelled-the-hospital.
[211] Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, pp. 25-27, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[212] Both T-72 and T-80 tanks were reportedly used to hit the Trostianets City Hospital, possibly at different dates. See Office of the Prosecutor General of Ukraine, “Another Russian serviceman who ordered to shell the Trostianetska hospital from a tank has been identified,” August 17, 2022, https://www.gp.gov.ua/ua/posts/vstanovleno-shhe-odnogo-viiskovosluzbovcya-rf-yakii-viddav-nakaz-obstrilyuvati-z-tanka-trostyanecku-likarnyu (identifying a T-80 tank); State Bureau of Investigation of Ukraine, “The SBI Identified Russian Service Members who, with Tanks, were Firing at a Hospital in Trostyanets,” May 5, 2022, https://dbr.gov.ua/en/news/dbr-vstanovilo-vijskovosluzhbovciv-rf-yaki-z-tankiv-rozstrilyuvali-likarnyu-v-trostyanci (identifying a T-72 tank). The T-80 tank is a cheaper and more reliable version of the T-72 tank; both of which have been reportedly used to equip Russian elite units in the 2022 conflict in Ukraine. The T-80 uses the same 125 mm 2A46 smoothbore gun as the T-72, which can fire regular high explosive (4,000-meter range) and armor piercing shells (3,000-meter range) as well as the 9M119 ‘Svir’ anti-tank guided missile (5,000-meter range). The T-80 and T-72 tanks use similar sighting systems from the 1970s and are, therefore not as accurate as those of modern NATO armored vehicles. Information provided by weapons analyst (on-file).
[213] “Russian Occupation Leaves Scars on Trostyanets,” Deutsche Welle, July 2, 2022, https://www.dw.com/en/russian-occupation-leaves-scars-on-trostyanet/video-62136969; “Locals look to rebuild their lives in liberated Trostianets,” The Irish Times, March 31, 2022, https://www.irishtimes.com/news/world/europe/locals-look-to-rebuild-their-lives-in-liberated-trostianets-1.4841334; Dzerkalo Tyzhnia, Telegram, August 17, 2022, https://t.me/znua_live/51689. According to the town head of Trostianets Yuri Bova “[o]n the 23rd of March, there were two tanks. They drove out to the street and began to fire directly at the hospital.” “Having Seen the Conditions in the Trostianets Hospital, the Invaders Began to Shoot at It with a Tank,” Television Service of News, April 17, 2022, https://tsn.ua/en/ato/having-seen-the-conditions-in-the-trostianets-hospital-the-invaders-began-to-shoot-at-it-with-a-tank-2039266.html. The State Bureau of Investigations mentions several tanks surrounding the hospital and opening fire. See State Bureau of Investigations, Telegram, 20 May, 2022, https://t.me/DBRgovua/2508. There is also unsourced footage of a tank firing directly at a building that matches the features of the hospital: Pavlo Kovtoniuk, Twitter, April 2, 2022, https://twitter.com/pavlokovtonyuk/status/1510163664061480968.
[214] Notes of site visit, UHC, August 11, 2022 (on-file).
[215] Notes of site visit, UHC, August 11, 2022 (on-file).
[216] “Ukraine war: Medic’s shock over Russian tank hospital hit,” BBC, May 18, 2022, https://www.bbc.co.uk/news/uk-england-leicestershire-61485495. See also Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[217] Office of the Prosecutor General of Ukraine, “Another Russian serviceman who ordered to shell the Trostianetska hospital from a tank has been identified,” August 17, 2022, https://www.gp.gov.ua/ua/posts/vstanovleno-shhe-odnogo-viiskovosluzbovcya-rf-yakii-viddav-nakaz-obstrilyuvati-z-tanka-trostyanecku-likarnyu.
[218] State Bureau of Investigation of Ukraine, “The SBI Identified Russian Service Members who, with Tanks, were Firing at a Hospital in Trostianets,” May 5, 2022, https://dbr.gov.ua/en/news/dbr-vstanovilo-vijskovosluzhbovciv-rf-yaki-z-tankiv-rozstrilyuvali-likarnyu-v-trostyanci; State Bureau of Investigation of Ukraine, “The SBI Put on the Wanted List the Russian Tankers who Shot the Local Hospital during the Occupation of Trostianets. The Repaired Tank ‘Takes Revenge’ on Former Owners for their Crimes,” October 24, 2022, https://dbr.gov.ua/en/news/dbr-ogolosilo-v-rozshuk-rosijskih-tankistiv-yaki-pid-chas-okupacii-trostyancya-rozstrilyali-miscevu-likarnyu.-vidremontovanij-tank-mstit-kolishnim-gospodaryam-za-zlochini.
[219] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[220] Notes of site visit, UHC, August 11, 2022 (on-file).
[221] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[222] Notes of site visit, UHC, August 11, 2022 (on-file).
[223] Notes of site visit, UHC, August 11, 2022 (on-file).
[224] Dmytro Zhyvytskyi Telegram, March 28, 2022, https://t.me/Zhyvytskyy/1443.
[225] India Today, Facebook, April 21, 2022, https://www.facebook.com/IndiaToday/videos/inside-a-hospital-in-trostyanets-sumy-region-of-ukraine/543236797447222/.
[226] Taras Kaidan et al., “A Ukrainian Mayor Looks at Life After Liberation,” Bloomberg, April 12, 2022, https://www.bloomberg.com/news/features/2022-04-12/ukraine-town-mayor-confronts-ruins-rebuilding-after-liberation.
[227] “Trostyanets Town Hospital,” United 24, accessed January 6, 2023, https://u24.gov.ua/needs/trostyanets_town_hospital.
[228] “The destroyed Trostyanets Hospital Resumes its Activities,” AAM, June 9, 2022, https://aam.com.ua/en/2022/06/09/the-destroyed-trostyanets-hospital-resumes-its-activities/.
[229] “The destroyed Trostyanets Hospital Resumes its Activities,” AAM, June 9, 2022, https://aam.com.ua/en/2022/06/09/the-destroyed-trostyanets-hospital-resumes-its-activities/; National Agency ZDOROVI, Instagram, April 28, 2022, https://www.instagram.com/p/Cc40DBmJjuL/.
[230] Alina Moh, “A German-Designed Mobile Hospital will be Built in Trostianets,” Pragmatika, September 26, 2022,https://pragmatika.media/en/news/u-trostjanci-sporudjat-mobilnu-likarnju-za-nimeckoju-rozrobkoju/.
[231] Geneva Convention IV, Art. 21.
[232] Additional Protocol I, Art. 21.
[233] Irina Venediktova, Facebook, February 26, 2022, https://www.facebook.com/irina.venediktova.31/posts/pfbid021AtYKbsbMAMBscx6fHmt2dm8sb42K3wBCMu6cTcoAS2fswEaJkJLW96WoxNo3BbBl; “Near Kherson, Russian Troops Overturned an Ambulance Carrying a Wounded Man,” UkrInform, February 26, 2022,https://www.ukrinform.ua/rubric-regions/3413928-pid-hersonom-rosijski-vijska-pidbili-svidku-aka-vezla-poranenih.html; “Civilian Toll Rises as Russians Enter Kherson,” Institute for War & Peace Reporting, March 1, 2022, https://iwpr.net/global-voices/civilian-toll-rises-russians-enter-kherson.
[234] Euromaidan Press, Twitter, February 26, 2022, https://twitter.com/EuromaidanPress/status/1497635178805698562?s=20&t=anX5wqUizRB5PIw4WCkYwQ.
[235] Victoria Bondarenko, “Shelling of an ‘Ambulance’ in Poltava Region: How it all Happened,” Suspilne, February 27, 2022,https://suspilne.media/211692-obstril-svidkoi-na-poltavsini-ak-use-stalosa/.
[236] Ihor Izotov, “‘Hadyatsky Safari’: Memories of Locals who Stopped the Russian Military in the North of Poltava Oblast,” Suspilne, July 11, 2022,https://suspilne.media/258713-gadacke-safari-spogadi-miscevih-aki-zupinali-rosijskih-vijskovih-na-pivnoci-poltavsini/.
[237] Victoria Bondarenko, “Shelling of an ‘Ambulance’ in Poltava Region: How it all Happened,” Suspilne, February 27, 2022,https://suspilne.media/211692-obstril-svidkoi-na-poltavsini-ak-use-stalosa/.
[238] Konstantin Shirokun, “Russian soldiers fired at the door to help on the way from Sumy to Kiev,” RBC-Ukraine, March 4, 2022, https://www.rbc.ua/ukr/news/rossiyskie-voennye-obstrelyali-skoruyu-pomoshch-1646384952.html; Insecurity Insight, “Violence Against or Obstruction of Health Care in Ukraine,” March 3-12, 2022, https://insecurityinsight.org/wp-content/uploads/2022/03/Violence-Against-or-Obstruction-of-Health-Care-in-Ukraine-03-12-March-2022.pdf.
[239] Konstantin Shirokun, “Russian soldiers fired at the door to help on the way from Sumy to Kiev,” RBC-Ukraine, March 4, 2022, https://www.rbc.ua/ukr/news/rossiyskie-voennye-obstrelyali-skoruyu-pomoshch-1646384952.html.
[240] Dmytro Zhyvytskyi, Facebook, March 4, 2022, https://www.facebook.com/Zhyvytskyy/posts/pfbid02iSLcjjvXB8hYh3o7cCsPbccq3rkNEXmCxNSQNjW4sHd8xGuy3tMY7qfq9xgPNRNsl.
[241] Yuriy Bova, Facebook, March 12, 2022, https://www.facebook.com/yura.bova.trostyanets/posts/pfbid0h5boWYaUmi3r32wwpJeEu7Bu63P94W8jzRuYo6MsEL5u1qUCo7357sQyVha84154l. See also Dmytro Zhyvytskyi, Telegram, March 13, 2022, https://t.me/Zhyvytskyy/1099. In an interview with UHC, a doctor confirmed this information: “In the first days of the occupation, there was an unreasonable instruction to accompany the green corridor column with an ambulance. Other ambulances (two or three) were stolen by Russians.” Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[242] Dmytro Zhyvytskyi, Telegram, March 4, 2022, https://t.me/Zhyvytskyy/768.
[243] Office of the Prosecutor General of Ukraine, Telegram, December 13, 2022, https://t.me/pgo_gov_ua/8099. See also Head of the Kharkiv Oblast Military Administration Oleg Synyehubov, Telegram, December 13, 2022, http://t.me/synegubov/5032. S-300 missiles are designed as anti-aircraft or anti-missile missiles. They are guided to their target by a separate ground-based radar array. However, when used against ground targets, S-300 missiles are not particularly accurate. Information provided by weapons analyst (on-file). See also “Factbox: What is the S-300 missile that is reported to have hit Poland?,” Reuters, November 16, 2022, https://www.reuters.com/world/europe/what-is-s-300-missile-that-is-reported-have-hit-poland-2022-11-16/: “The S-300 is a family of surface-to-air missiles, originally developed by the Soviet Union. S-300 missiles are intended to shoot down aircraft, drones and incoming cruise and ballistic missiles. Full S-300 launchers include detection radars that track incoming targets. Missiles are equipped with guidance systems to automatically latch on to targets.”
[244] Office of the Prosecutor General of Ukraine, Telegram, December 13, 2022, https://t.me/pgo_gov_ua/8099.
[245] Center for Emergency Medical Aid and Disaster Medicine, Facebook, March 12, 2022, https://www.facebook.com/ekstrena.dopomoga.kh/posts/493387372385092. See also Anna Tsyomyk, “An Ambulance in Kharkiv Came under Fire: a Paramedic was Injured,” Suspilne, March 12, 2022, https://suspilne.media/216646-svidka-u-harkovi-potrapila-pid-obstril-feldserka-svidkoi-otrimala-poranenna/.
[246] Center for Emergency Medical Aid and Disaster Medicine, Facebook, March 12, 2022, https://www.facebook.com/ekstrena.dopomoga.kh/posts/493387372385092.
[247] Chernihiv’s main bridge was reportedly blown up by Russian forces on March 23, 2022. See “Live Updates: Governor: Russians Destroyed Chernihiv Bridge,” The Independent,March 23, 2022, https://www.independent.co.uk/news/ukraine-ap-lviv-dmitry-peskov-kyiv-b2041939.html.
[248] Interview with Dr. Mykola Liutkevych, UHC, July 15, 2022 (on-file).
[249] Natalia Popova, Telegram, October 2, 2022, https://t.me/krotkh/1005.
[250] Center for Emergency Medical Aid and Disaster Medicine, Facebook, October 2, 2022, https://www.facebook.com/ekstrena.dopomoga.kh/posts/pfbid0276KRpmW8sN1FMjVDavhSG3K6BAANrp1Nds6fp7qYWA3NJACPYPv4St5Vbh18Sh9Jl; Natalia Popova, Telegram, October 2, 2022, https://t.me/krotkh/1005; Head of the Kharkiv Oblast Military Administration Oleg Synyehubov, Telegram, October 3, 2022, https://t.me/synegubov/4392.
[251] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[252] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[253] Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, pp. 25-27, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[254] Interview with a doctor at the Trostianets City Hospital [anonymous], UHC, August 11, 2022 (on-file).
[255] Ambulance stations in Ukraine house medical vehicles but also serve broader purposes for the community, including hosting trainings and/or storing medications. During the height of the COVID-19 pandemic, some stations served as vaccination centers.
[256] “The Russians Captured Kreminna and Killed Several Civilians, Evacuation in Impossible, Fighting Continues, Gayday,” Espreso TV, April 18, 2022, https://espreso.tv/rosiyski-viyska-zayshli-u-kreminnu-trivayut-vulichni-boi-evakuatsiya-nemozhliva-ova.
[257] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[258] Stanislav Miroshnychenko and Olha Reshetylova, “Road of Death: The Shooting of Civilians on Kreminna-Lyman Road,” Media Initiative for Human Rights, October 28, 2022, https://mipl.org.ua/en/the-road-of-death-the-shooting-of-civilians-on-the-kreminna-lyman-road/.
[259] MIHR’s investigation, based on field and remote research, including interviews and an analysis of photographs, video recordings, satellite imagery, and open-source information, provides an in-depth analysis of the Lyman attack, which appeared to be part of a broader attack on civilians who were fleeing the shelling by Russian forces of Kreminna along the Torske-Kreminna highway. See Stanislav Miroshnychenko and Olha Reshetylova, “Road of Death: The Shooting of Civilians on Kreminna-Lyman Road,” Media Initiative for Human Rights, October 28, 2022, https://mipl.org.ua/en/the-road-of-death-the-shooting-of-civilians-on-the-kreminna-lyman-road/.
[260] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[261] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[262] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[263] Stanislav Miroshnychenko and Olha Reshetylova, “Road of Death: The Shooting of Civilians on Kreminna-Lyman Road,” Media Initiative for Human Rights, October 28, 2022, https://mipl.org.ua/en/the-road-of-death-the-shooting-of-civilians-on-the-kreminna-lyman-road/.
[264] Stanislav Miroshnychenko and Olha Reshetylova, “Road of Death: The Shooting of Civilians on Kreminna-Lyman Road,” Media Initiative for Human Rights, October 28, 2022, https://mipl.org.ua/en/the-road-of-death-the-shooting-of-civilians-on-the-kreminna-lyman-road/.
[265] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[266] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[267] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[268] See Stanislav Miroshnychenko and Olha Reshetylova, “Road of Death: The Shooting of Civilians on Kreminna-Lyman Road,” Media Initiative for Human Rights, October 28, 2022, https://mipl.org.ua/en/the-road-of-death-the-shooting-of-civilians-on-the-kreminna-lyman-road/.
[269] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[270] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[271] Interview with paramedic [anonymous], MIHR, November 22, 2022 (on-file).
[272] Geneva Convention IV, Art. 55; Additional Protocol I, Art. 14.
[273] “Russians engaging in mass theft of medical equipment, says Zelenskiy,” Reuters, October 28, 2022, https://www.reuters.com/world/europe/russians-engaging-mass-theft-medical-equipment-says-zelenskiy-2022-10-28/.
[274]Information provided by the head of the medical department of Kyiv Regional Military Administration, UHC, May 3, 2022 (on-file).
[275] Anna Mamonova et al., “The Hardest Thing is When they Bring Friends, and they are in Agony, and you are Powerless,” Babel, November 10, 2022,https://babel.ua/texts/86822-nayvazhche-koli-privozyat-znayomih-a-voni-v-agoniji-i-ti-bezsiliy-likar-z-izyumu-p-yat-misyaciv-okupaciji-zhiv-u-pidvali-likarni-i-operuvav-bez-anesteziji-poranenih-ta-katovanih-os-yogo-istoriya.
[276] Mariupol City Council, Telegram, April 29, 2022, https://t.me/mariupolrada/9447.
[277] Department of Intelligence of the Ministry of Defense of Ukraine, Telegram, May 1, 2022, https://t.me/DIUkraine/433.
[278] Luhansk Military Administration, Telegram, May 10, 2022, https://t.me/luhanskaVTSA/2478.
[279] Ukrainian Healthcare Center, “Massive. Brutal. Deliberate. Attacks on Hospitals in the Russia-Ukraine War during the First Phase of the Invasion,” September 2022, pp. 41-43, https://uhc.org.ua/en/2022/09/15/report-by-uhc/.
[280] Tatyana Fedorkova, “Russian troops have captured Balaklia and are blocking Kharkiv from the north — General Staff,” Suspilne, March 4, 2022, https://suspilne.media/213600-vijska-rf-zahopili-balakliu-i-blokuut-harkiv-z-pivnoci-genstab/.
[281] Oleg Kononenko, “The Ukrainian flag is already flying over Balaklia – video,” New Voice of Ukraine, September 8, 2022, https://nv.ua/ukr/ukraine/events/zvilnennya-balakliji-u-misti-vivisili-ukrajinskiy-prapor-video-novini-ukrajini-50268723.html.
[282] Mykola Melnyk, “An Updated Intensive Care Unit will be Opened in the Balakli District,” Slobidsky Krai, June 14, 2018, https://www.slk.kh.ua/news/oblast-online/u-balaklijskomu-rajoni-vidkriyetsya-onovlene-reanimacijne-viddilennya.html.
[283] “‘Balakliya Clinical Multidisciplinary Intensive Care Hospital’ Received Medical and Laboratory Equipment in November,” Healthy Future, December 1, 2022, https://healthyfuture.com.ua/en/projects/ourprojects/balakleya-medical-and-lab-equipment.html.
[284] Mykola Melnyk, “An Updated Intensive Care Unit will be Opened in the Balakli District,” Slobidsky Krai, June 14, 2018, https://www.slk.kh.ua/news/oblast-online/u-balaklijskomu-rajoni-vidkriyetsya-onovlene-reanimacijne-viddilennya.html.
[285] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[286] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[287] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file); Oleg Synyehubov, head of the Kharkiv Regional State administration, Telegram, April 2, 2022, https://t.me/synegubov/2789; “Russian Military Shells Occupied Balakliya Again, 3 People Killed – Prosecutor’s Office,” Interfax Ukraine, April 7, 2022, https://interfax.com.ua/news/general/821912.html.
[288] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[289] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[290] “Russians Loot Hospitals in Kharkiv Oblast – Loss of Equipment are at 95%,” Pravda,September 20, 2022, https://www.pravda.com.ua/eng/news/2022/09/20/7368361/.
[291] “‘Balakliya Clinical Multidisciplinary Intensive Care Hospital’ Received Medical and Laboratory Equipment in November,” Healthy Future, December 1, 2022, https://healthyfuture.com.ua/en/projects/ourprojects/balakleya-medical-and-lab-equipment.html.
[292] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[293] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[294] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[295] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[296] “UNICEF Provides Medical Supplies to Hospital in Balakliya,” UNICEF,January 10, 2023, https://www.unicef.org/ukraine/en/stories/medical-supplies-to-hospital-in-balakliya.
[297] Interview with Dr. Maryna Rudenko, UHC, November 18, 2022 (on-file).
[298] “In Balakliia, the Multiprofile Hospital Destroyed by the Occupiers Resumed Work,” Kharkiv Regional Military Administration, January 3, 2023, https://kharkivoda.gov.ua/news/119057; “UNICEF Provides Medical Supplies to Hospital in Balakliya,” UNICEF,January 10, 2023, https://www.unicef.org/ukraine/en/stories/medical-supplies-to-hospital-in-balakliya.
[299] “Part of Kherson Region Territory Occupied by Aggressor – Regional Administration,” Interfax Ukraine, February 24, 2022, https://en.interfax.com.ua/news/general/801461.html. On September 30, 2022, the Kherson oblast was illegally annexed by Russia. See Pjotr Sauer and Luke Harding, “Putin Annexes Four Regions of Ukraine in Major Escalation of Russia’s War,” The Guardian, September 30, 2022, https://www.theguardian.com/world/2022/sep/30/putin-russia-war-annexes-ukraine-regions.
[300] The hospital has 19 inpatient departments, 11 of which are surgical departments. The hospital has 565 beds, where more than 23,000 patients are treated annually. More than 15,000 surgeries are performed annually. See “Kherson Regional Clinical Hospital,” accessed January 6, 2023, https://www.oblhospital.com.ua.
[301] Interview with a doctor at the Kherson Regional Clinic Hospital [anonymous], MIHR, October 23, 2022 (on-file); Interview with a doctor at the Kherson Regional Clinic Hospital [anonymous], MIHR, October 28, 2022 (on-file) For additional reporting, see Anastasia Pantelieieva, “Medicine in the Occupation: A Curator from Tuva, Russian doctors and Detention for Refusing to Cooperate,” Media Initiative for Human Rights (November 10, 2022), https://mipl.org.ua/en/medicine-under-occupation-overseer-from-tuva-russian-doctors-and-detention-for-refusing-to-cooperate/.
[302] Upon occupying the building, Russian authorities renamed it as the “Ministry of Health Protection of Kherson Region.”
[303] “2014 – the start of the Anti-terrorist operation in the east of Ukraine was officially announced,” Ukraine’s Institute of Memory, April 14, 2021, https://uinp.gov.ua/istorychnyy-kalendar/kviten/14/2014-oficiyno-ogolosheno-pro-pochatok-antyterorystychnoyi-operaciyi-na-shodi-ukrayiny. On April 14, 2014, an anti-terrorist operation was launched to liberate the territories of the Donetsk and Luhansk regions of Ukraine captured by Russian-controlled militants. The operation ended on April 30, 2018. The launch of the operation was preceded by the annexation of Crimea and the escalation of tension in the south and east of Ukraine, which were accompanied by the seizure of the premises of the Security Service of Ukraine, police and administrative buildings, and the declaration of the so-called “People’s Republics.” After April 2018, the Operation of the United Forces was launched under the leadership of the Armed Forces of Ukraine.
[304] “The Occupation Authorities of the Kherson Region Force Doctors to Cooperate,” Suspilne, June 20, 2022,https://suspilne.media/252113-okupacijna-vlada-hersonsini-primusue-medikiv-do-spivpraci/.
[305] Names of alleged collaborators are not made public in this report but, to the extent the authoring organizations are aware of them, will be made available to interested prosecutors and accountability mechanisms upon request.
[306] Interview with Dr. Oksana Kyrsanova, MIHR, March 19, 2022 (on-file); Interview with Dr. Oksana Kyrsanova, MIHR, December 2, 2022 (on-file).
[307] In 2014, after the occupation of Donetsk, the Donetsk Regional Hospital was relocated to Mariupol and became part of Mariupol City Hospital No. 2. On December 22, 2016, the hospital was renamed the Mariupol Regional Intensive Care Hospital. In 2021, 14,732 surgeries were performed at the hospital, and 74,197 patients received treatment. See “Regional Hospital for Intensive Care,” accessed January 6, 2023, http://mariupol.medkontrol.pro/oblastnaya-bolnica-intensivnogo-lecheniya-g-mariupolya; Donetsk State Administration, “Order of the Head of the Regional State Administration No. 1163 dated 22.12.2016 “On acceptance into joint ownership of the territorial communities of villages, towns, and cities under the management of the regional council, of the integral property complex of the communal institution ‘Mariupol City Hospital No. 2,’” December 22, 2016, https://web.archive.org/web/20170118053235/http://dn.gov.ua/rozporyadzhennya-golovy-oda-vid-22-12-2016-1163-pro-pryjnyattya-do-spilnoyi-vlasnosti-terytorialnyh-gromad-sil-selyshh-mist-shho-znahodytsya-v-upravlinni-oblasnoyi-rady-tsilisnogo-majnovogo-kompleksu/.
[308] See “They Spent Three Weeks in the Hell of Mariupol: The Doctor who Managed to Get Out Talked about his Experience,” Bug, March 31, 2022,http://bug.org.ua/interview/try-tyzhni-proviv-u-pekli-mariupolya-likar-yakomu-vdalosya-vybratysya-rozpoviv-pro-perezhyte-650256/.
[309] Matt Murray, “Ukraine War: Refugee tells of wife’s death after maternity hospital bombing,” BBC, November 11, 2022, https://www.bbc.com/news/uk-wales-63588749.
[310] Dr. Kyrsanova did not remember the exact date, but said that the missile hit the hospital before March 12, 2022. Interview with Dr. Oksana Kyrsanova, MIHR, December 2, 2022 (on-file). Other witnesses reported bombings in the area on March 10 and 11, 2022. See “‘They Drove a Tank and Two Armored Personnel Carriers and Started Shooting Houses Around…’ How the Russians Captured the Hospital in Mariupol, and What Happened There After That,” 0629.com.ua Mariupol City Website, March 31, 2022, https://www.0629.com.ua/news/3362062/voni-prignali-tank-i-dva-btra-i-pocali-rozstriluvati-budinki-navkolo-ak-rosiani-zahopili-likarnu-v-mariupoli-i-so-tam-vidbuvalos-pisla-cogo; “Armoury, Prison, Graveyard: Mariupol Intensive Care Hospital under Russian Occupation,” International Partnership for Human Rights, Truth Hounds, Global Diligence, November 2022, https://www.iphronline.org/wp-content/uploads/2022/11/Mariupol-report_for_distribution_final_1.pdf.
[311] The doctor only agreed to be identified with the initial of his first name, to focus the interview on the living and working conditions of health workers and other prisoners generally, rather than his own personal experience only.
[312] Interview with Dr. Y, MIHR, November 24, 2022 (on file).
[313] Garrison Hospital No. 555 in Mariupol had been established in July 2020.
[314] For additional reporting, see Media Initiative for Human Rights, “Medic from Mariupol: ‘Doctors operated in bulletproof vests and helmets, did not take them off for several days,’” July 12, 2022, https://mipl.org.ua/medyk-iz-mariupolya-likari-operuvaly-v-bronezhyletah-i-kaskah-ne-znimaly-yih-po-kilka-dib/.
[315] On “filtration camps” and the crime of forcible transfer, see Human Rights Watch, “‘We Had No Choice’: ‘Filtration’ and the Crime of Forcibly Transferring Ukrainian Civilians to Russia,” September 2022, https://www.hrw.org/report/2022/09/01/we-had-no-choice/filtration-and-crime-forcibly-transferring-ukrainian-civilians#4455.
[316] On the night of July 28-29, a large explosion in one of the barracks killed 53 Ukrainian prisoners of war and injured at least 75 others. Following requests from both Ukraine and Russia, the United Nations appointed a fact-finding mission to investigate the incident on August 3, 2022. See “Members of Fact-Finding Mission regarding Incident at Olenivka, Ukraine, on 29 July 2022,” United Nations Secretary-General Press Statement, August 22, 2022, https://www.un.org/sg/en/content/sg/personnel-appointments/2022-08-22/members-of-fact-finding%C2%A0mission-regarding-incident-olenivka-ukraine-29-july-2022%C2%A0.https://www.un.org/sg/en/content/sg/personnel-appointments/2022-08-22/members-of-fact-finding%C2%A0mission-regarding-incident-olenivka-ukraine-29-july-2022%C2%A0. The fact-finding mission was disbanded in January 2023 because the “UN mission cannot deploy to the site.” “Russia-Ukraine War Live,” The Guardian, January 5, 2023, https://www.theguardian.com/world/live/2023/jan/05/russia-ukraine-war-live-no-rational-reason-west-hasnt-sent-tanks-says-zelenskiy-as-allies-offer-armoured-vehicles-instead?page=with:block-63b72a3a8f084f5e7540c7f6#block-63b72a3a8f084f5e7540c7f6.
[317] See Tetyana Katrychenko et al., “Crimes in Olenivka: Chronology, Testimonies and Names of Those Involved,” Media Initiative for Human Rights, December 1, 2022, https://mipl.org.ua/en/crimes-in-olenivka-chronology-testimonies-and-names-of-those-involved/.
[318] The current Criminal Code of Ukraine was adopted on April 5, 2001 and came into force on September 1, 2001, with subsequent amendments since. It replaced the 1960 Criminal Code of the Ukrainian SSR. See http://www.encyclopediaofukraine.com/display.asp?linkpath=pages%5CC%5CR%5CCriminalCodeofUkraine.htm.
[319] See “What is Universal Jurisdiction,” TRIAL International, accessed January 6, 2023, https://trialinternational.org/topics-post/universal-jurisdiction/.
[320] See “Statement Calling for the Creation of a Special Tribunal for the Punishment of the Crime of Aggression against Ukraine,” March 2022, https://gordonandsarahbrown.com/wp-content/uploads/2022/03/Combined-Statement-and-Declaration.pdf; “Law Not War: A Special Tribunal for the Crime of Aggression,” UN Web TV, October 25, 2022, https://media.un.org/en/asset/k1q/k1qyewjw26. For an analysis of the proposed tribunal, see Olivier Corten, Vaios Koutroulis, “Tribunal for the Crime of Aggression against Ukraine – a Legal Assessment,” European Parliament, December 2022, https://www.europarl.europa.eu/RegData/etudes/IDAN/2022/702574/EXPO_IDA(2022)702574_EN.pdf.
[321] ICRC, “What is International Humanitarian Law?,” July 2004, https://www.icrc.org/en/doc/assets/files/other/what_is_ihl.pdf.
[322] An international armed conflict exists where the resort to armed force involves at least two States. See Geneva Conventions I, II, III, IV, Art. 2.
[323] Russia’s war on Ukraine is distinct from its status as the aggressor state (what is known as jus ad bellum, the law that regulates the conditions for initiating war or the use of armed force). Regardless of which party initiated a conflict, IHL also regulates the conduct of both parties in the conduct of the conflict itself (jus in bello).
[324] The four Geneva Conventions of 1949 have been ratified by 196 countries, including Russia and Ukraine, both of which also ratified Additional Protocol I of 1977.
[325] The Hague Convention of 1899 and The Hague Convention IV of 1907 and annexed regulations on the Laws and Customs of War on Land have been ratified by Russia and Ukraine. The two versions differ only slightly from each other. See ICRC, “Convention (IV) respecting the Laws and Customs of War on Land and its Annex,” access February 6, 2023, https://ihl-databases.icrc.org/en/ihl-treaties/hague-conv-iv-1907?activeTab=default.
[326] The Moscow Mechanism of the human dimension of the Organization for Security and Co-operation (OSCE) in Europe allows OSCE participating States to request investigations. The Moscow Mechanism was invoked by Ukraine and supported by 45 States on March 3, 2022. Its mandate is to establish the facts and circumstances concerning contraventions of OSCE commitments, violations and abuses of international human rights law and international humanitarian law, and establish the facts and circumstances of possible war crimes and crimes against humanity cases in the context of Russia’s full-scale invasion of Ukraine.
[327] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. i, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[328] Additional Protocol I, Art. 50 provides by reference that civilians are those who do not belong to the armed forces. In case of doubt, the person shall be considered civilian.
[329] Additional Protocol I, Art. 52 defines civilian objects as “objects which are not military objectives” and defines military objectives as “objects which by their nature, location, purpose or use make an effective contribution to military action and whose total or partial destruction, capture or neutralization, in the circumstances ruling at the time, offers a definite military advantage.” It further provides that in case of doubt, the object shall be considered civilian.
[330] International Committee of the Red Cross (ICRC), “Protocol Additional to the Geneva Conventions of 12 August 1949, and relating to the Protection of Victims of International Armed Conflicts,” June 8, 1977, 1125 UNTS 3 (Additional Protocol I), Art. 48; ICRC, Customary International Humanitarian Law, Rules 1, 7, accessed January 16, 2023, https://ihl-databases.icrc.org/en/customary-ihl/v1. Russia’s and Ukraine’s military manuals specifically provide for the principle of distinction. See ICRC, “Practice relating to Rule 7 (Russian Federation),” accessed January 16, 2023, https://ihl-databases.icrc.org/en/customary-ihl/v2/rule7?country=ru; see ICRC, “Practice relating to Rule 7 (Ukraine),” accessed January 16, 2023, https://ihl-databases.icrc.org/en/customary-ihl/v2/rule7?country=ua.
[331] Additional Protocol I, Art. 51(3); ICRC, Customary International Humanitarian Law, Rule 6.
[332] Cf Additional Protocol I, Art. 52(1), (2); ICRC, Customary International Humanitarian Law, Rule 10.
[333] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 27, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[334] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 27, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[335] Additional Protocol I, Art. 51(5)(b); ICRC, Customary International Humanitarian Law, Rule 14. See also ICRC, “Practice relating to Rule 14 (Russian Federation),” accessed January 16, 2023, https://ihl-databases.icrc.org/en/customary-ihl/v2/rule14?country=ru; ICRC, “Practice relating to Rule 14 (Ukraine),” accessed January 16, 2023, https://ihl-databases.icrc.org/en/customary-ihl/v2/rule14?country=ua.
[336] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 29, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[337] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 29, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[338] Additional Protocol I, Art. 57(1); ICRC, Customary International Humanitarian Law, Rule 15. See also ICRC, “Practice relating to Rule 15 (Russian Federation),” accessed January 16, 2023, https://ihl-databases.icrc.org/en/customary-ihl/v2/rule15?country=ru; ICRC, “Practice relating to Rule 15 (Ukraine),” accessed January 16, 2023, https://ihl-databases.icrc.org/en/customary-ihl/v2/rule15?country=ua.
[339] Additional Protocol I, Art. 57(2)(a)(i); ICRC, Customary International Humanitarian Law, Rule 16.
[340] Additional Protocol I, Art. 57(2)(c); ICRC, Customary International Humanitarian Law, Rule 20.
[341] Additional Protocol I, Art. 57(2)(b); ICRC, Customary International Humanitarian Law, Rule 19.
[342] Additional Protocol I, Art. 57(2)(a)(ii); ICRC, Customary International Humanitarian Law, Rule 18.
[343] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 30, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[344] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, pp. 30-31, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[345] Additional Protocol I, Arts. 8(c), 15; ICRC, Customary International Humanitarian Law, Rule 25. Medical personnel is defined as persons assigned, by a Party to the conflict, exclusively to the medical purposes or to the administration of medical units or to the operation or administration of medical transports, either permanently or temporarily.
[346] Additional Protocol I, Arts. 8(e), 12; ICRC, Customary International Humanitarian Law, Rule 28. Medical units are defined as establishments and other units, whether military or civilian, organized for medical purposes, be they fixed or mobile, permanent or temporary, including, for example, hospitals and other similar units, blood transfusion centers, medical depots and the medical and pharmaceutical stores of such units.
[347] Additional Protocol I, Arts. 8(f)-(j), 21; ICRC, Customary International Humanitarian Law, Rule 29. Medical vehicles are defined as means of transportation, whether military or civilian, permanent or temporary, assigned exclusively to medical transportation under the control of a competent authority of a party to the conflict, including means of transportation by land, water or air, such as ambulances, hospital ships and medical aircraft.
[348] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 36, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[349] See Geneva Convention IV, Arts. 18, 20; Additional protocol I, Arts. 12, 15, 21.
[350] “A Physician’s Ethical Responsibility to Provide Care During Times of War is Identical to That During Times of Peace,” Physicians for Human Rights, https://phr.org/issues/health-under-attack/medical-impartiality/.
[351] Additional Protocol I, Arts. 12, 13.
[352] See ICRC, Commentary of 1987 on Additional Protocol I, Art. 13, paras 565-68, https://ihl-databases.icrc.org/en/ihl-treaties/api-1977/article-13/commentary/1987?activeTab=undefined: The special protection afforded to hospitals and other medical units does not cease when it is guarded by pickets, sentries, or an escort made up of soldiers or civilian uniformed police force. The mere presence of guards shelters them from attacks as they have no offensive role to play and are only there to protect the sick and wounded.
[353] See ICRC, Commentary of 1987 on Additional Protocol I, Art. 13, paras 571-74, https://ihl-databases.icrc.org/en/ihl-treaties/api-1977/article-13/commentary/1987?activeTab=undefined.
[354] See ICRC, Commentary of 1987 on Additional Protocol I, Art. 13, para. 551, https://ihl-databases.icrc.org/en/ihl-treaties/api-1977/article-13/commentary/1987?activeTab=undefined.
[355] Additional protocol, Art. 13.
[356] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 36, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[357] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 37, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[358] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 37, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[359] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 37, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[360] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, pp. 8-9, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[361] Unlike war crimes, there is no comprehensive, universal treaty on crimes against humanity. Since its first authoritative articulation in the Charter of the Nuremberg International Military Tribunal, the concept of crimes against humanity has extensively developed outside treaty law and is rather a product of customary international law. See David Luban, “A Theory of Crimes against Humanity,” Georgetown University Law Center (2004), https://scholarship.law.georgetown.edu/facpub/146/. In 2019, the International Law Commission—a body of experts established by the United Nations General Assembly to develop international law and its codification—completed a set of proposed articles for a Convention on Crimes against Humanity. The project is currently under discussion. See Priya Pillai, “Draft Convention on Crimes against Humanity: A Window of Opportunity,” Opinio Juris, November 22, 2022, http://opiniojuris.org/2022/11/22/draft-convention-on-crimes-against-humanity-a-window-of-opportunity/.
[362] See Roger O’Keefe, International Criminal Law (Oxford University Press, 2017), pp. 137-145.
[363] See for instance Open Society Justice Initiative and TRIAL International, “Universal Jurisdiction Law and Practice in Germany”, Briefing Paper, March 2019, https://www.justiceinitiative.org/uploads/0b3c66af-68e0-4fd3-a8e0-d938a6e2b43b/universal-jurisdiction-law-and-practice-germany.pdf, 5-6 in relation to Section 7 VStGB; Open Society Justice Initiative and TRIAL International, “Universal Jurisdiction Law and Practice in Sweden”, Briefing Paper, April 2020, https://www.justiceinitiative.org/uploads/550b6548-a951-425f-84b3-d75e5d78688c/universal-jurisdiction-law-and-practice-sweden.pdf, 7, in relation to Section 2 of the UCA; Open Society Justice Initiative and TRIAL International, “Universal Jurisdiction Law and Practice in France”, Briefing Paper, February 2019, https://www.justiceinitiative.org/uploads/b264bc4f-053f-4e52-9bb8-fccc0a52816a/universal-jurisdiction-law-and-practice-france.pdf, 6 in relation to Article 212 of the French Criminal Code (FCC).
[364] See Rome Statute, Art. 7; Parliament of Ukraine, “Draft Law on Amendments to Certain Legislative Acts of Ukraine on the Implementation of International Criminal and Humanitarian Law,” accessed January 8, 2023, http://w1.c1.rada.gov.ua/pls/zweb2/webproc4_1?pf3511=67804; The Law of Ukraine “About Making Changes to Criminal Code of Ukraine and Code of Criminal Procedure of Ukraine,” April 14, 2022, https://itd.rada.gov.ua/billInfo/Bills/pubFile/1271913.
[365] A 2001 decision by the Constitutional Court of Ukraine found the Rome Statute to overall be in compliance with the Constitution of Ukraine, with the exception of provisions on complementarity. See Case N 1-35/2001, N 3-v/2001, Constitutional Court of Ukraine, July 11, 2001, https://zakon.rada.gov.ua/laws/show/v003v710-01#Text.
[366] See Embassy of Ukraine, No. 61219/35-673-384, April 9, 2014, https://www.icc-cpi.int/sites/default/files/itemsDocuments/997/declarationRecognitionJuristiction09-04-2014.pdf.
[367] ICC-OTP, The Prosecutor of the International Criminal Court, Fatou Bensouda, opens a preliminary examination in Ukraine, April 25, 2014, https://www.icc-cpi.int/news/prosecutor-international-criminal-court-fatou-bensouda-opens-preliminary-examination-ukraine.
[368] See Minister for Foreign Affairs of Ukraine, No. 145-VIII, September 8, 2015, https://www.icc-cpi.int/sites/default/files/iccdocs/other/Ukraine_Art_12-3_declaration_08092015.pdf#search=ukraine.
[369] ICC-OTP, ICC Prosecutor extends preliminary examination of the situation in Ukraine following second article 12(3) declaration, September 29, 2015, https://www.icc-cpi.int/news/icc-prosecutor-extends-preliminary-examination-situation-ukraine-following-second-article-123.
[370] ICC-OTP, “Report on Preliminary Examination Activities (2020),” December 2020, paras. 267-90, https://www.icc-cpi.int/sites/default/files/itemsDocuments/2020-PE/2020-pe-report-eng.pdf.
[371] See Parliament of Ukraine, “On Amendments to the Constitution of Ukraine (Regarding Justice), June 2, 2016, https://zakon.rada.gov.ua/laws/show/1401-19#Text. The amendment entered into force on September 30, 2016.
[372] ICC, “Situation in Ukraine (ICC-01/22), https://www.icc-cpi.int/ukraine. ICC, “Statement of ICC Prosecutor, Karim A.A. Khan QC, on the Situation in Ukraine: receipt of referral from 39 States Parties and the opening of an investigation,” March 2, 2022, https://www.icc-cpi.int/news/statement-icc-prosecutor-karim-aa-khan-qc-situation-ukraine-receipt-referrals-39-states.
[373] Rome Statute, Art. 8(2)(b)(xx), providing for the war crime of employing weapons, projectiles or materials or methods of warfare listed in the Annex to the Statute. The annex was never drafted. In the absence of such an Annex, the Elements of Crimes of the Rome Statute provide: “Elements will have to be drafted once weapons, projectiles or material or methods of warfare have been included in an annex to the Statute.” See also Knut Dörmann, “War Crimes under the Rome Statute of the International Criminal Court, with a Special Focus on the Negotiations on the Elements of Crimes” (Max Planck Yearbook of United Nations Law, Volume 7, 2003, 341-407), pp. 346-45, https://www.mpil.de/files/pdf3/mpunyb_doermann_7.pdf.
[374] Melanie O’Brien, “Russian Violations of IHL: The ICC is Not the Complete Answer,” Opinio Juris, March 18, 2022, https://opiniojuris.org/2022/03/18/russian-violations-of-ihl-the-icc-is-not-the-complete-answer: “There is a provision (Article 8(2)(b)(iii)) prohibiting attacks on against personnel and material (etc) involved in humanitarian assistance, however this only applies to those involved in a humanitarian assistance mission in accordance with the Charter of the United Nations, thus only providing protection to UN mandated missions and inapplicable to the Ukrainian conflict. The attack on humanitarian corridors could be prosecuted under the Rome Statute offence of directing attacks against the civilian population (Article 8(2)(b)(i)), but again, this would not fully capture the conduct in question, which is violating the sanctity of a specially created non-military zone.”
[375] Office of the Prosecutor of the International Criminal Court, “Policy Paper on Case Selection and Prioritisation,” September 15, 2016, p. 14, https://www.icc-cpi.int/sites/default/files/itemsDocuments/20160915_OTP-Policy_Case-Selection_Eng.pdf.
[376] Rome Statute, Arts. 15(4) and 53(1).
[377] ICC, Situation in the Republic of Cote d’Ivoire (ICC-02/11), Corrigendum to “Decision Pursuant to Article 15 of the Rome Statute on the Authorisation of an Investigation into the Situation in the Republic of Côte d’Ivoire,” November 15, 2011, paras. 23-25, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2011_18794.PDF.
[378] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Mbarushimana, Decision on the Confirmation of Charges (ICC-01/04-01/10), December 16, 2011, para. 94, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2011_22538.PDF.
[379] Rome Statue, Art. 8(1).
[380] ICC, Situation in the Central African Republic, Prosecutor v. Bemba Gombo (ICC-01/05-01/08), Decision Pursuant to Article 61(7)(a) and (b) of the Rome Statute on the Charges of the Prosecutor Against Jean-Pierre Bemba Gombo, June 15, 2009, para. 211, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2009_04528.PDF; ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Mbarushimana, Decision on the Confirmation of Charges (ICC-01/04-01/10), December 16, 2011, para. 94, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2011_22538.PDF. See also John J. Paust, “The International Criminal Court Does Not Have Complete Jurisdiction over Customary Crimes against Humanity and War Crimes,” 43 J. Marshall L. Rev. (2010) 603-713, p. 701, https://repository.law.uic.edu/cgi/viewcontent.cgi?article=1090&context=lawreview (“Under customary international law, war crimes do not have to be committed as part of a plan or policy or large-scale set of crimes and it would be illogical and not policy-serving to impose a limitation by interpreting the phrase “in particular” differently than its ordinary meaning.”).
[381] ICC, Situation in the Central African Republic, Prosecutor v. Bemba Gombo (ICC-01/05-01/08), Decision Pursuant to Article 61(7)(a) and (b) of the Rome Statute on the Charges of the Prosecutor Against Jean-Pierre Bemba Gombo, June 15, 2009, para. 211, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2009_04528.PDF.
[382] Rome Statute, Art. 7(2)(a).
[383] While the existence of a policy is relevant to both war crimes and CAH, in the case of crimes against humanity it is a “chapeau element,” meaning the existence of a policy must be established as a predicate to criminal liability. For war crimes, however, the existence of a plan or policy is not a jurisdictional requirement but serves as a guideline for the Court.
[384] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Katanga (ICC-01/04-01/07), Judgment pursuant to Article 74 of the Statute, March 7, 2014, para. 1110, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2015_04025.PDF.
[385] ICC, Situation in Kenya (ICC-01/09), Decision Pursuant to Article 15 of the Rome Statute on the Authorization of an Investigation into the Situation in the Republic of Kenya, March 31, 2010, para. 87, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2010_02409.PDF (quoting ICTY, Prosecutor v. Blaškić (Case No. IT-95-14-T), Judgement, March 3, 2000, para. 205, https://www.icty.org/x/cases/blaskic/tjug/en/bla-tj000303e.pdf).
[386] ICC, Situation in Kenya (ICC-01/09), Decision Pursuant to Article 15 of the Rome Statute on the Authorization of an Investigation into the Situation in the Republic of Kenya, March 31, 2010, para. 87, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2010_02409.PDF.
[387] ICTY, Prosecutor v. Blaškić (Case No. IT-95-14-T), Judgement, March 3, 2000, para. 205, https://www.icty.org/x/cases/blaskic/tjug/en/bla-tj000303e.pdf.
[388] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Katanga (ICC-01/04-01/07), Judgment pursuant to Article 74 of the Statute, March 7, 2014, para. 1109, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2015_04025.PDF.
[389] Relying on ICTY jurisprudence, the ICC considers that “an armed conflict exists whenever there is a resort to armed force between States or protracted violence between governmental authorities and organized armed groups or between such groups within a State.” ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Lubanga Dyilo (ICC-01/04-01/06), Judgment pursuant to Article 74 of the Statute, March 14, 2012, para. 533, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2012_03942.PDF.
[390] An international armed conflict is one that “takes place between two or more States.” ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Lubanga Dyilo (ICC-01/04-01/06), Judgment pursuant to Article 74 of the Statute, March 14, 2012, para. 541, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2012_03942.PDF. International armed conflicts also include military occupation, i.e. when it is actually placed under the authority of the hostile army, and this authority can be exercised. Elements of Crimes, fn. 34; ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Lubanga Dyilo (ICC-01/04-01/06), Decision on the Confirmation of Charges, January 29, 2007, para. 212, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2007_02360.PDF.
[391] Knut Dörmann, “War Crimes under the Rome Statute of the International Criminal Court, with a Special Focus on the Negotiations on the Elements of Crimes” (Max Planck Yearbook of United Nations Law, Volume 7, 2003, 341-407), pp. 362-63, https://www.mpil.de/files/pdf3/mpunyb_doermann_7.pdf.
[392] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Mbarushimana, Decision on the Confirmation of Charges (ICC-01/04-01/10), December 16, 2011, para. 94, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2011_22538.PDF.
[393] ICC, Situation in the Central African Republic, Prosecutor v. Bemba Gombo (ICC-01/05-01/08), Decision Pursuant to Article 61(7)(a) and (b) of the Rome Statute on the Charges of the Prosecutor Against Jean-Pierre Bemba Gombo, June 15, 2009, para. 211, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2009_04528.PDF.
[394] See ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Sentencing Judgment, November 7, 2019, para. 138, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_06674.PDF. Attacks against protected objects are considered by ICC jurisprudence as more grave than attacks against objects that are protected as regular civilian objects. ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Sentencing Judgment, November 7, 2019, para. 138, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_06674.PDF.
[395] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Sentencing Judgment, November 7, 2019, para. 138, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_06674.PDF.
[396] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Sentencing Judgment, November 7, 2019, para. 138, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_06674.PDF.
[397] See e.g. ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Judgment, July 8, 2019, para. 1147, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_03568.PDF (considering that the perpetrators referred to a health center as a dispensary sufficient to establish their awareness of its protected status).
[398] Intent can be inferred from various factors such as, for example, the means and methods used during the attack and the discriminatory nature of the attack. Elements of Crimes, General Introduction, para. 3. Cf ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Katanga (ICC-01/04-01/07), Judgment pursuant to Article 74 of the Statute, March 7, 2014, paras 807, 878 (in relation to intentional attacks against civilians), https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2015_04025.PDF.
[399] However, the protected object does not need to be the sole target of the attack: the crime would likely also be committed when the perpetrator launches the attack with two distinct specific aims – to target a military objective and simultaneously to target a protected object in the vicinity. Cf ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Katanga and Ngudjolo Chui (ICC-01/04-01/07), Decision on the Confirmation of Charges, September 30, 2008, paras 272-74 (in the context of showing attacks against the civilian population or individual civilians), https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2008_05172.PDF.
[400] Knut Dörmann, “War Crimes under the Rome Statute of the International Criminal Court, with a Special Focus on the Negotiations on the Elements of Crimes” (Max Planck Yearbook of United Nations Law, Volume 7, 2003, 341-407), pp. 380-81, https://www.mpil.de/files/pdf3/mpunyb_doermann_7.pdf.
[401] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Judgment, July 8, 2019, para. 1147, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_03568.PDF.
[402] Other acts that are not considered harmful to the enemy include: equipment of unit’s personnel with light individual weapons for personal defense or for that of the wounded and sick in their charge; guarding of the unit by a picket, by sentries or by an escort; presence in the units of small arms and ammunition taken from the wounded and sick, and not yet handed to the proper service. See Protocol Additional I, Art. 13(1).
[403] Cf ICTY, Prosecutor v. Prlić, Case No. IT-04-74-T, Judgement (TC), 29 May 2013, para 125, https://www.icty.org/x/cases/prlic/tjug/en/130529-1.pdf.
[404] “Interview with Dr. Alla Barsehian, UHC, December 17, 2022 (on-file).
[405] Igor Rozin, “Russia’s Most Devastating Sear, Ground, and Air Missiles,” Russia Beyond, November 7, 2017, https://www.rbth.com/science-and-tech/326642-russias-most-devastating-sea-ground.
[406] Information provided by weapons analyst (on-file).
[407] The occupation of Trostianets reportedly lasted from February 24 to March 26, 2022.
[408] Two tank commanders and one assistant were identified by Ukrainian prosecutors for their alleged role in the attack(s). See See Office of the Prosecutor General of Ukraine, “Another Russian serviceman who ordered to shell the Trostianetska hospital from a tank has been identified,” August 17, 2022, https://www.gp.gov.ua/ua/posts/vstanovleno-shhe-odnogo-viiskovosluzbovcya-rf-yakii-viddav-nakaz-obstrilyuvati-z-tanka-trostyanecku-likarnyu; State Bureau of Investigation of Ukraine, “The SBI Identified Russian Service Members who, with Tanks, were Firing at a Hospital in Trostyanets,” May 5, 2022, https://dbr.gov.ua/en/news/dbr-vstanovilo-vijskovosluzhbovciv-rf-yaki-z-tankiv-rozstrilyuvali-likarnyu-v-trostyanci.
[409] See ICRC, War Crimes under the Rome Statute of the International Criminal Court and their source in International Humanitarian Law – Comparative Table, October 31, 2012, https://www.icrc.org/en/document/war-crimes-under-rome-statute-international-criminal-court-and-their-source-international. See also Harmen van der Wilt, “Towards a Better Understanding of the Concept of ‘Indiscriminate Attack’ – How International Criminal Law Can be of Assistance,” Yearbook of International Humanitarian Law, 22 (2019), 29-42, https://pure.uva.nl/ws/files/59114194/Wilt2021_Chapter_TowardsABetterUnderstandingOfT.pdf.
[410] See Harmen van der Wilt, “Towards a Better Understanding of the Concept of ‘Indiscriminate Attack’ – How International Criminal Law Can be of Assistance,” Yearbook of International Humanitarian Law, 22 (2019) 29-42, p. 38, https://pure.uva.nl/ws/files/59114194/Wilt2021_Chapter_TowardsABetterUnderstandingOfT.pdf.
[411] Rome Statute, Art. 8(2)(b)(iv). According to the Elements of Crimes, the expression “concrete and direct overall military advantage” refers to a military advantage that is foreseeable by the perpetrator at the relevant time. Such advantage may or may not be temporally or geographically related to the object of the attack. In other words, the crime admits the possibility of lawful collateral damage provided it does not violate the law applicable in armed conflict, in line with the principle of proportionality. See Rome Statute, Elements of Crimes, fn. 36. In some instances, the use of indiscriminate weapons may reveal that the attack was directed at a protected object, especially where the damage caused is so great that it appears that the perpetrator meant to target it.
[412] Rome Statute, Elements of Crimes, fn. 37.
[413] Knut Dörmann, “War Crimes under the Rome Statute of the International Criminal Court, with a Special Focus on the Negotiations on the Elements of Crimes” (Max Planck Yearbook of United Nations Law, Volume 7, 2003, 341-407), p. 384, https://www.mpil.de/files/pdf3/mpunyb_doermann_7.pdf.
[414] On the night of March 2 to March 3, March 6, March 7, and March 8, 2022.
[415] See ICRC, Commentary of 1987 on Additional Protocol I, Art. 13, paras 571-74, https://ihl-databases.icrc.org/en/ihl-treaties/api-1977/article-13/commentary/1987?activeTab=undefined.
[416] See ICRC, Commentary of 1987 on Additional Protocol I, Art. 13, paras 565-68, https://ihl-databases.icrc.org/en/ihl-treaties/api-1977/article-13/commentary/1987?activeTab=undefined.
[417] Knut Dörmann, “War Crimes under the Rome Statute of the International Criminal Court, with a Special Focus on the Negotiations on the Elements of Crimes” (Max Planck Yearbook of United Nations Law, Volume 7, 2003, 341-407), pp. 380-81, https://www.mpil.de/files/pdf3/mpunyb_doermann_7.pdf.
[418] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Katanga (ICC-01/04-01/07), Judgment pursuant to Article 74 of the Statute, March 7, 2014, para. 905, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2015_04025.PDF; ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Judgment, July 8, 2019, para. 1028, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_03568.PDF; ICC, Situation in Uganda, Prosecutor v. Ongwen (ICC-02/04-01/15), Trial Judgment, February 4, 2021, para. 2763, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2021_01026.PDF.
[419] The “war crime of pillaging under Article 8(2)(b)(xvi) of the Statute requires that the property subject to the offence belongs to an ‘enemy’ or ‘hostile’ party to the conflict.” ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Katanga and Ngudjolo Chui (ICC-01/04-01/07), Decision on the Confirmation of Charges, September 30, 2008, para. 329, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2008_05172.PDF.
[420] “In the absence of the owner, or in coercive circumstances, the perpetrator’s knowledge of non-consent of the owner may be inferred.” See ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Judgment, July 8, 2019, para. 1028-29, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_03568.PDF.
[421] Appropriations justified by military necessity do not constitute the crime of pillaging, as any military necessity would require its use to be directed to further the war effort and thus use for military purposes. See Elements of Crimes, fn. 47; ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Ntaganda (ICC-01/04-02/06), Judgment, July 8, 2019, para. 1030, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2019_03568.PDF.
[422] In this regard, see Geneva Convention IV, Arts. 18, 21, 57.
[423] See Commentary on the Law of the International Criminal Court, Article 8(2)(b)(xvi), updated June 30, 2016, accessed January 6, 2023, https://cilrap-lexsitus.org/clicc/8-2-b-xvi/8-2-b-xvi.
[424] This exception must be interpreted narrowly. Only measures which are indispensable for securing the ends of the war and are lawful according to the modern law and usages of war are considered military necessity. ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Katanga (ICC-01/04-01/07), Judgment pursuant to Article 74 of the Statute, March 7, 2014, para. 894, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2015_04025.PDF.
[425] The crimes listed below are a non-exhaustive list of possible applicable Rome Statute provisions.
[426] Cf ICTY, Prosecutor v. Blaškić (Case No. IT-95-14-A), Judgement, July 29, 2004, para. 654, https://www.icty.org/x/cases/blaskic/acjug/en/bla-aj040729e.pdf.
[427] ICRC, Customary International Humanitarian Law, Rule 99, accessed January 16, 2023, https://ihl-databases.icrc.org/en/customary-ihl/v1.
[428] The definition of torture as a war crime, which requires that the victims be “protected persons” (as doctors and medics are), differs slightly from the definition of torture as a crime against humanity, which requires the victims to be in the custody of, or under the control of the perpetrator. See Rome Statute, Elements of Crimes, fn. 35. Further, unlike the definition of torture under the United Nations Convention against Torture, the Rome Statute does not require the perpetrator to hold the status of a public official or to have acted in an official capacity. Cf UN Convention against Torture, Art. 1.
[429] Rome Statute, Elements of Crimes, Art. 8(2)(a)(ii)-2.
[430] United Nations Human Rights Monitoring Mission in Ukraine, “Update on the Human Rights Situation in Ukraine (1 August – 31 October 2022), December 2, 2022, p. 4, https://www.ohchr.org/sites/default/files/documents/countries/ua/2022-12-02/HRMMU_Update_2022-12-02_EN.pdf.
[431] In this sense see “Armoury, Prison, Graveyard: Mariupol Regional Intensive Care Hospital under Russian occupation”, International Partnership for Human Rights, Truth Hounds, Global Diligence, November 2022, https://www.iphronline.org/wp-content/uploads/2022/11/Mariupol-report_for_distribution_final_1.pdf, pp. 28 – 31.
[432] Under the Elements of Crimes, the term “killed” is interchangeable with the term “caused death.”
[433] Protected persons include, among others: the wounded and sick, civilians in the power of the occupying party that are not nationals of the occupying power, and medical personnel. “Glossary: Protected Persons,” ICRC, accessed January 12, 2023, https://casebook.icrc.org/glossary/protected-persons. To be wounded or sick under IHL, two cumulative criteria have to be fulfilled: (1) a person must require medical care; and (2) he or she must refrain from any act of hostility. Additional Protocol I, Art. 8(a).
[434] See infra, “Overview and Impact of Attacks on Ukraine’s Health Care System.”
[435] Rome Statute, Arts. 7(1), 7(2)(a).
[436] Rome Statute, Art. 7(2)(a).
[437] ICTY, Prosecutor v. Blaškić (Case No. IT-95-14-T), Judgement, March 3, 2000, para. 205, https://www.icty.org/x/cases/blaskic/tjug/en/bla-tj000303e.pdf.
[438] ICC, Situation in Kenya (ICC-01/09), Decision Pursuant to Article 15 of the Rome Statute on the Authorization of an Investigation into the Situation in the Republic of Kenya, March 31, 2010, para. 87, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2010_02409.PDF
[439] Jeffrey Mankoff, “Russia’s War in Ukraine – Identity, History, and Conflict,” Center for Strategic & International Studies, April 2022, https://www.csis.org/analysis/russias-war-ukraine-identity-history-and-conflict
[440] For an in-depth analysis of Russia’s involvement in Crimea and Donbas between December 2013 and February 13, 2022, see Global Rights Compliance, “International Law and Defining Russia’s Involvement in Crimea and Donbas,” February 13, 2022, https://globalrightscompliance.com/wp-content/uploads/2022/05/International-Law-and-Russia-Involvement-in-Crimea-and-Donbas-1.pdf. See also Ukraine and the Netherlands v. Russia, No. 8019/16, 43800/14, 28525/20, ECHR (Grand Chamber), January 25, 2023 (finding that Russia exercised “effective control” on account of its military presence in eastern Ukraine and the decisive degree of influence it enjoyed over these areas as a result of its military, political and economic support to the “DPR” and the “LPR”).
[441] “Extracts from Putin’s Speech on Ukraine,” Reuters, February 21, 2022, https://www.reuters.com/world/europe/extracts-putins-speech-ukraine-2022-02-21/.
[442] Pjotr Sauer and Luke Harding, “Putin Annexes Four Regions of Ukraine in Major Escalation of Russia’s War,” The Guardian, September 30, 2022, https://www.theguardian.com/world/2022/sep/30/putin-russia-war-annexes-ukraine-regions.
[443] On December 13, 2022, the bill was considered by the State Duma and adopted in the first reading, with its submission for amendments due December 17, 2022. The draft law neither defines the concept of “interests of the Russian Federation” or territories, nor specifies the crimes to which it applies. At the time of publication of this report, amendments to the bill have not been published on the website of the State Duma. See Parliament of Russia, “Bill No. 246425-8 ‘On the Application of the Provisions of the Criminal Code of the Russian Federation and the Code of Criminal Procedure of the Russian Federation in the Territories of the Donetsk People’s Republic, the Lugansk People’s Republic, the Zaporozhskayaa oblast, the Khersonskaya oblast,” accessed January 16, 2023, https://sozd.duma.gov.ru/bill/246425-8. Bill No. 246425-8 and Explanatory Notes to Bill No. 246425-8 are on-file.
[444] “Russia’s War in Ukraine: Military and Intelligence Aspects,” Congressional Research Service, September 14, 2022, https://crsreports.congress.gov/product/pdf/R/R47068.
[445] Pablo Gutierrez et al., “Buildup, Bombing, Resistance: Mapping Russia’s Invasion of Ukraine,” The Guardian,March 17, 2022, https://www.theguardian.com/world/ng-interactive/2022/mar/17/russia-invasion-of-ukraine-maps-mapping-buildup-bombing; Andrew Roth et al., “Russia’s war in Ukraine: complete guide in maps, video and pictures,” The Guardian,May 15, 2022, https://www.theguardian.com/world/2022/mar/17/russias-war-in-ukraine-complete-guide-in-maps-video-and-pictures.
[446] “How Many Troops has Russia Sent into Invasion of Ukraine?,” AS English, February 26, 2022, https://en.as.com/en/2022/02/24/latest_news/1645729870_894320.html.
[447] Pjotr Sauer, “Vladimir Putin Signs Decree to Increase Size of Russian Armed Forces,” The Guardian, August 25, 2022, https://www.theguardian.com/world/2022/aug/25/vladimir-putin-signs-decree-increase-size-russian-armed-forces-ukraine.
[448] Office of the President of Russia, “Decree ‘On the announcement of partial mobilization in the Russian Federation,’” September 21, 2022, http://kremlin.ru/events/president/news/69391.
[449] Kateryna Stepanenko et al., “Russian Offensive Campaign Assessment, December 22,” December 22, 2022, https://www.criticalthreats.org/analysis/russian-offensive-campaign-assessment-december-22.
[450] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine (1 April – 25 June 2022),” July 11, 2022, p. 42, https://www.osce.org/files/f/documents/3/e/522616.pdf.
[451] These terms are disjunctive, not cumulative. See ICC, Situation in Kenya (ICC-01/09), Decision Pursuant to Article 15 of the Rome Statute on the Authorization of an Investigation into the Situation in the Republic of Kenya, March 31, 2010, para. 94, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2010_02409.PDF.
[452] ICC, Situation in Kenya (ICC-01/09), Decision Pursuant to Article 15 of the Rome Statute on the Authorization of an Investigation into the Situation in the Republic of Kenya, March 31, 2010, para. 95, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2010_02409.PDF.
[453] ICC, Situation in Kenya (ICC-01/09), Decision Pursuant to Article 15 of the Rome Statute on the Authorization of an Investigation into the Situation in the Republic of Kenya, March 31, 2010, para. 95, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2010_02409.PDF.
[454] ICC, Situation in Kenya (ICC-01/09), Decision Pursuant to Article 15 of the Rome Statute on the Authorization of an Investigation into the Situation in the Republic of Kenya, March 31, 2010, para. 96, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2010_02409.PDF.
[455] ICC, Situation in Kenya (ICC-01/09), Decision Pursuant to Article 15 of the Rome Statute on the Authorization of an Investigation into the Situation in the Republic of Kenya, March 31, 2010, para. 96, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2010_02409.PDF.
[456] See further, “Evidence of Widespread and Systematic Bombardment of Ukrainian Healthcare Facilities,” Yale School of Public Health – Humanitarian Research Lab, May 17, 2022, https://search.issuelab.org/resource/evidence-of-widespread-and-systematic-bombardment-of-ukrainian-healthcare-facilities.html: “Based on a review of nearly 300 facilities across five cities and regions, the HRL has concluded that Russia-aligned forces have engaged in widespread and systematic bombardment of Ukrainian healthcare facilities.”.
[457] ICC, Situation in the Democratic Republic of the Congo, Prosecutor v. Katanga and Ngudjolo Chui (ICC-01/04-01/07), Decision on the Confirmation of Charges, September 30, 2008, para. 448, https://www.icc-cpi.int/sites/default/files/CourtRecords/CR2008_05172.PDF.
[458] Sunčana Roksandić Vidlička, “Systemic Deprivation of Access to Essential Medicine and Medical Care – a Crime against Humanity?” (Koninklijke Brill NV, Leiden, 2021), pp. 159-61, https://doi.org/10.1163/9789004364424_008, noting that courts and tribunals have relied on the underlying offenses of persecution, enslavement, and other inhumane acts in relation to large-scale violations of economic, social, and cultural rights, including deprivation of medical care.
[459] Note that the case studies discussed above may give rise to other crimes against humanity qualifications, such as murder, imprisonment, and torture. See Rome Statute, Art. 7(1)(a), (e), (f), respectively.
[460] Organization for Security and Co-operation in Europe, “Report on Violations of International Humanitarian and Human Rights Law, War Crimes and Crimes against Humanity Committed in Ukraine since 24 February 2022,” April 22, 2022, p. 87, https://www.osce.org/files/f/documents/f/a/515868.pdf.
[461] Office of the Prosecutor General of Ukraine, “Statistics,” accessed January 23, 2023, https://www.gp.gov.ua/.
[462] Code of Criminal Procedure of Ukraine, Art. 214(1), https://zakon.rada.gov.ua/laws/show/4651-17#Text.
[463] For a comprehensive analysis of the application of IHL rules under Ukrainian law more generally, see Global Rights Compliance, “The Domestic Implementation of International Humanitarian Law in Ukraine (updated),” February 2021, https://www.asser.nl/media/794633/2021-the-domestic-implementation-of-ihl-in-ukraine-updated.pdf.
[464] Criminal Code of Ukraine, Law No. 2341-III of April 5, 2001, revised on December 29, 2022, https://zakon.rada.gov.ua/laws/show/2341-14?lang=en#Text.
[465] See Global Rights Compliance, “The Domestic Implementation of International Humanitarian Law in Ukraine (updated),” February 2021, https://www.asser.nl/media/794633/2021-the-domestic-implementation-of-ihl-in-ukraine-updated.pdf.
[466] See Parliament of Ukraine, “Draft Law on Amendments to Certain Legislative Acts of Ukraine on the Implementation of International Criminal and Humanitarian Law,” accessed January 8, 2023, http://w1.c1.rada.gov.ua/pls/zweb2/webproc4_1?pf3511=67804. For a comparative table of the amendments to the CCU proposed in Bill No. 2689, see: Parliamentarian for Global Action, “Bill No. 2689: Comparative Table to the Draft Law of Ukraine “On Amendments to Certain Legislative Acts on the Enforcement of International Criminal and Humanitarian Law,” accessed January 8, 2023, https://www.pgaction.org/pdf/2021/en-bill-2689-10-03-2021.pdf.
[467] The Law of Ukraine “About Making Changes to Criminal Code of Ukraine and Code of Criminal Procedure of Ukraine,” April 14, 2022, https://itd.rada.gov.ua/billInfo/Bills/pubFile/1271913.
[468] Parliamentarians for Global Action, “Parliament of Ukraine Adopts Bill to Implement International Criminal and Humanitarian Law,” May 20, 2021, https://www.pgaction.org/news/ukraine-bill-2689.html: “In the merits, Bill 2689 enshrines principles of international criminal law, including command responsibility; equips Ukraine with universal jurisdiction to effectively combat impunity even for acts without a link with Ukraine; includes provisions on crimes against humanity, otherwise missing in the legislation previously in force; and defines war crimes in conformity with the requirements of International Law.” See also Maria Zheltukha, “Conflict-Related Sexual Violence in Ukraine: Legislative Regulation,” Analytical Center JurFem, July 25, 2022, https://jurfem.com.ua/en/conflict-related-sexual-violence-in-ukraine-legislative-regulation/.
[469] See Center for Civil Liberties, “Euromaidan SOS: a New Government Bill No. 7290 Artificially Reduces Opportunities to Prosecute Russian Military Commanders and Civilian Superiors Liable for War Crimes,” April 20, 2022, https://ccl.org.ua/en/claims/euromaidan-sos-a-new-government-bill-%E2%84%96-7290-artificially-reduces-opportunities-to-prosecute-russian-military-commanders-and-civilian-superiors-liable-for-war-crimes/.
[470] See Parliament of Ukraine, “Draft Law on Amendments to the Criminal Code of Ukraine and the Criminal Procedure Code of Ukraine,” accessed January 8, 2023, http://w1.c1.rada.gov.ua/pls/zweb2/webproc4_1?pf3511=74105.
[471] Zmina, “Human Rights Defenders Recommend the Ukrainian Authorities to Finilize [sic] the Draft Law No 7290,” April 22, 2022, https://zmina.ua/en/statements-en/human-rights-defenders-recommend-the-ukrainian-authorities-to-finilize-the-draft-law-no-7290/. See also Center for Civil Liberties, “Euromaidan SOS: a New Government Bill No. 7290 Artificially Reduces Opportunities to Prosecute Russian Military Commanders and Civilian Superiors Liable for War Crimes,” April 20, 2022, https://ccl.org.ua/en/claims/euromaidan-sos-a-new-government-bill-%E2%84%96-7290-artificially-reduces-opportunities-to-prosecute-russian-military-commanders-and-civilian-superiors-liable-for-war-crimes/; Office of the High Commissioner for Human Rights, “Situation of Human Rights in Ukraine in the Context of the Armed Attack by the Russian Federation,” June 29, 2022, paras. 130-31, https://www.ohchr.org/sites/default/files/documents/countries/ua/2022-06-29/2022-06-UkraineArmedAttack-EN.pdf; T.M.C. Asser Institute and Global Rights Compliance, “MATRA-Ukraine: The Halfway Mark,” September 22, 2022, https://www.asser.nl/matra-ukraine/news-and-events/matra-ukraine-the-halfway-mark/. On command responsibility specifically, the text of Bill No. 7290 proposes to only criminalize “the omission of a commander, person acting as a commander or other superiors to terminate a war crime, crime of aggression, crime against humanity or genocide by a subordinate.” T.M.C. Asser Institute and Global Rights Compliance, “MATRA-Ukraine: The Halfway Mark,” September 22, 2022, https://www.asser.nl/matra-ukraine/news-and-events/matra-ukraine-the-halfway-mark/.
[472] Note that this section only analyzes provisions that are directly relevant to attacks against Ukraine’s health care system. For a comparative table identifying the relevant provisions of the CCU that are most relevant to a consideration of the propriety of pursuing war crimes or the lesser corresponding domestic crime, see Global Rights Compliance, “The Domestic Implementation of International Humanitarian Law in Ukraine (updated),” February 2021, Annex VIII, https://www.asser.nl/media/794633/2021-the-domestic-implementation-of-ihl-in-ukraine-updated.pdf.
[473] For an analysis of prosecution and adjudication of war crimes since the beginning of Russia’s invasion of Ukraine under Article 438 of the CCU, see e.g. Iryna Marchuk, “Domestic Accountability Efforts in Response to the Russia-Ukraine War,” Journal of International Criminal Justice, Volume 20, Issue 4, September 2022, https://doi.org/10.1093/jicj/mqac051. See also Ukrainian Legal Advisory Group, “‘The First Trial against the Russian Soldier’ as an Indicator of the State Justice System of Ukraine,” May 25, 2022, https://zmina.info/en/articles-en/the-first-trial-against-the-russian-soldier-as-an-indicator-of-the-state-justice-system-of-ukraine/.
[474] See State Bureau of Investigation of Ukraine, “The SBI Identified Russian Service Members who, with Tanks, were Firing at a Hospital in Trostyanets,” May 5, 2022, https://dbr.gov.ua/en/news/dbr-vstanovilo-vijskovosluzhbovciv-rf-yaki-z-tankiv-rozstrilyuvali-likarnyu-v-trostyanci; Office of the Prosecutor General of Ukraine, “Another Russian Serviceman who Ordered to Shell the Trostianetska Hospital from a Tank has been Identified,” August 17, 2022, https://www.gp.gov.ua/ua/posts/vstanovleno-shhe-odnogo-viiskovosluzbovcya-rf-yakii-viddav-nakaz-obstrilyuvati-z-tanka-trostyanecku-likarnyu; State Bureau of Investigation of Ukraine, “The SBI Put on the Wanted List the Russian Tankers who Shot the Local Hospital during the Occupation of Trostianets. The Repaired Tank ‘Takes Revenge’ on Former Owners for their Crimes,” October 24, 2022, https://dbr.gov.ua/en/news/dbr-ogolosilo-v-rozshuk-rosijskih-tankistiv-yaki-pid-chas-okupacii-trostyancya-rozstrilyali-miscevu-likarnyu.-vidremontovanij-tank-mstit-kolishnim-gospodaryam-za-zlochini.
[475] Global Rights Compliance a Foundation made up of lawyers and development experts, specialized in on-the-ground international humanitarian law and issues in conflict-affected and high-risk areas around the world, working to identify, prevent and mitigate adverse human rights impacts. See: https://globalrightscompliance.com/.
[476] Global Rights Compliance, “The Domestic Implementation of International Humanitarian Law in Ukraine (updated),” February 2021, p. 63, https://www.asser.nl/media/794633/2021-the-domestic-implementation-of-ihl-in-ukraine-updated.pdf.
[477] Additional Protocol I, Art. 51(4).
[478] Additional Protocol I, Art. 51(5)(b).
[479] Additional Protocol I, Arts. 12, 15, 21.
[480] Geneva Convention IV, Arts. 33, 147.
[481] Additional Protocol I, Art. 51(7).
[482] Geneva Convention IV, Art. 147.
[483] Additional Protocol I, Art. 75(2)(a).
[484] Additional Protocol I, Art. 75(2).
[485] ICRC, “War Crimes under the Rome Statute of the International Criminal Court and their source in International Humanitarian Law – Comparative Table,” October 31, 2012, https://www.icrc.org/en/document/war-crimes-under-rome-statute-international-criminal-court-and-their-source-international.
[486] Criminal Code of Ukraine, Arts. 185, 186.
[487] Criminal Code of Ukraine, Arts. 115, 127.
[488] Criminal Code of Ukraine, Art. 146.
[489] “What is Universal Jurisdiction,” TRIAL International, accessed January 6, 2023, https://trialinternational.org/topics-post/universal-jurisdiction/. It must be noted, however, that the exercise of universal jurisdiction varies around the world and depends on the country’s legislation. For example, several states have incorporated crimes contained in the Rome Statute in their national legislation and vested their courts with exercising the principle of universal jurisdiction. However, the definitions of the crimes may differ across different jurisdictions. For example, some countries may distinguish between war crimes committed in international armed conflicts and those committed in non-international armed conflicts, while others do not. Similarly, the requirements to exercise universal jurisdiction may also vary in different countries. For example, certain states condition the exercise of universal jurisdiction to the presence or residence of the alleged perpetrator on their territory or to the principle of double criminality, while others do not.
[490] Geneva Convention I, Art. 49; Geneva Convention II, Art. 50; Geneva Convention III, Art. 129; Geneva Convention IV, Art. 146.
[491] See Additional Protocol I, Art. 85(1).
[492] Convention Against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, 1465 UNTS 85, adopted on December 10, 1984, entered into force on June 26, 1987; International Convention for the Protection of All Persons from Enforced Disappearance, 2716 UNTS 3, adopted on December 20, 2006, entered into force on December 23, 2010.
[493] Elise Baker and Gissou Nia, “Attacks on Hospitals from Syria to Ukraine: Improving Prevention and Accountability Mechanisms,” Atlantic Council Issue Brief, 4, June 2022, https://www.atlanticcouncil.org/wp-content/uploads/2022/06/Attacks-on-Hospitals-from-Syria-to-Ukraine-Improving-Prevention-and-Accountability-Mechanisms.pdf. See also Anya Neistat, “Victims of war crimes in Ukraine have an unprecedented chance to seek justice”, The Guardian, July 24, 2022, https://www.theguardian.com/commentisfree/2022/jul/24/war-crimes-ukraine-investigations-justice, noting that cases can be brought under the universal jurisdiction principle in more than 150 countries.
[494] Mark Kersten, “Universal Jurisdiction in Ukraine: States should commit to using their own courts to address Russian atrocities”, Justice in Conflict, October 17, 2022, https://justiceinconflict.org/2022/10/17/universal-jurisdiction-in-ukraine-states-should-commit-to-using-their-own-courts-to-address-russian-atrocities/.
[495] See e.g. Open Society Justice Initiative and TRIAL International, “Universal Jurisdiction Law and Practice in the Netherlands,” Briefing Paper, April 2019, https://www.justiceinitiative.org/uploads/e91b3105-914b-415d-9067-54543fac7e36/universal-jurisdiction-law-and-practice-netherlands.pdf.
[496] See e.g. Open Society Justice Initiative and TRIAL International, “Universal Jurisdiction Law and Practice in the Netherlands,” Briefing Paper, April 2019, https://www.justiceinitiative.org/uploads/e91b3105-914b-415d-9067-54543fac7e36/universal-jurisdiction-law-and-practice-netherlands.pdf; Open Society Justice Initiative and TRIAL International, “Universal Jurisdiction Law and Practice in France,” Briefing Paper, February 2019, https://www.justiceinitiative.org/uploads/b264bc4f-053f-4e52-9bb8-fccc0a52816a/universal-jurisdiction-law-and-practice-france.pdf.
[497] See Parliamentarians for Global Action, “Implementation,” accessed January 27, 2023, https://www.pgaction.org/ilhr/rome-statute/implementation.html: Note that the definitions do not need to be verbatim but can also go beyond what the Rome Statute provides “to reflect more protective definitions that may exist under general international law or applicable treaties.” See e.g. Open Society Justice Initiative and TRIAL International, “Universal Jurisdiction Law and Practice in Germany,” Briefing Paper, March 2019, https://www.justiceinitiative.org/uploads/0b3c66af-68e0-4fd3-a8e0-d938a6e2b43b/universal-jurisdiction-law-and-practice-germany.pdf; Open Society Justice Initiative and TRIAL International, “Universal Jurisdiction Law and Practice in Sweden,” Briefing Paper, April 2020, https://www.justiceinitiative.org/uploads/550b6548-a951-425f-84b3-d75e5d78688c/universal-jurisdiction-law-and-practice-sweden.pdf.
[498] Mark Kersten, “Universal Jurisdiction in Ukraine: States should commit to using their own courts to address Russian atrocities”, Justice in Conflict, October 17, 2022, https://justiceinconflict.org/2022/10/17/universal-jurisdiction-in-ukraine-states-should-commit-to-using-their-own-courts-to-address-russian-atrocities/. These countries are Germany, Spain, Sweden, France, Lithuania, Canada, Poland, Estonia, Latvia, Slovakia, the United States, and the United Kingdom.
[499] Anya Neistat, “Victims of war crimes in Ukraine have an unprecedented chance to seek justice”, The Guardian, July 24, 2022, https://www.theguardian.com/commentisfree/2022/jul/24/war-crimes-ukraine-investigations-justice.
[500] See Leonard Rubenstein, Perilous Medicine – The Struggle to Protect Health Care from the Violence of War, Columbia University Press, 2021, p. 284.
[501] Lara Hakki, Eric Stover, and Rohini J. Haar, “Breaking the silence: Advocacy and accountability for attacks on hospitals in armed conflict,” International Review of the Red Cross (2021).
















